

Abstract
Anxiety sensitivity (AS) has been conceptualized as trait-like vulnerability and maintenance factor for PTSD. Although recent literature has demonstrated its malleability during treatment, few have examined its influence on and effect from PTSD treatment. Using multilevel regression analyses we examined: a) changes in AS during treatment, and b) whether pre-treatment AS predicted PTSD treatment response, in sample of female victims of interpersonal trauma receiving one of three treatments (Cognitive Processing Therapy, Cognitive Processing Therapy-Cognitive, and Written Accounts). Participants exhibited reductions in total ASI scores from pre- to post-treatment. Growth curve modeling revealed slightly different trajectories of PTSD symptoms as a function of pre-treatment AS, and overall decreases in PTSD symptoms during treatment were not associated with pretreatment AS. Pretreatment AS dimensions impacted PTSD total scores and symptoms clusters differentially. Clinical and theoretical implications for these results are discussed.
Keywords: Anxiety Sensitivity, Posttraumatic Stress Disorder, Treatment, Cognitive Therapy
1. Introduction
Anxiety sensitivity (AS) is the fear of anxiety-related sensations and their consequences (Reiss, Peterson, Gursky, & McNally, 1986). AS was originally conceptualized as a trait-like cognitive risk factor for the development of panic attacks and panic disorder (Maller & Reiss, 1992; Schmidt, Lerew, & Jackson, 1997). However, research on AS has demonstrated its critical role in a variety of psychiatric disorders including anxiety (Olatunji & Wolitzky-Taylor, 2009), mood (e.g., Cox, Enns, & Taylor, 2001; Zinbarg, Brown, Barlow, & Rapee, 2001), and alcohol use disorders (Schmidt, Zvolensky, & Maner, 2006), suggesting that it is a unifying and core component underlying many disorders. Although high levels of AS have been associated with a wide range of disorders, it has been shown to be particularly relevant to panic disorder and posttraumatic stress disorder (PTSD) as compared to other anxiety and mood disorders in a recent meta-analysis (Olatunji & Wolitzky-Taylor, 2009), likely due to the shared autonomic arousal component of these two disorders (Brown & McNiff, 2009).
Increased levels of AS are both retrospectively (Collimore, McCabe, Carleton, & Asmundson, 2008; Lang, Kennedy, & Stein, 2002; Stephenson, Valentiner, Kumpula, & Orcutt, 2009) and prospectively (Elwood, Mott, Williams, Lohr, & Schroeder, 2009; Feldner, Zvolensky, Schmidt, & Smith, 2008) related to greater PTSD symptom severity. Moreover, this association exists above and beyond other related constructs such as negative and positive affect (Fetzner, Collimore, Carleton, & Asmundson, 2012). Theoretically AS may be relevant for both the development and maintenance of PTSD. For example, individuals high in AS may be more sensitive to autonomic arousal experienced during a traumatic event, and, therefore, likely to react more strongly during the peritraumatic period. Additionally, individuals high in AS may be more likely to misinterpret symptoms of PTSD (e.g., physical arousal associated with reexperiencing symptoms) as dangerous (e.g., impending heart attack). This misinterpretation increases avoidance of situations that may evoke physical symptoms (e.g., trauma cues), further exacerbating and reinforcing their PTSD symptoms. To this end, a longitudinal study of physical trauma survivors who were assessed shortly after injury, 6-months, and 12-months later, found that AS predicted future PTSD symptom severity and vice versa (Marshall, Miles, & Stewart, 2010), lending further support to the notion that AS may serve a maintaining role in the course of PTSD.
The latent structure of AS has been debated in the literature. AS was initially conceptualized as a dimensional construct (Taylor, Rabian, & Fedoroff, 1999), however, there remains an ongoing, unresolved debate regarding the latent structure of AS, with some arguing for a categorical or mixed categorical-dimensional structure, representing two forms of AS, pathological and normative (e.g., Bernstein, Zvolensky, Weems, Stickle, & Leen-Feldner, 2005) and others (e.g., Broman-Fulks et al., 2010) arguing for a dimensional model as originally conceptualized. Generally, research has largely been driven by the notion of dimensionality and the assumption that one experiences and expresses AS along a continuum (e.g., Bronman-Fulks, Berman, Rabian, & Webster, 2004; Gardenswartz, & Craske, 2001), and the dimensional structure has been found to serve as a better fit than a categorical latent structure (Broman-Fulks, et al., 2010).
Although AS is frequently examined as a unitary construct, its three dimensions (i.e., fear of somatic concerns, cognitive dyscontrol, and socially observable) may differentially influence PTSD. A recent study examining the different dimensions of AS on PTSD symptom clusters demonstrated that only the somatic concerns dimension significantly predicted PTSD total symptom severity, reexperiencing, and numbing symptoms, and that the somatic concerns and cognitive dyscontrol dimensions both significantly predicted PTSD hyperarousal symptoms (Fetzner et al., 2012). These findings suggest that the fear of the physical symptoms (e.g., “it scares me when my heart beats rapidly”) and their cognitive consequences (e.g, “when i am nervous, i worry that I might be mentally ill”), as opposed to the fear of publically observable symptoms (e.g., “it is important to me not to appear nervous”), may be driving the associations between AS and PTSD.
Previous research conceptualized AS as a trait-like construct; however recent literature has demonstrated its malleability with treatment. As noted above, a growing body of literature has focused on the role of AS in many psychiatric disorders and has more recently demonstrated change in AS following treatment. A recent meta-analysis examined change in AS during the course of cognitive behavioral therapy (CBT), which included cognitive therapy alone and exposure therapy alone, in 16 treatment studies and 8 prevention studies for at risk individuals for panic disorder, social anxiety disorder, claustrophobia, and tinnitus (Smits, Berry, Tart, & Powers, 2008). Results indicated that CBT was efficacious at reducing AS during treatment. Notably, there were no studies of PTSD included in this meta-analysis.
