

Abstract
The pericardial lipomas are rare benign cardiac tumors. The clinical presentation of these cardiac neoplasms varies according to the site of growth. We describe here a case of massive intrapericardial lipoma leading to severe dyspnea, its diagnostic work up and briefly review the existing literature of this uncommon disorder. The patient underwent successful surgical resection of the tumor with complete alleviation of the symptoms.
Keywords: Pericardial lipoma, CECT thorax, Cardiac tumour
1. Introduction
Primary cardiac tumors represent a constellation of uncommon neoplasms with an autopsy incidence of 0.0017–0.056%.1 Cardiac lipomas are uncommon benign cardiac tumours and constitute approximately 10% of all neoplasms of the heart. Usually these tumors are discovered incidentally at the time of cardiac surgery or autopsy, but rarely they may produce symptoms because of compression of cardiac chambers or lung tissue and can lead to life threatening complications.
2. Case report
A 50-year old female with no conventional risk factors presented to us with the one and half year history of gradually progressive dyspnea (NYHA class-III). On examination, the patient had pulse rate of 80/min, blood pressure of 90/60 mm of Hg and fall of systolic BP of 14 mm Hg with inspiration. She had elevated jugular venous pressure (7 cm of H2O) with absent Kussmaul's sign and normal heart sounds. The chest examination revealed decreased breath sounds at the right lung base and rest of the systemic examination was unremarkable. ECG of the patient showed no significant changes. The chest radiograph anteroposterior view revealed large right lower lung field opacity in continuation with the right heart border with normal pulmonary vasculature (Fig. 1A). Right lateral radiograph showed well circumscribed radio opacity growing in retrosternal space overlying cardiac silhouette (Fig. 1B). 2D transthoracic echocardiography showed relative echolucent shadow occupying pericardial space with compression of right side of the heart (Fig. 2) leading to diastolic collapse of right atrium (RA) and right ventricle (RV) associated with dilated hepatic veins and inferior vena cava. The patient had mild tricuspid regurgitation with no other valvular dysfunction with normal left ventricular systolic function. CECT scan of thorax confirmed the presence of a huge intrapericardial homogenous mass measuring 10 × 11.5 cm, extending into right lung field with marked loss of lung volume with no direct infiltration of heart and great vessels (Fig. 3A). The mass had similar signal intensity as fat (Fig. 3B) and there was no associated lymphadenopathy. The pulmonary function tests showed significant compromise of the lung volumes. The arterial blood gas analysis revealed hypoxemia (PO2 – 65 mm Hg) with normal pH. CT guided FNAC from the mass revealed presence of mature adipocytes. The cardiac catheterization revealed elevated intracardiac filling pressures (Mean RA pressure – 10 mm of Hg, RV end diastolic pressure – 14 mm Hg, PCWP – 16 mm Hg, LV end diastolic pressure – 18 mm Hg) and normal coronary arteries. The patient was referred for surgical excision of the tumor, where a large mass growing in pericardial space was confirmed and successfully removed. Histopathological evaluation of the mass confirmed the diagnosis as benign lipoma (Fig. 4). Subsequently, she had uneventful recovery and discharged in a stable condition.
Fig. 1.
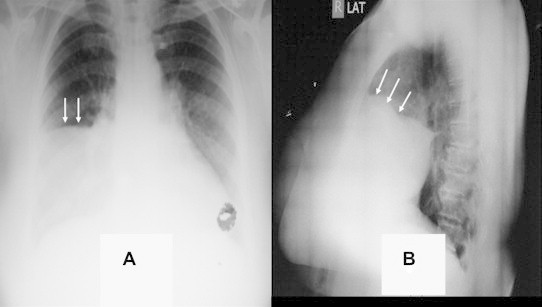
(A) Chest roentgenogram PA view showing large radio opacity in right lower lung field in continuation with right heart border (white arrows), (B) right lateral view showing radio opacity in retrosternal space overlying cardiac shadow (white arrows).
Fig. 2.
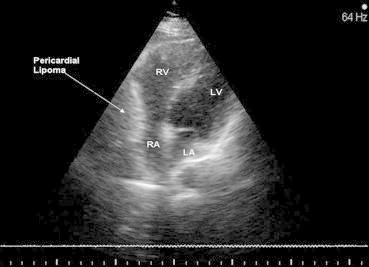
Two dimensional transthoracic echocardiography in apical four chamber view showing relative echolucency in pericardial space with compression of the right atrium and right ventricle.
Fig. 3.
