

Abstract
A young male following road traffic accident (RTA) with head injury and parietal bleed was diagnosed with STEMI based on ECG findings which is rare occurrence. Coronary angiography showed thrombotic ostial occlusion of LAD. Successful primary angioplasty using thrombo-aspiration was done, in difficult clinical scenario. The case was challenging in terms of use of anticoagulation and antiplatelet strategy in a rare etiology of acute myocardial infarction following road traffic accident.
Keywords: Anterior wall myocardial infarction, Accidents, Traffic intracranial hemorrhage, Traumatic thoracic injuries
1. Introduction
Among the non-atherosclerotic etiologies of acute myocardial infarction (AMI) in young adults, blunt chest trauma is one of the extremely rare mechanisms.1,2 Earlier few case reports did not describe the true incidence of cases of traffic accidents leading to AMI and most of them were treated conservatively.3,4 This report describes a case of AMI following a blunt chest trauma due to road traffic accident resulting in severe left ventricular dysfunction and treated successfully with percutaneous coronary intervention (PCI).
2. Case report
A 36-year-old male rushed to emergency room with history of road traffic accident, complaining of headache, chest pain and inability to move right arm. On examination, patient was conscious and coherent with relatively stable vital parameters [pulse 98/min, blood pressure 100/70 mmHg, respiratory rate 36/min and temperature was 36.7 °F]. His general and neurological examination revealed blunt chest trauma, left parietal head injury, left orbital ecchymosis with red eye, grade 0 power in the right arm.
On cardio-respiratory examination, crackles were present in lung base without any murmur or rub. There was no distension, organomegaly or tenderness on abdominal examination. Cardiac monitor in ER showed ST elevation. ECG showed Q wave and 10 mm ST segment elevation in all precordial leads (Fig. 1). CT scan brain showed hemorrhagic contusions in left parietal area and fractures in the parietal bone and hemorrhage in left parietal area (Fig. 2). Bedside echocardiography revealed akinesia of apical and mid inter-ventricular septal, apical and apico-anterior segments with preserved thickness and calculated LVEF of 32% (modified Simpson's method).
Fig. 1.
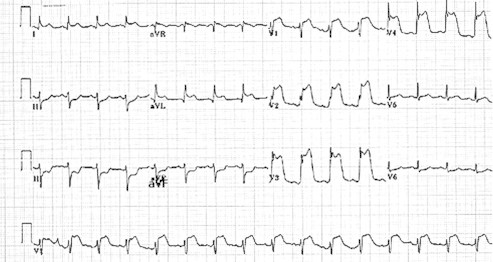
ECG showing anterior wall MI [ST elevation in leads V1-4] with reciprocal ST depression in inferior leads.
Fig. 2.
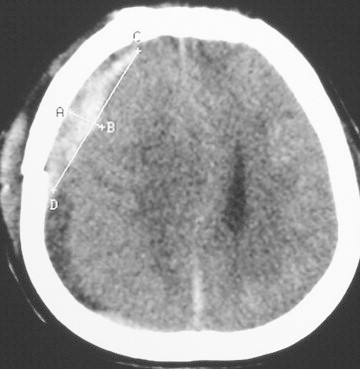
CT scan brain showed hemorrhagic contusions in left parietal area and fractures in the parietal bone and hemorrhage in left parietal area.
It was difficult to convince the patient's relatives about RTA's role in etiology of AMI & the need for invasive procedure'. After persuasion, a diagnostic coronary angiogram was performed which revealed thrombotic occlusion of ostial LAD with extension of thrombus in Ramus. Right coronary artery and left circumflex artery were normal (Fig. 3a, b, c). After discussing with Neuro-surgeon and Cardiac-surgeon about benefit of procedure versus risk of further increase in intracranial bleed, primary PCI was opted as a strategy of revascularization. The loading dose of clopidogrel 300 mg (as an only antiplatelet agent) was given and intravenous heparin 5000 IU (as an anticoagulant under monitoring of ACT) at the time of procedure. Loading dose of aspirin was not administered.
