

Abstract
OBJECTIVES:
To review the epidemiological aspects of fractures of the tibial plateau in a level one hospital.
METHODS:
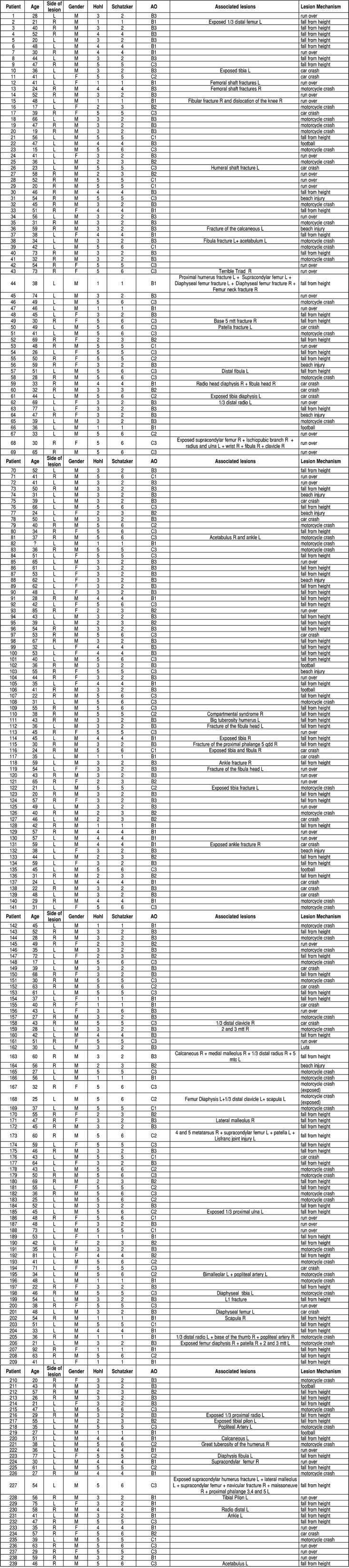
We retrospectively analyzed 239 tibial plateau fractures treated surgically. We took into account age, gender, trauma mechanism, classification of the injuries, associated injuries and affected side.
RESULTS:
168 were male, the fifth decade has been the most affected, the mechanism of trauma, car accident was the main causal fator, 128 cases were on the left side and 22,6% had associated injuries.
CONCLUSIONS:
Most patients were male, in the fifth decade of life, and victim of traffic accidents, and the depression and shear fractures of the tibial plateau are the most frequent. Associated lesions were infrequent in our study. Level of Evidence II, Prognostic Studies. Investigating the Effect of a Patient Characteristic on the Outcome of Disease.
Keywords: Tibial Fractures/epidemiology, Knee joint, Knee injuries
INTRODUCTION
The tibial plateau fractures represent 1-2% of all fractures and approximately 8% of the fractures in elderly. 1
Epidemiological studies are essential tools for understanding the occurrence of the injury. In this study, we observed age, side, gender, mechanism of injury, most frequently type of injury and injuries associated with tibial plateau fractures.
The objective of this research was to provide a retrospective epidemiological study of tibial plateau fractures in a level I trauma hospital.
METHODS
Two hundred and thirty nine tibial plateau fractures treated surgically in a trauma hospital level I, between January 2006 and January 2011, were analyzed retrospectively. The survey was conducted through an active search in Hospital Municipal Miguel Couto (HMMC) database using the International Classification of Diseases (ICD) S82-1, which corresponds to fractures of the proximal tibia. We then performed, from the record number of the patient in HMMC, consulting of the records and archives of images of the same patients. Inclusion criteria were patients of both sexes and all ages, who underwent surgical treatment of tibial plateau fractures, regardless of having or not related injuries, as well as comorbidities. Patients treated by non-surgical method and those whose records and/or imaging were insufficient were excluded from the study. Age, gender, side of the lesion, injury mechanism and classification of lesions were taken into consideration. All charts and radiographs in antero-posterior and lateral knee were evaluated by a physician with a PhD degree member of Sociedade Brasileira de Cirurgia do Joelho (Brazilian Society of Knee Surgery).
Of the 244 patients analyzed, five were excluded from the analysis, two due to non-surgical treatment, three for presenting records and/or imaging with incomplete information regarding the questions considered in this study. Such exclusion was due to failure in obtaining information regarding the trauma mechanism of injury. Were effectively included 239 patients in our analysis. This research is in accordance with the Declaration of Helsinki of the World Medical Association. The descriptive analysis presented in tables the observed data, expressed as mean ± standard deviation (SD) for numeric data, and frequency (n) and percentage (%) for categorical data. Graphs were plotted to illustrate the relative distribution of severity scales. Statistical analysis was conducted using the statistical software SAS(r) System version 6.11 (SAS Institute, Inc., Cary, North Carolina).