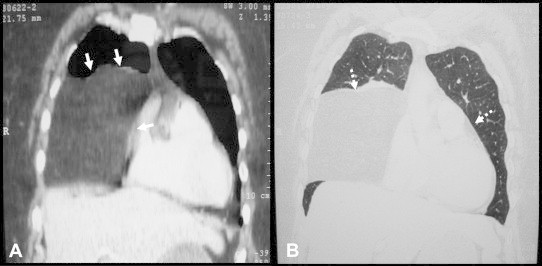
(A) CECT thorax showing 10 × 11.5 cm mass with extension into right lung field and compressing over right side of the heart (white arrows) (B) Mass having similar signal intensity as pericardial fat (White dashed arrows).
Fig. 4.
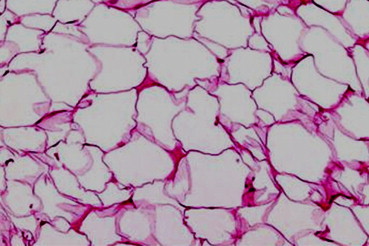
Histopathological evaluation of the resected mass showing presence of mature adipocytes (100× magnification).
3. Discussion
Cardiac lipomas are least common benign cardiac tumors which may develop intracardiac or in subpericardial space.2 These tumors can be part of the diffuse lipomatosis or isolated neoplasms. Intrapericardial lipomas usually remain indolent for many years and signs and symptoms depend on the speed of tumor growth, location and extent of the tumor. Massive pericardial lipomas may cause dyspnea either due to loss of lung volume or elevation of ventricular filling pressures.2 Other presenting features can be fatigue, chest pain3 possibly by compression of coronary arteries or due to outward strech of pericardium, and rarely arrhythmias.4 The intracavitary lipomas may present as congestive heart failure, syncope or sudden cardiac death. The physical findings usually remain subtle even in large tumors.
Chest X-rays of these tumors are often interpreted as, herniated liver, large atrial appendage with thrombus, primary hilar neoplasm, sequestration of a lobe of the liver, diaphragmatic hernia, or a mediastinal mass. Transthoracic echocardiography is the usual initial investigation in the detection of pericardial lipomas. Intrapericardial lipomas are commonly relative echolucent structures just opposed to intracavitary lipomas which have echodense appearance. The pericardial lipomas may be incorrectly diagnosed as loculated pericardial fluid. CT scan and magnetic resonance imaging are primary investigations in delineation and differentiation of these tumors and precisely define topography and relation of vessels to the tumor growth.5 Coronary angiography may be an ancillary investigation, as in some cases, tumor may have its blood supply originating from one of the coronaries. Surgical excision of the tumor with pedicle is usually successful with low complications and very low recurrence rates.6
There are few sporadic case descriptions of large pericardial lipomas in the literature that vindicates rarity of this condition. In summary, massive subpericardial lipomas are uncommon cardiac neoplasms which should be considered in the differential diagnosis of mediastinal radio opacities on chest roentgenogram and resection is the rule, even in asymptomatic masses, to prevent the compression syndromes.
Conflicts of interest
All authors have none to declare.
References
- 1.Lam K.Y., Dickens P., Chan A.C. Tumors of the heart. A 20 year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med. 1993;117:1027–1031. [PubMed] [Google Scholar]
- 2.Doshi S., Halim M., Singh H., Patel R. Massive intrapericardial lipoma, a rare cause of breathlessness. Investigations and management. Int J Cardiol. 1998;66:211–215. doi: 10.1016/s0167-5273(98)00221-6. [DOI] [PubMed] [Google Scholar]
- 3.Rafel J., Pujadas R., Batalla N. Cardiac lipoma presenting as angina. Rev Esp Cardiol. 2004;57:884. [PubMed] [Google Scholar]
- 4.Cooper M.J., deLorinier A.A., Higgins C.B., Van Hare G.F., Enderlein M.A. Atrial flutter-fibrillation resulting from left atrial compression by an intrapericardial lipoma. Am Heart J. 1994;127:950–951. doi: 10.1016/0002-8703(94)90573-8. [DOI] [PubMed] [Google Scholar]
- 5.Hananouchi G.I., Goff W.B. Cardiac lipoma: 6 year follow up with MRI characteristics, and a review of literature. Magn Reson Imaging. 1990;8:825–828. doi: 10.1016/0730-725x(90)90021-s. [DOI] [PubMed] [Google Scholar]
- 6.Botta L., Amore A., Pirini M.G., Andrea A., Mastrorilli M., Mikus P.M. Intrapericardial lipoma: successful resection of a giant tumor without cardiopulmonary bypass. Cardiovasc Pathol. 2007;16:122–124. doi: 10.1016/j.carpath.2006.09.009. [DOI] [PubMed] [Google Scholar]