Fig. 3.
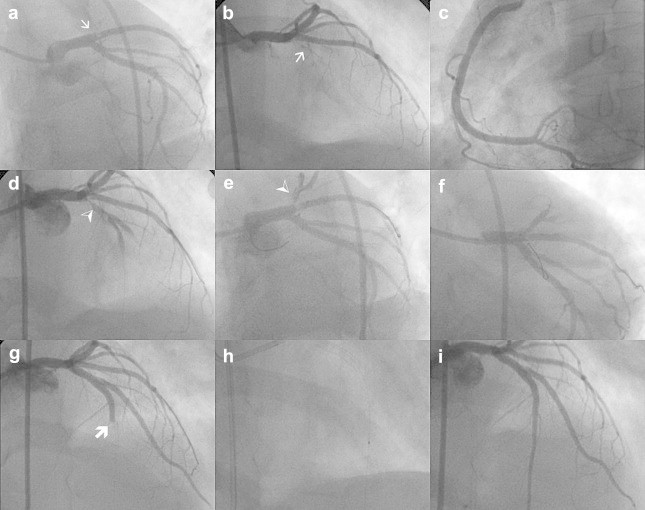
(a, b): Showing ostial thrombotic occlusion of LAD artery [thin arrow] in AP cranial and LAO caudal views. (c) Right coronary artery was normal except for mild plaque in the mid segment. (d, e) After thrombo-aspiration and balloon dilatation there was dissection with residual thrombus in ostio-proximal segment of LAD. (f) Bare metal stent [4 × 23 mm] was placed across ostio-proximal segment of LAD with protection of ramus with another guide wire. (g, h) Showing dislodgement of thrombus [thick arrow] in mid LAD segment which was thrombo-aspirated. (i) Showing final angiogram with complete recanalization with no residual stenosis with TIMI III flow.
After crossing occluded LAD and Ramus intermedius with floppy guide wires, initial thrombo-aspiration with Diver CE catheter (eV3, Inc., Plymouth, Minnesota, USA) could not retrieve much thrombus. The lesion was pre-dilated with 2.5 × 15 mm Voyager RX (Abbott Vascular) balloon. The check angiogram revealed mild dissection and some residual thrombus (Fig. 3d, e) with flow limitation (TIMI 2 flow). Hence, 4 × 23 mm bare metal stent was deployed at the ostio-proximal segment of LAD (Fig. 3f) without further dilatation attempts to seal dissection flap and improve flow in LAD. Check angiogram revealed dislodgment of thrombus to mid LAD segment, which was retrieved by Diver CE (eV3, Inc., Plymouth, Minnesota, USA) thrombo-aspiration catheter (Fig. 3g, h and Fig. 4). Finally TIMI III coronary flow was achieved with no residual stenosis (Fig. 3i). His neurological status was stable without any deterioration; patient improved significantly in terms of right arm power [Grade 3] and was discharged after 2 days. His echocardiography before discharge showed improvement in EF to 48%. Clopidogrel 75 mg OD was prescribed as a maintenance antiplatelet therapy without aspirin. Patient recovered well and completed one year of follow up without symptoms.
Fig. 4.

Showing aspirated large thrombus in fragments which was dislodged in mid LAD.