RESULTS
Table 1 provides the frequency (n) and percentage (%) of the characteristics of the 239 patients in study.
Table 1. Sample Characteristics.
| Variable | Category | n | % |
|---|---|---|---|
| Age (years)* | 44,5±14,4 | (15 - 92) | |
| Sex | male | 168 | 70,3 |
| female | 71 | 29,7 | |
| Side of the lesion | right | 111 | 46,4 |
| left | 128 | 53,6 | |
| Mechanism of the lesion | fall from height | 96 | 40,2 |
| motorcycle crash | 54 | 22,6 | |
| run over | 45 | 18,8 | |
| car crash | 26 | 10,9 | |
| beach injury | 10 | 4,2 | |
| football | 7 | 2,9 | |
| fight | 1 | 0,4 | |
| Associated lesions | present | 54 | 22,6 |
| absent | 185 | 77,4 |
(*) Age is expressed by mean ± St. deviation (minimum - maximum). Source: SOT-HMMC, 2011
Figure 1 illustrates the relative distribution in descending order of the mechanisms of injury to the sample.
Figure 1. Relative distribution in ascending order of lesion mechanisms in the whole sample.

Figure 2 shows the frequency distribution by age of patients with tibial plateau fractures. It was observed that 71% of injuries occurred in those aged 30-60 years.
Figure 2. Frequency distribution by age range.

Table 2 provides the frequency (n) and percentage (%) of classifications of tibial plateau by Hohl, Schatzker and AO. It can be observed in Table 2 that 52% of the lesions were of low energy (level < 3) according to Schatzker and Hohl scales, approximately 36% of the lesions were in the high energy in the scales of Hohl (level 5), Schatzker (levels 5 and 6 ) and AO (levels C1, C2 and C3). (Table 2) The Chart 1 shows the overall sample of injuries.
Table 2. Classification of the tibial plateau to the 239 lesions.
| Scale | level | n | % |
|---|---|---|---|
| Hohl | 1 | 20 | 8,4 |
| 2 | 20 | 8,4 | |
| 3 | 86 | 36 | |
| 4 | 28 | 11,6 | |
| 5 | 85 | 35,6 | |
| Schatzker | 1 | 20 | 8,4 |
| 2 | 84 | 35,1 | |
| 3 | 21 | 8,8 | |
| 4 | 28 | 11,7 | |
| 5 | 38 | 15,9 | |
| 6 | 48 | 20,1 | |
| AO | B1 | 44 | 18,4 |
| B2 | 23 | 9,6 | |
| B3 | 88 | 36,9 | |
| C1 | 13 | 5,4 | |
| C2 | 20 | 8,4 | |
| C3 | 51 | 21,3 |
Source: SOT-HMMC, 2011.
DISCUSSION
There is, to date, no research on epidemiological study of tibial plateau fractures in the national literature. For this reason, our study is important and relevant, especially if we take into consideration the huge socioeconomic impact involved in the genesis of this and many other traumatic injuries produced mostly by traffic violence. At the beginning of the last decade, between 20 and 50 million people around the world were fully or partially disabled due to injuries caused by traffic accidents and about 10% occupied hospital beds during this period. 2
Although there are no consistent data from the Ministry of Health specifically on the tibial plateau fractures, but taking it as a marker of musculoskeletal trauma, and considering that 52.3% of patients in our sample were victims of traffic trauma and 22.6% had associated injuries, it becomes evident the need of adopting a series of proactive actions to reduce accidents on public roads. Recent government campaigns such as the "Alcohol Prohibition Law", in which the risks of alcohol intake and disrespect traffic rules are strongly cautioned and offenders punished, as well as the "Projeto Vida no Transito" (Project "Life in Traffic", or National Pact for Accident Reduction), signed in September 2012 by the Minister of Health, aim to reduce the number of accidents and deaths on Brazilian roads and streets. 3 Moreover, mostly from medium to long term, we believe that standardization of control and education measures can change the existing epidemiological paradigm in our country.