There are initial data offering promising results for a similar pattern of reductions in AS over the course of trauma-focused treatment. Given the research demonstrating the role of AS in PTSD, some have argued that a treatment approach that focuses on interoceptive exposures (i.e., purposely eliciting physiological arousal) and trauma-related exposure therapy, without any focus on cognitive restructuring, may improve symptoms of PTSD more effectively (e.g., Taylor, 2003). Furthermore, it is suggested that interoceptive exposure, which explicitly targets the physiological symptoms of PTSD, preceding trauma-focused treatment may result in more efficacious trauma-focused treatment (Taylor, 2003). Notably, the interoceptive component of treatment is similar to anxiety sensitivity reduction protocols, (e.g., Keough & Schmidt, 2012; Schmidt et al., 2007; Vujanovic, Bernstein, Berenz, & Zvolensky, 2012) that include interoceptive exposure to reduce AS and related symptoms. Findings from Vujanovic and colleagues (2012) suggest that theoretically, changes in AS maybe be useful in improving outcomes in trauma-exposed adults.
Despite the focus on AS and PTSD and the emergence of AS reduction protocols, only one PTSD treatment outcome study, to our knowledge, has directly examined the impact of trauma-focused treatment on reductions in AS. A small CBT group treatment for PTSD related to motor vehicle accidents (MVA) demonstrated that AS was a predictor of PTSD symptoms, but not MVA related beliefs, despite the fact that the CBT targeted driving related beliefs (Fedroff, Taylor, Asmundson, & Koch, 2000). Moreover, a decrease in AS pre- to post-treatment significantly predicted reductions in PTSD above and beyond pain severity and MVA related beliefs, suggesting that AS is a significant cognitive risk factor for exacerbating and maintaining symptoms of PTSD. However, no study has directly examined whether AS has a direct influence on treatment response.
Given that the role of AS in treatment for PTSD remains understudied, the goals of the current study were to examine whether: a) AS decreases with PTSD treatment in a sample of female victims of interpersonal trauma; and b) AS at baseline predicts change over time in PTSD symptoms. To better characterize these associations, we examined AS and PTSD total scores, as well as different dimensions of AS and PTSD symptom clusters. With regard to our first aim, we predicted that AS would decrease across treatment despite the inherently different sample used in the current study. Although exploratory in nature, we also hypothesized that decreases in AS scores, particularly the physical and cognitive subscales, would predict decreases in PTSD symptoms across clusters given previous research demonstrating the unique relevance of these subscales to PTSD symptoms (Fetzner et al., 2012). Our secondary aim was exploratory in nature. AS has been validated as both a risk and maintaining factor for PTSD, yet it has not been studied in conjunction with PTSD treatment from a longitudinal perspective. Moreover, there are little data to suggest how elevated levels of AS might impact treatment response.
2. Methods
2.1 Participants
Participants were female interpersonal trauma victims with PTSD who enrolled in a dismantling study of cognitive processing therapy in which the full protocol of cognitive processing therapy (CPT) was compared with its components, cognitive therapy only (CPT-C) and written accounts (WA), for the treatment of PTSD and comorbid symptoms (Resick et al., 2008). Of the original sample, 70 participants (25 CPT, 20 WA, 25 CT) completed the Anxiety Sensitivity Index (ASI) pre- and post-treatment.
Because we used multilevel regression analysis, which is efficient in dealing with missing data, our analysis examining change over time in ASI included the 70 participants who had ASI scores at pre-treatment, post-treatment, or both assessments. This sample (n=70) had a mean age of 34.52 (SD = 12.68), and a mean of 14.25 (SD = 2.66) years of education. The sample was 61 % Caucasian, 34% African American, and 5 % other races. With respect to relationship status, 19% identified as being married, 19% as divorcees, 53 % single, and the remaining (9%) as separated, widowed, or living with someone. Twelve (4 CPT, 6 CPT-C, and 2 WA) of these participants only had post-treatment ASI scores and were excluded from the analyses examining pre-treatment ASI as a predictor of change in PTSD symptoms during treatment. A series of t-tests and chi-squared tests indicated that the 12 participants who did not have pre-treatment ASI scores did not significantly differ from participants who did on any of the above reported demographic variables and the outcome variables. Additionally, a chi-squared test confirmed that these 12 participants were equally distributed across treatment conditions, χ2 (2) = 1.57, n.s.
2.2 Measures
PTSD Diagnostic Scale (PDS; Foa, 1995)
The PDS is a 49-item self-report scale that assesses symptoms of PTSD according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM–IV; American Psychiatric Association, 1994) and trauma history. The PDS has demonstrated reliability and validity in diverse trauma groups (Foa, Cashman, Jaycox, & Perry, 1997). For these analyses, we used the PDS total frequency score, as well as the cluster scores. At pre-treatment, Cronbach’s αs were .82, .80, .56, .71, and .59 for the total PDS scale and the re-experiencing, avoidance, emotional numbing, and hyperarousal subscales, respectively.
Anxiety Sensitivity Index (ASI; Reiss et al., 1986)
The ASI is a 16-item, self-report measure of fear of experiencing anxiety symptoms. The ASI is measured on a 5-point Likert scale (0 = very little to 4 = very much) and has demonstrated adequate test-retest reliability (.71 – .75) and validity (Reiss et al. 1986), good internal reliability (a = .88; Peterson & Heilbronner, 1987). The total score has demonstrated good representation of a single factor structure (Reiss et al., 1986). The 3 subscales of the ASI (physical concerns, cognitive concerns, and social concerns) have demonstrated good reliability and validity (Zinbarg, Mohlman, & Hong, 1999) and were also used in the analyses. At pre-treatment, Cronbach’s αs were .92, .88, .77, and .62 for the total ASI scale and for the physical, social, and cognitive concerns subscales, respectively.