3. Discussion
Blunt chest trauma is a rare cause of cardiac damage including myocardial contusion, ventricular rupture, ventricular septal defect, valvular damage5 and coronary artery occlusion with myocardial infarction2 The most frequently injured vessel is the left anterior descending artery, followed by the right coronary and the circumflex coronary arteries.1 The mechanisms of injury contributing to infarction can include an intimal tear, subintimal hemorrhage, intra-luminal thrombosis, and spasm.6
The treatment of acute myocardial infarction caused by blunt chest trauma may be complicated by the severity of accompanying injuries, and most of the cases in the literature have been managed conservatively.3,7 Successful thrombolytic treatments of coronary occlusions in patients with blunt chest trauma have been reported.8,9 However, many trauma patients will not be candidates for thrombolytic therapy because of the risk of hemorrhage from coexisting injuries.10 In complicated cases, immediate surgical corrections were often performed.11 Recently, direct PCI has been performed in some patients and a few cases of stent implantation were reported.10,12
4. Conclusion
This case is a rare complication of blunt chest trauma leading to AMI. Clinically and technically there were challenges in the form of selection and doses of anti-thrombotics, for angioplasty ostial site of occlusion and coexisting intracranial bleeding. No remarkable long-term result has been reported about the prognosis of the coronary artery occlusion caused by the trauma. Considering the overall condition of this patient, angioplasty with stenting appeared to be the only option of thrapy.
Conflicts of interest
All authors have none to declare.
References
- 1.Ginzburg E., Dygert J., Parra-Davila E. Coronary artery stenting for occlusive dissection after blunt chest trauma. The Journal of Trauma. 1998;45:157. doi: 10.1097/00005373-199807000-00034. [DOI] [PubMed] [Google Scholar]
- 2.B.T, Moosikasuwan J.B., Thomas J.M. Myocardial infarction as a complication of injury. J Am Coll Surg. 2000;190:665–670. doi: 10.1016/s1072-7515(00)00263-5. [DOI] [PubMed] [Google Scholar]
- 3.Sinha A.K., Agrawal R., Singh A. Acute myocardial infarction due to blunt chest trauma. Indian Heart Journal. 2002;54:713–714. [PubMed] [Google Scholar]
- 4.Barton E., Henry R., Martin A. Acute myocardial infarction following blunt chest trauma due to the kick of a cow. West Indian Medical Journal. 1988;37:236–239. [PubMed] [Google Scholar]
- 5.Tengler M. The spectrum of myocardial contusion: a review. J Trauma. 1985;25:620–627. doi: 10.1097/00005373-198507000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Lee D.W., Garnic J.D., Barlow G.C. Acute anterior wall myocardial infarction secondary to blunt chest trauma–a case report. Angiology. 1990;41:82. doi: 10.1177/000331979004100113. [DOI] [PubMed] [Google Scholar]
- 7.Anto M.J., Cokinos S.G., Jonas E. Acute anterior wall myocardial infarction secondary to blunt chest trauma. Angiology. 1984;35:802. doi: 10.1177/000331978403501209. [DOI] [PubMed] [Google Scholar]
- 8.K.M. Ledley GS, Yazdanfar S, et al. Acute thrombotic coronary occlusion secondary to chest trauma treated with intracoronary thrombolysis. Am Heart J. 123:518–521. [DOI] [PubMed]
- 9.Orbe L.C., Gallego F.G., Sobrino N. Acute myocardial infarction after blunt chest trauma in young people: need for prompt intervention. Catheterization and Cardiovascular Diagnosis. 1991;24:182–185. doi: 10.1002/ccd.1810240309. [DOI] [PubMed] [Google Scholar]
- 10.Salmi A., Blank M., Slomski C. Left anterior descending artery occlusion after blunt chest trauma. The Journal of Trauma. 1996;40:832. doi: 10.1097/00005373-199605000-00028. [DOI] [PubMed] [Google Scholar]
- 11.Neiman J., Hui W. Posteromedial papillary muscles rupture as a result of right coronary artery occlusion after blunt chest injury. American Heart Journal. 1992;123:1694. doi: 10.1016/0002-8703(92)90827-i. [DOI] [PubMed] [Google Scholar]
- 12.James M.L., David B.C., Peter S.M. Acute myocardial infarction caused by blunt chest trauma: successful treatment by direct coronary angioplasty. Am Heart J. 1996;132:1275–1277. doi: 10.1016/s0002-8703(96)90475-5. [DOI] [PubMed] [Google Scholar]