Besides traffic accidents, 7.5% of our patients underwent tibial plateau fractures through sports trauma. Characteristically, we believe that the reason is due to the physical location of our hospital, situated in the coastal region of the city, a place that encourages sports activities. Quite punctual and curious, we observed that some injuries due to injury at sea (in the beach) occurred in older populations, probably due to a lower bone quality.
In our study, the most affected gender was the male sex, which was not seen in the study of Schulak Gunn 4 , who found no difference between genders. In our opinion, the predominance of males in the population due to their greatest vulnerability and exposure to risk situations, such as the use of physical strength during most physical activities and physical labor or dangerous high speed driving and disregard to traffic laws. 5 Another important observation of the current study was that most fractures occurred in individuals in the fifth decade of life, usually associated with traffic injuries and falls from height. Schatzker et al. 6 , in his classic 1979 study, reported the sixth and seventh decades of life as the most frequent ages of tibial plateau injuries. Again, we believe that the increased traffic trauma greatly influenced the decrease in most frequent age of injuries observed by Schatzker et al. 6 Due to this fact, the fracture patterns most frequently observed in our study were moderate and high energy, namely, the bicondylar injuries and the combination of shear and depression of the lateral tibial plateau, respectively seen in 36% and 35.1% of the patients. We classified the fractures according to three distinct systems which are usually used in the literature, Hohl's, Schatzker's et al. 6 and the AO Group's. 7 - 9 It is known that there is no consensus on which classification should be adopted in tibial plateau fractures, although the two most used are Schatzker's et al. 6 and the AO Group's. 7 - 9 In a national survey, Albuquerque et al. 10 included Hohl's classification to the previous two, noting that the later present greater interobserver accordance. More recently, Luo et al. 11 proposed the use of the "three collumn" concept in the classification of tibial plateau fractures, giving a new perspective on a subject still undefined in the literature.
Finally, regarding to imaging tests, we routinely used radiographs in anteroposterior and lateral knee. We know that ideally a series of knee trauma was to be performed , in which the oblique radiographs at 45º are included, and not rarely, computed tomography (CT), which we began to use on a regular basis from 2009. 12 Because this retrospective study started in 2006, our sample included some patients who did not undergo the oblique views or CT of the knee. For this reason, we adopted as standard only knee anteroposterior and lateral radiographic incidences, which is corroborated by the study of Dirschl and Dawson. 13
One of the weaknesses of our study was the inability to search the associated intra-articular lesions of the knee. We know that the lateral tibial plateau fractures are associated with significant risk of meniscal and capsuloligamentous injuries. In these patients, when the joint depression is greater than 6mm and the extension of the plateau greater than 5mm, the lesion of the lateral meniscus may be present in 83% of fractures, compared with 50% in fractures with less deviation. The medial meniscus injury happens more often when depression and enlargement overcome 8mm. 8 Magnetic ressonance imaging (MRI), in our view, should be sought in all patients with tibial plateau fractures, a procedure corroborated by several authors, although its high cost, and not being available in many public Brazilian hospitals. 8 , 14 - 17 .
One of the authors' suggestions, based on this last observation is that the MRI might soon become popular in hospitals of the Unified Health System (SUS), considering that a great number of patients shall benefit, either for intra-articular lesions analysis of the knee in tibial plateau fractures as well as in many other traumatic and non-traumatic musculoskeletal system diseases, such as spinal cord injuries and herniated discs, respectively.
CONCLUSION
In the population studied, the authors noted that most patients who suffer complete tibial plateau are male, around the fifth decade of life, mostly victims of traffic accidents with depression type bicondylar fractures or shear joint. Perhaps due to the lack of MRI images, associated injuries were uncommon in our study.
The adoption of preventive measures such as educational campaigns, surveillance and traffic education, and the inclusion of sensitive imaging methods in major trauma centers in our country, such as CT and MRI, can respectively reduce the number of injuries and improve victim patient care of tibial plateau fractures.
Footnotes
Work performed at Orthopedic Surgery and Traumatology Professor Nova Monteiro, Hospital Municipal Miguel Couto (OST-HMMC), Rio de Janeiro, RJ, Brazil.
Citation: Albuquerque RP, Hara R, Prado J, Schiavo L, Giordano V, Amaral NP. Epidemiological study on tibial plateau fractures at a level I trauma center. Acta Ortop Bras. [online]. 2013;21(2):109-15. Available from URL: http://www.scielo.br/aob.