2.3 Procedure
Participants were recruited and participated in a brief telephone screen prior to being scheduled for an assessment. All participants signed consent to participate in the study and were made aware that they would not be included in the treatment portion of the study if they did not meet inclusion criteria or met any of the exclusion criteria. After the assessment confirmed eligibility, participants were randomly assigned to CPT, CPT-C, or WA as part of a randomized control trial. The treatments were conducted over 6-weeks and were equated for amount of time in session (i.e., 12 hours; see, Resick et al., 2008, for more information). If participants were unable to complete treatment within 12 weeks, treatment was terminated and the assessment occurred 2 weeks later no matter how much treatment they received. The PDS was administered once a week during treatment in addition to the pretreatment, posttreatment, and 6-month follow up visits. The ASI was administered to a subsample of women in the current study and was only administered at pretreatment and posttreatment. See Resick et al. (2008) for a detailed description of the original study.
3 Results
3.1 Data Analysis
We used Hierarchical Linear and Non-linear modeling (HLM6; Raudenbush, Bryk, & Congdon, 2004) to examine change over time in anxiety sensitivity and PTSD symptoms during treatment (Singer & Willett, 2003). A notable strength of multilevel regression is that it uses full information maximum likelihood estimation procedures. Therefore, all participants with at least one assessment (regardless of missing data at one or more time points) were included in the analyses. Multilevel regression is also very efficient and flexible providing multiple options for modeling change. Anxiety sensitivity was assessed on two occasions, pre- and post-treatment. To examine change in anxiety sensitivity, time was modeled using dummy coded variables (Cohen, Cohen, West, & Aiken, 2003) with time effects specified as fixed, producing multilevel models analogous to repeated measures ANOVAs. To assess treatment effects (i.e., treatment condition x time interactions), dummy-coded treatment variables were included as a Level-2 predictor of change over time. PTSD symptoms were assessed at nine occasions. Thus, we used multilevel growth curve modeling to specify change in PTSD symptoms and evaluate whether anxiety sensitivity at baseline impacted treatment outcome (i.e., anxiety sensitivity x time interactions) and whether the impact of anxiety sensitivity on treatment outcome varied as a function of treatment condition (i.e., treatment condition x anxiety sensitivity x time interactions). Cohen’s d (d) values are reported as estimates of effect size, and we adopted the convention of d = .25, .50, and .80 being indicative of small, medium, and large effect sizes, respectively.
3.2 Results
Table 1 depicts descriptive statistics and bivariate correlations among all variables at the baseline assessment. The mean of the baseline total ASI score was 30.15 (SD = 14.44), which is indicative of clinically significant levels of anxiety sensitivity. Total PDS and ASI scores were significantly correlated (r = .39) with reexperiencing and hyperarousal symptoms exhibiting the strongest associations with ASI total and subscale scores relative to avoidance and numbing symptoms.
Table 1.
Descriptive Statistics and Intercorrelations among Study Variables at Time 1
| Variable (n) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | M | SD |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. ASI- Total (58) | --- | 30.15 | 14.44 | ||||||||
| 2. ASI- Physical (58) | .95* | --- | 14.59 | 8.12 | |||||||
| 3. ASI-Mental (60) | .86* | .71* | --- | 6.67 | 4.33 | ||||||
| 4. ASI-Social (60) | .78* | .64* | .64* | --- | 7.67 | 2.65 | |||||
| 5. PDS- Total (70) | .39* | .37* | .43* | .35* | --- | 27.83 | 8.81 | ||||
| 6. PDS- Reexperiencing (70) | .38* | .41* | .37* | .28* | .76* | --- | 6.84 | 3.48 | |||
| 7. PDS- Avoidance (70) | .24 | .22 | .26* | .32* | .73* | .61* | --- | 3.84 | 1.70 | ||
| 8. PDS- Numbing (70) | .12 | .08 | .21 | .25 | .71* | .27* | .39* | --- | 4.86 | 2.40 | |
| 9. PDS- Hyperarousal (70) | .37* | .36* | .40* | .28* | .84* | .55* | .46* | .52* | --- | 9.53 | 3.11 |
Note.
p < .05;
M = mean; SD = Standard deviation; ASI = Anxiety Sensitivity Index; PDS = Posttraumatic Diagnostic Scale
Table 2 displays the results of the multilevel regression analyses examining change in anxiety sensitivity from pre- to post-treatment. Total ASI as well as each ASI subscale demonstrated statistically significant, large-effect size decreases from pre- to post-treatment. The magnitude of change was similar across ASI subscales. While the effect size for decrease in total ASI was noticeably larger for the WA condition compared to the other conditions, these differences did not reach statistical significance. However, the WA condition exhibited larger decreases in the physical subscale of the ASI compared to both the CPT (mean difference in change = 6.02, t = 2.42, p = .02, d = .71) and the CPT-C (mean difference in change = 5.51, t = 2.19, p = .03, d = .64) conditions (see Models 2a–2c in Table 2). No differences among treatment conditions approach statistical significance (largest d = .13) for the mental and social subscales.
Table 2.
Change in ASI from pre- to post-treatment
| Model | ASI Scale | Group | Pre-Treatment M (95% CI ) |
Post-Treatment M (95% CI ) |
Change M (95% CI ) |
Effect Size d (change) |
|---|---|---|---|---|---|---|
| ASI Total | ||||||
| 1 | Overall | 30.32 (26.72 to 33.92) | 20.63 (16.93 to 24.33) | −9.69 (−13.33 to −6.05) | −1.52* | |
| 1a | CPT | 29.66 (23.86 to 35.46) | 21.63 (15.52 to 27.73) | −8.03 (−13.99 to −2.08) | −0.80* | |
| 1b | CPT-C | 27.22 (21.22 to 33.22) | 19.76 (13.76 to 25.76) | −7.46 (−13. to 56 −1.36) | −0.71* | |
| 1c | WA | 34.45 (28.11 to 40.8) | 20.13 (13.06 to 27.19) | −14.33 (−21.07 to −7.58) | −1.26* | |
| ASI Physical Group | ||||||
| 2 | Overall | 14.35 (12.31 to 16.38) | 9.14 (7 to 11.28) | −5.2 (−7.36 to −3.04) | −1.39* | |
| 2a | CPT | 14.24 (10.93 to 17.56) | 10.94 (7.46 to 14.42) | −3.3 (−6.62 to 0.02) | −0.59*a | |
| 2b | CPT-C | 12.33 (8.91 to 15.76) | 8.52 (5.09 to 11.94) | −3.82 (−7.22 to −0.42) | −0.65*a | |
| 2c | WA | 16.62 (12.99 to 20.25) | 7.3 (3.27 to 11.32) | −9.32 (−13.08 to −5.56) | −1.47*b | |
| ASI Mental Group | ||||||
| 3 | Overall | 6.74 (5.71 to 7.77) | 4.13 (3.02 to 5.24) | −2.61 (−3.81 to −1.41) | −1.27* | |
| 3a | CPT | 6.74 (5.02 to 8.45) | 3.54 (1.72 to 5.36) | −3.2 (−5.17 to −1.22) | −0.94* | |
| 3b | CPT-C | 5.85 (4.13 to 7.57) | 3.81 (2.03 to 5.6) | −2.04 (−3.97 to −0.11) | −0.62* | |
| 3c | WA | 7.82 (5.95 to 9.69) | 5.31 (3.19 to 7.44) | −2.51 (−4.75 to −0.28) | −0.65* | |
| ASI Social Group | ||||||
| 4 | Overall | 7.61 (6.95 to 8.27) | 6.2 (5.5 to 6.89) | −1.41 (−2.06 to −0.76) | −1.28* | |
| 4a | CPT | 7.43 (6.32 to 8.54) | 5.98 (4.82 to 7.14) | −1.45 (−2.54 to −0.36) | −0.78* | |
| 4b | CPT-C | 7.57 (6.46 to 8.68) | 6.12 (4.98 to 7.27) | −1.45 (−2.51 to −0.38) | −0.81 | |
| 4c | WA | 7.88 (6.67 to 9.1) | 6.58 (5.24 to 7.92) | −1.30 (−2. to 53 −0.07) | −0.62 |
Note.
p < .05;
M = mean; SD = Standard deviation; CI = Confidence Interval; d = Cohen’s d (0.02 = small; 0.05 = medium; 0.08 = large); ASI = Anxiety Sensitivity Index; CPT = Cognitive Processing Therapy; CPT-C = Cognitive Processing Therapy-cognitive only ; WA = written accounts.
The next set of analyses examined pre-treatment ASI levels as a predictor of treatment response. Growth curve analyses with the nine PDS scores (pre-treatment, six during treatment, post-treatment, six-month follow-up) as outcomes were evaluated. A series of preliminary unconditional change models (i.e., examining change without predictor variables) revealed that a non-linear pattern of change modeling time with the assessment number (0–8) and assessment number squared fit the data best. This model produces three change parameters: a Level-1 intercept (initial status), and linear and quadratic change coefficients. We next added total ASI scores as a predictor of change in PDS. The coefficients for these analyses are presented in Table 3.
Table 3.
Growth Curve Models with Pre-treatment ASI Predicting Change in PDS
| Analysis | Coefficient/Predictor | Outcome | Level-1 Intercept (Initial Status) | Linear Change (Assessment #) | Quadratic Change (Assessment#2) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| b | t | d | b | t | d | b | t | d | |||
| Analysis 1 | |||||||||||
| Level-2 Intercept | PDS Total | 28.65* | 26.74 | 7.15 | −2.67* | −3.21 | −0.86 | 0.08 | 0.84 | 0.23 | |
| Total ASI | 0.22* | 2.69 | 0.72 | −0.13* | −2.35 | −0.63 | 0.01* | 2.23 | 0.60 | ||
| Analysis 2 | |||||||||||
| Level-2 Intercept | PDS Total | 28.69* | 36.12 | 9.74 | −2.62* | −3.18 | −0.86 | 0.08 | 0.79 | 0.21 | |
| Total ASI | 0.14* | 2.67 | 0.72 | −0.11* | −2.02 | −0.55 | 0.01a | 1.92 | 0.52 | ||
| TOTAL CAPS | 0.32* | 7.44 | 2.01 | −0.08 | −1.41 | −0.38 | 0.01 | 1.23 | 0.33 | ||
| Analysis 3a | |||||||||||
| Level-2 Intercept | PDS Total | 28.67* | 26.18 | 7.00 | −2.69* | −3.22 | −0.86 | 0.08 | 0.87 | 0.23 | |
| ASI Physical | 0.34* | 2.36 | 0.63 | −0.22 | −2.36 | −0.63 | 0.02* | 2.27 | 0.61 | ||
| Analysis 3b | |||||||||||
| Level-2 Intercept | PDS Total | 28.64* | 27.16 | 7.26 | −2.63* | −3.06 | −0.82 | 0.08 | 0.76 | 0.20 | |
| ASI Mental | 0.81* | 2.86 | 0.76 | −0.35* | −2.29 | −0.61 | 0.04* | 2.29 | 0.61 | ||
| Analysis 3c | |||||||||||
| Level-2 Intercept | PDS Total | 28.67* | 26.95 | 7.20 | −2.68* | −3.21 | −0.86 | 0.08 | 0.85 | 0.23 | |
| ASI Social | 1.29* | 2.82 | 0.75 | −0.73 | −1.53 | −0.41 | 0.07 | 1.25 | 0.33 | ||
| Analysis 4a | |||||||||||
| Level-2 Intercept | PDS Rex | 7.08* | 15.95 | 4.26 | −0.61* | −2.21 | −0.59 | 0.00 | 0.16 | 0.04 | |
| Total ASI | 0.08* | 2.47 | 0.66 | −0.02 | −1.33 | −0.35 | 0.00 | 1.12 | 0.30 | ||
| Analysis 4b | |||||||||||
| Level-2 Intercept | PDS Avd | 3.80* | 17.73 | 4.74 | −0.45* | −3.75 | −1.00 | 0.02 | 1.38 | 0.37 | |
| Total ASI | 0.02 | 1.59 | 0.42 | −0.02* | −2.10 | −0.56 | 0.002* | 2.11 | 0.56 | ||
| Analysis 4c | |||||||||||
| Level-2 Intercept | PDS En | 5.11* | 16.08 | 4.30 | −0.56* | −2.99 | −0.80 | 0.02 | 1.05 | 0.28 | |
| Total ASI | 0.03 | 1.06 | 0.28 | −0.03* | −2.58 | −0.69 | 0.004* | 2.34 | 0.63 | ||
| Analysis 4d | |||||||||||
| Level-2 Intercept | PDS HA | 9.83* | 26.91 | 7.19 | −1.11* | −4.55 | −1.22 | 0.07* | 2.30 | 0.61 | |
| Total ASI | 0.07* | 2.98 | 0.80 | −0.04* | −2.52 | −0.67 | 0.004* | 2.41 | 0.64 | ||
Note.