REFERENCES
- 1.Jacofsky DJ, Haidukerwych GJ. Scott WN. Insall & Scott Surgery of the knee. Philadelphia: Churchill Livingstone; 2006. Tibia plateau fractures; pp. 1133–1146. [Google Scholar]
- 2.Souza ER, Minayo MCS, Franco LG. Avaliação do processo de implantação e implementação do Programa de Redução da Morbimortalidade por Acidentes de Trânsito. Epidemiologia e Serviços de Saúde. 2007;16(1):19–31. [Google Scholar]
- 3. [Acessado em abril de 2013];Padilha assina Pacto pela Redução de Acidentes. a Available from: http://portalsaude.saude.gov.br/portalsaude/noticia/7315/162/padilha-assina-pacto-pela-reducao-de-acidentes.html.
- 4.Schulak DJ, Gunn DR. Fractures of tibial plateau. A review of the literature. Clin Orthop Relat Res. 1975;(109):166–177. doi: 10.1097/00003086-197506000-00025. [DOI] [PubMed] [Google Scholar]
- 5.Marín-León L. [Acessado em abril de 2013];Acidentes de trânsito, um problema de saúde pública. a Available from: http://www.unicamp.br/unicamp/unicamp_hoje/jornalPDF/234pag04.pdf.
- 6.Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968-1975. Clin Orthop Relat Res. 1979;(138):94–104. [PubMed] [Google Scholar]
- 7.Charalambous CP, Tryfonidis M, Alvi F, Moran M, Fang C, Samarji R, et al. Inter- and intra-observer variation of the Schatzker and AO/OTA classifications of tibial plateau fractures and a proposal of a new classification system. Ann R Coll Surg Engl. 2007;89(4):400–404. doi: 10.1308/003588407X187667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Luciano RC, Krause M, Skaf AY. Projeto Diretrizes: Fratura do planalto tibial. Associação Médica Brasileira / Conselho Federal de Medicina; 2007. pp. 1–9. [Google Scholar]
- 9.Walton NP, Harish S, Roberts C, Blundell C. AO , Schatzker? How reliable is classification of tibial plateau fractures? Arch Orthop Trauma Surg. 2003;123(8):396–398. doi: 10.1007/s00402-003-0573-1. [DOI] [PubMed] [Google Scholar]
- 10.Albuquerque RP, Giordano V, Pallottino A, Sassine T, Canedo R, Pina J, et al. Analise da reprodutibilidade das classificações das fraturas do platô tibial. Rev Bras Ortop. 2009;44(3):225–229. doi: 10.1016/S2255-4971(15)30072-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Luo C-F, Sun H, Zhang B, Zeng B-F. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma. 2010;24(11):683–692. doi: 10.1097/BOT.0b013e3181d436f3. [DOI] [PubMed] [Google Scholar]
- 12.Kfuri M, Júnior , Fogagnolo F, Bitar RC, Freitas RL, Salim R, Paccola CAS. Fraturas do planalto tibial. Rev Bras Ortop. 2009;44(6):468–474. doi: 10.1016/S2255-4971(15)30142-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dirschl DR, Dawson PA. Injury severity assessment in tibial plateau fractures. Clin Orthop Relat Res. 2004;(423):85–92. doi: 10.1097/01.blo.0000132626.13539.4b. [DOI] [PubMed] [Google Scholar]
- 14.Gardner MJ, Yacoubian S, Geller D, Suk M, Mintz D, Potter H, et al. The incidence of soft tissue injury in operative tibial plateau fractures: a magnetic resonance imaging analysis of 103 patients. J Orthop Trauma. 2005;19(2):79–84. doi: 10.1097/00005131-200502000-00002. [DOI] [PubMed] [Google Scholar]
- 15.Shepherd L, Abdollahi K, Lee J, Vangsness CT Jr. The prevalence of soft tis-sue injuries in nonoperative tibial plateau fractures as determined by magnetic resonance imaging. J Orthop Trauma. 2002;16(9):628–631. doi: 10.1097/00005131-200210000-00003. [DOI] [PubMed] [Google Scholar]
- 16.Stannard JP, Lopez R, Volgas D. Soft tissue injury of the knee after tibial plateau fractures. J Knee Surg. 2010;23(4):187–192. doi: 10.1055/s-0030-1268694. [DOI] [PubMed] [Google Scholar]
- 17.Yacoubian SV, Nevins RT, Sallis JG, Potter HG, Lorich DG. Impact of MRI on treatment plan and fracture classification of tibial plateau fractures. J Orthop Trauma. 2002;16(9):632–637. doi: 10.1097/00005131-200210000-00004. [DOI] [PubMed] [Google Scholar]