p < .05;
b = unstandardized regression; t = t statistic; d = Cohen’s d (0.02 = small; 0.05 = medium; 0.08 = large); ASI = Anxiety Sensitivity Index; PDS = Posttraumatic Diagnostic Scale.
ASI scores were mean-centered, therefore the Level-2 intercept can be interpreted as the change parameter at a mean level of ASI, with the ASI coefficient representing the impact of ASI scores on the change parameter. The Analysis 1 section of Table 3 shows that total pre-treatment ASI scores were significantly associated with all three change parameters. Figure 1 depicts PDS trajectories at 1SD above and below the mean and shows that participants reporting higher levels of pre-treatment ASI reported higher pre-treatment PDS scores (i.e., the positive association between ASI and initial status) and exhibited slightly larger decreases in PDS, such that there was no significant association between ASI and PDS at the follow-up assessment.1
Figure 1.
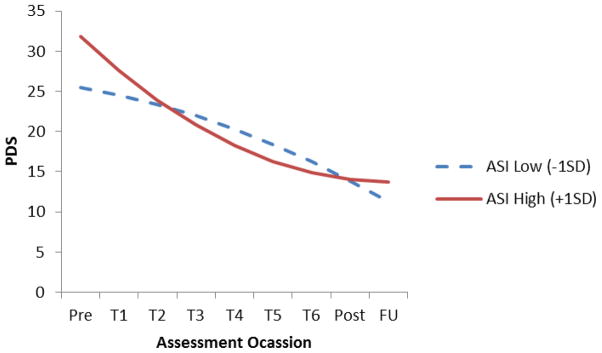
Change in PDS as function of pre-treatment
Therefore, higher levels of ASI are associated with higher initial PDS levels and larger decreases in PDS during treatment such that, by post-treatment, ASI was no longer associated with PDS. The Analysis 2 section of Table 3 depicts the results of a follow-up analysis conducted to evaluate the impact of ASI on change in PDS when controlling for initial PTSD symptom levels. To accomplish this, we added pre-treatment total CAPS severity scores as a Level-2 covariate predicting each change parameter. While the strengths of the associations were attenuated, the pattern of results remained the same. Total ASI score was significantly associated with the linear change parameter with the association between total ASI score and the quadratic coefficient approaching statistical significance (p = .06).
We next conducted a series of follow-up growth curve analyses to examine whether the three ASI subscales differentially predicted treatment outcome. The coefficients for these analyses are depicted in the Analysis 3a–3c sections of Table 3. In sum, total ASI, ASI-physical, and ASI-mental exhibited similar associations with change in PTSD, whereas ASI-social was not significantly associated with the linear or quadratic change coefficients.
We conducted one final set of follow-up analyses that examined whether the impact of ASI on PTSD trajectory varied across PTSD symptom clusters. The Analysis 4a-4d sections of Table 3 presents the coefficients from these analyses. The most notable finding to emerge from these follow-up analyses is that total ASI scores predicted change in each of the PTSD symptom clusters with the exception of re-experiencing symptoms.
4. Discussion
To our knowledge, this study is the first to demonstrate a decrease in AS with PTSD treatment in females with interpersonal trauma. Moreover, reductions in AS were seen following treatment conditions that did not explicitly focus on interoceptive exposures and two (CPT and CPT-C) of the three conditions were cognitively-focused treatment modalities. The WA condition demonstrated a significantly larger decrease in the physical symptom subscale of the ASI pre- to post-treatment, which is notably the first time the WA has demonstrated a slight advantage compared to CPT and CPT-C in symptom reduction (e.g., Resick et al., 2008; Resick, Suvak, Johnides, Mitchell, Iverson, 2012). The WA condition was exposure based, involving the repeated writing of a trauma account. Although by nature this may initiate an increase in physiological arousal, there were no specific interoceptive exposures involved in this therapy. Additionally, physical symptoms of anxiety were not specifically targeted in any other way in CPT, nor was the “meaning” of the anxiety. These findings provide initial support for the idea that the addition of interoceptive exposures to trauma focused treatment are not needed to see reductions in AS. The findings counter previous suggestions that the addition of interoceptive exposures to trauma focused protocols may be the most effective way to improve symptoms of PTSD (e.g., Taylor, 2003), given that individuals with PTSD would have higher levels of AS. Our findings suggest that individuals receiving trauma-focused treatment in the absence of interoceptive exposures have significant improvements in PTSD that are maintained through follow-up. Given evidence that changes in AS may improve outcomes in trauma exposure therapy (e.g., Vujanovic et al., 2012), it is not surprising that decreases in AS were related to decreases in PTSD in our study.
Another important finding is that high AS scores did not hinder PTSD treatment. This finding lends support for the idea that adding treatment targeting high levels of interoceptive sensitivity prior to PTSD treatment does not appear to be necessary. In fact, the current study showed no differences in end-state functioning based on where an individual started (high versus low) with respect to interoceptive sensitivity (i.e., high AS). Although CPT and Prolonged Exposure (PE) have demonstrated comparable results with regard to PTSD (Resick, Nishith, Weaver, Astin, & Feuer, 2002), clinicians often debate about whether a patient is a “better fit” for CPT or PE based on their interoceptive sensitivity. Our findings offer initial support that patients are not necessarily better suited for CPT or PE based on level of AS, and using interoceptive sensitivity to decide against a more cognitive treatment approach may not make a difference, as cognitive approaches successfully work with individuals high in AS.
Given that the current study did not include PE, the impact of PE on AS remains an empirical question that should be addressed in future research. However, given the literature that has consistently demonstrated that change in cognitions changes behaviors, and changes in behaviors results in cognition change (e.g., Hofmann, 2008; Newman, Hofmann, Trabert, Roth, & Taylor, 1994), it is not entirely surprising that a cognitively-based treatment would result in decreases in AS. Individuals high in AS have a tendency to assign catastrophic meaning to physiological symptoms, leading to an increased focus on them, which may in turn increase the experience of these symptoms. Therefore, cognitive treatments would presumably increase willingness to endure interoceptive sensitivity, even if it is not an explicit component of the treatment. Another possibility is that the psychoeducation component of these treatments may help normalize some of the anxiety symptoms and impact one’s willingness to experience interoceptive sensations.
We also found different trajectories of change in PTSD for individuals with high versus low AS. Given that individuals with higher levels of AS have more room to change during treatment, it is not entirely surprising that there would be different trajectories. However, the fact that individuals both high and low in AS exhibit similar PTSD symptom severity following treatment further demonstrates that: 1) having high AS does not hinder PTSD treatment, and 2) the addition of interoceptive exposures to facilitate the effectiveness of trauma focused treatment may not be necessary. However, future research is warranted to examine the potential benefits of interoceptive exposures in trauma-focused treatments.
The second aim of the study was to explore whether AS at baseline predicted change over time in PTSD symptoms, and if these changes differed by subscales of the ASI. We found that pretreatment AS impacted PTSD total scores and symptoms clusters differentially. Our findings demonstrated that AS total score predicted change in PTSD total scores, as well as for avoidance, numbing, and hyperarousal cluster scores. The absence of an effect on reexperiencing symptoms may be explained by a few lines of research. First is the idea that there are different types of reexperiencing symptoms that fall under the reexperiencing cluster (Brewin, Gregory, Lipton, & Burgess, 2010). For example, flashbacks are characterized by physical symptoms that accompany reliving the trauma, whereas frightening thoughts do not inherently occur with physical sensations. As a result, an individual could very well have symptoms that fall under the reexperiencing cluster that are unrelated to physiological symptoms. Second, the clusters of PTSD are distinct dimensions (e.g., Gootzeit & Markon, 2011), so even though the clusters of PTSD are related, they are inherently distinct. This may explain why the ASI relates to some clusters of PTSD and not reexperiencing. It is possible that in terms of external factors, the ASI may not be capturing symptoms that are inherently related to the reexperiencing cluster.
Although the current paper offers a new perspective on the relationship between AS and PTSD during the course of treatment, there are several limitations that should be considered. The sample in this study included women with interpersonal trauma, which limits the generalizability. Future studies would benefit from including men and women with a variety of traumas to better understand whether or not the relationship between AS and PTSD varies as a result of trauma type and/or gender. Another factor to consider is that the ASI was not given throughout treatment, leaving only two data points to examine AS. Given the recent evidence in support of the malleability of AS, having weekly measurements would provide additional insight into when these decreases are happening and if there is a specific component of the treatment that is most responsible for them. Additionally, there are psychometric limitations of the version of the ASI (Reiss et al., 1986) used in the study, which include concerns with items that may detract from construct validity (see Olatunki & Wolitzky-Taylor, 2009), that should be considered when interpreting these results. Given that it was previously thought that interoceptive exposures were responsible for decreases in AS, it would be important to better understand the mechanism responsible for this change in the absence of those exposures. Information about AS levels at follow-up would provide important information with respect to maintenance of both AS and PTSD gains. Both ASI and PTSD symptoms were assessed via self-report questionnaires, and thus shared method variance may account for some of the associations between these two variables. Future multi-method research is needed to assess and adjust for shared-method variance. Finally, it is important to investigate whether or not interoceptive exposures may further reduce levels of AS and how that may impact treatment response in PTSD. Although our posttreatment ASI scores are in the nonclinical range, the absence of a follow-up score limits information about the maintenance of changes in AS seen in the current study. Moreover, AS has been found to be associated with a wide range of disorders, and future studies would benefit from examining whether AS at baseline predicts change in other disorders that are comorbid with PTSD (e.g., depression).
In sum, this study demonstrated that AS is malleable in response to a primarily cognitive- focused PTSD treatment and that high levels of AS prior to treatment don’t hinder the effectiveness of the treatment itself. Literature supports the conceptualization of AS as a transdiagnostic mechanism underlying multiple disorders. Although PTSD treatment influences this mechanism, future research is needed to better understand how to target mechanisms of change within PTSD treatment. From a clinical perspective, these findings suggest that use of a cognitively-based treatment for PTSD (e.g., CPT or CPT-C) with individuals with high interoceptive sensitivity (e.g., high AS) should be given equal consideration when making treatment protocol decisions. Future studies examining the role of AS in cognitive therapy and exposure therapy would provide important information about the potential for a differential change in AS based on a primarily cognitive versus exposure therapy.
Highlights.
We examine changes in anxiety sensitivity (AS) during treatment.
We examine whether pre-treatment AS predicted PTSD treatment response.
AS reduces from pre- to post-treatment through different trajectories
Decreases in PTSD during treatment were not associated with pretreatment AS.
Pretreatment AS impacts PTSD total scores and symptoms clusters differentially.
Acknowledgments
This work was supported by National Institute of Mental Health Grant NIH-1 R01-MH51509 awarded to Patricia A. Resick while at the University of Missouri–St. Louis. This article was also supported by the National Center for PTSD, VA Boston Healthcare System. This study was partially supported by a National Institute of Mental Health grant (T32MH019836-15A2) awarded to Terence M. Keane.
Footnotes
Centering the time (assessment) variable such that zero represents the post-treatment assessment (i.e., assessment starts at −7 increases by one for each subsequent assessment) produces the same analysis but changes how the intercept is interpreted (now interpreted as post-treatment outcome levels). We conducted the analysis in this manner, which confirmed that ASI was not significantly associated with post-treatment PDS levels (b = .01, t = .10, p = .96, d = .02).
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: Author; 1994. [Google Scholar]
- Bernstein A, Zvolensky MJ, Weems C, Stickle T, Leen-Feldner EW. Taxonicity of anxiety sensitivity: An empirical test among youth. Behaviour Research and Therapy. 2005;43:1131–1155. doi: 10.1016/j.brat.2004.07.008. [DOI] [PubMed] [Google Scholar]
- Brewin CR, Gregory JD, Lipton M, Burgess N. Intrusive images in psychological disorders: characteristics, neural mechanisms, and treatment implications. Psychological Review. 2010;117(1):210–232. doi: 10.1037/a0018113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broman-Fulks JJ, Deacon BJ, Olatunji BO, Bondy CL, Abramowitz JS, Tolin DF. Categorical or dimensional: A reanalysis of the anxiety sensitivity construct. Behavior Therapy. 2010;41(2):154–171. doi: 10.1016/j.beth.2009.02.005. [DOI] [PubMed] [Google Scholar]
- Broman-Fulks JJ, Berman ME, Rabian B, Webster MJ. Effects of aerobic exercise on anxiety sensitivity. Behaviour Research and Therapy. 2004;42:125–136. doi: 10.1016/S0005-7967(03)00103-7. [DOI] [PubMed] [Google Scholar]
- Brown TA, McNiff J. Specificity of autonomic arousal to DSM-IV panic disorder and posttraumatic stress disorder. Behaviour Research and Therapy. 2009;47(6):487. doi: 10.1016/j.brat.2009.02.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, Aiken LS. Applied multiple regression/correlation analysis for the behavioral sciences. 2. Hillsdale, NJ: Lawrence Erlbaum; 2003. [Google Scholar]
- Collimore KC, McCabe RE, Carleton RN, Asmundson GJG. Media exposure and dimensions of anxiety sensitivity: Differential associations with PTSD symptom clusters. Journal of Anxiety Disorders. 2008;22(6):1021–1028. doi: 10.1016/j.janxdis.2007.11.002. [DOI] [PubMed] [Google Scholar]
- Cox BJ, Enns MW, Taylor S. The effect of rumination as a mediator of elevated anxiety sensitivity in major depression. Cognitive Therapy and Research. 2001;25(5):525–534. doi: 10.1023/A:1005580518671. [DOI] [Google Scholar]
- Elwood LS, Mott J, Williams NL, Lohr JM, Schroeder DA. Attributional style and anxiety sensitivity as maintenance factors of posttraumatic stress symptoms: A prospective examination of a diathesis stress model. Journal of Behavior Therapy and Experimental Psychiatry. 2009;40(4):544–557. doi: 10.1016/j.jbtep.2009.07.005. [DOI] [PubMed] [Google Scholar]
- Fedroff IC, Taylor S, Asmundson GJG, Koch WJ. Cognitive factors in traumatic stress reactions: Predicting PTSD symptoms from anxiety sensitivity and beliefs about harmful events. Behavioural and Cognitive Psychotherapy. 2000;28(01):5–15. [Google Scholar]
- Feldner MT, Zvolensky MJ, Schmidt NB, Smith RC. A prospective test of anxiety sensitivity as a moderator of the relation between gender and posttraumatic symptom maintenance among high anxiety sensitive young adults. Depression and Anxiety. 2008;25(3):190–199. doi: 10.1002/da.20281. [DOI] [PubMed] [Google Scholar]
- Fetzner MG, Collimore KC, Carleton RN, Asmundson GJG. Clarifying the relationship between AS dimensions and PTSD symptom clusters: are negative and positive affectivity theoretically relevant constructs? Cognitive Behaviour Therapy. 2012;41(1):15–25. doi: 10.1080/16506073.2011.621971. [DOI] [PubMed] [Google Scholar]
- Foa EB, Cashman L, Jaycox L, Perry K. The validation of a self-report measure of PTSD: The posttraumatic diagnostic scale. Psychological Assessment. 1997;4:445–451. [Google Scholar]
- Foa EB. Posttraumatic Stress Diagnostic Scale (manual) Minneapolis, MN: National Computer Systems; 1995. [Google Scholar]
- Gardenswartz CA, Craske MG. Prevention of panic disor-der. Behavior Therapy. 2001;32:725–737. [Google Scholar]
- Gootzeit J, Markon K. Factors of PTSD: Differential specificity and external correlates. Clinical Psychology Review. 2011;31(6):993–1003. doi: 10.1016/j.cpr.2011.06.005. [DOI] [PubMed] [Google Scholar]
- Hofmann SG. Cognitive processes during fear acquisition and extinction in animals and humans: implications for exposure therapy of anxiety disorders. Clinical Psychology Review. 2008;28(2):199–210. doi: 10.1016/j.cpr.2007.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keough ME, Schmidt NB. Refinement of a brief anxiety sensitivity reduction intervention. Journal of Consulting and Clinical Psychology. 2012;80(5):766–772. doi: 10.1037/a0027961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lang AJ, Kennedy CM, Stein MB. Anxiety sensitivity and PTSD among female victims of intimate partner violence. Depression and Anxiety. 2002;16(2):77–83. doi: 10.1002/da.10062. doi:10.1002/da.10062. [DOI] [PubMed] [Google Scholar]
- Maller RG, Reiss S. Anxiety sensitivity in 1984 and panic attacks in 1987. Journal of Anxiety Disorders. 1992;6(3):241–247. doi:org/10.1016/0887-6185(92)90036-7. [Google Scholar]
- Marshall GN, Miles JNV, Stewart SH. Anxiety sensitivity and PTSD symptom severity are reciprocally related: Evidence from a longitudinal study of physical trauma survivors. Journal of Abnormal Psychology. 2010;119(1):143. doi: 10.1037/a0018009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newman MG, Hofmann SG, Trabert W, Roth WT, Taylor CB. Does behavioral treatment of social phobia lead to cognitive changes? Behavior Therapy. 1994;25(3):503–517. doi: 10.1016/S0005-7894(05)80160-1. [DOI] [Google Scholar]
- Olatunji BO, Wolitzky-Taylor KB. Anxiety Sensitivity and the Anxiety Disorders: A Meta-Analytic Review and Synthesis. Psychological Bulletin. 2009;135(6):974–999. doi: 10.1037/a0017428. [DOI] [PubMed] [Google Scholar]
- Peterson RA, Heilbronner RL. The anxiety sensitivity index: construct validity and factor analytic structure. Journal of Anxiety Disorders. 1987;1:117–121. doi: 10.1016/0887-6185(87)90002-8. [DOI] [Google Scholar]
- Raudenbush SW, Bryk AS, Congdon R. HLM 6 for Windows [computer software] Skokie, IL: Scientific Software International, Inc; 2004. [Google Scholar]
- Reiss S, Peterson RA, Gursky DM, McNally RJ. Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behaviour Research and Therapy. 1986;24(1):1–8. doi: 10.1016/0005-7967(86)90143-9. doi:org/10.1016/0005-7967(86)90143-9. [DOI] [PubMed] [Google Scholar]
- Resick PA, Nishith P, Weaver TL, Astin MC, Feuer CA. A comparison of cognitive-processing therapy with prolonged exposure and a waiting condition for the treatment of chronic posttraumatic stress disorder in female rape victims. Journal of Consulting & Clinical Psychology. 2002;70(4):867–879. doi: 10.1037//0022-006x.70.4.867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resick PA, Galovski TE, Uhlmansiek MO, Scher CD, Clum G, Young-Xu Y. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence. Journal of Consulting & Clinical Psychology. 2008;76(2):243–258. doi: 10.1037/0022-006X.76.2.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resick PA, Suvak MK, Johnides BD, Mitchell KS, Iverson KM. The impact of dissociation on ptsd treatment with cognitive processing therapy. Depression and Anxiety. 2012;29(8):718–730. doi: 10.1002/da.21938. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Eggleston AM, Woolaway-Bickel K, Fitzpatrick KK, Vasey MW, Richey JA. Anxiety Sensitivity Amelioration Training (ASAT): a longitudinal primary prevention program targeting cognitive vulnerability. Journal of Anxiety Disorders. 2007;21(3):302–319. doi: 10.1016/j.janxdis.2006.06.002. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Lerew DR, Jackson RJ. The role of anxiety sensitivity in the pathogenesis of panic: Prospective evaluation of spontaneous panic attacks during acute stress. Journal of Abnormal Psychology. 1997;106(3):355–364. doi: 10.1037/0021-843X.106.3.355. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Zvolensky MJ, Maner JK. Anxiety sensitivity: Prospective prediction of panic attacks and Axis I pathology. Journal of Psychiatric Research. 2006;40(8):691–699. doi: 10.1016/j.jpsychires.2006.07.009. [DOI] [PubMed] [Google Scholar]
- Singer JD, Willett JB. Applied longitudinal data analysis: Modeling change and event occurrence. USA: Oxford University Press; 2003. [Google Scholar]
- Smits JAJ, Berry AC, Tart CD, Powers MB. The efficacy of cognitive-behavioral interventions for reducing anxiety sensitivity: A meta-analytic review. Behaviour Research and Therapy. 2008;46:1047–1054. doi: 10.1016/j.brat.2008.06.010. [DOI] [PubMed] [Google Scholar]
- Stephenson KL, Valentiner DP, Kumpula MJ, Orcutt HK. Anxiety sensitivity and posttrauma stress symptoms in female undergraduates following a campus shooting. Journal of Traumatic Stress. 2009;22(6):489–496. doi: 10.1002/jts.20457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor S, Rabian B, Federoff IC. Anxiety sensitivity: Problems, prospects, and challenges. In: Taylor S, editor. Anxiety sensitivity: Theory, research, and treatment of the fear of anxiety. Mahwah, NJ: Erlbaum; 1999. pp. 339–353. [Google Scholar]
- Taylor S. Anxiety sensitivity and its implications for understanding and treating PTSD. Journal of Cognitive Psychotherapy. 2003;17:179–186. [Google Scholar]
- Vujanovic AA, Bernstein A, Berenz EC, Zvolensky MJ. Single-session anxiety sensitivity reduction program for trauma-exposed adults: A case series documenting feasibility and initial efficacy. Behavior Therapy. 2012 doi: 10.1016/j.beth.2012.03.005. [DOI] [PubMed] [Google Scholar]
- Zinbarg RE, Brown TA, Barlow DH, Rapee RM. Anxiety sensitivity, panic, and depressed mood: A reanalysis teasing apart the contributions of the two levels in the hierarchical structure of the Anxiety Sensitivity Index. Journal of Abnormal Psychology. 2001;110(3):372. doi: 10.1037/0021-843X.110.3.372. [DOI] [PubMed] [Google Scholar]
- Zinbarg RE, Mohlman J, Hong NN. Dimensions of anxiety sensitivity. In: Taylor S, editor. Anxiety sensitivity: Theory, research, and treatment of the fear of anxiety. The LEA series in personality and clinical psychology. Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 1999. pp. 83–114. [Google Scholar]