

Abstract
Mucocele of the appendix is a term used to describe a dilated, mucin-filled appendix. It is most commonly the result of epithelial proliferation, but can be caused by inflammation or obstruction of the appendix. Two cases of mucocele of the appendix are presented with a discussion of the histologic and radiologic features as well as the surgical management.
CASE REPORTS
Case 1. A 30-year-old man presented to the emergency department at Baylor University Medical Center at Dallas with a 1-day history of cramping abdominal pain with nausea, vomiting, and diarrhea. He reported mild tenderness to palpation in the left lower quadrant. The patient was afebrile with stable vital signs and a normal white blood cell count. A contrast-enhanced computed tomography (CT) study of the abdomen and pelvis revealed the stomach, small bowel, and colon to be fluid filled. These findings were compatible with the clinical impression of gastroenteritis. The appendix was dilated to 1.6 cm and filled with low-density material. Calcific deposits were present in the wall of the appendix, but there were no surrounding inflammatory changes (Figure 1a). The CT findings were compatible with a mucocele of the appendix, and a laparoscopic appendectomy was performed. Final pathology revealed a mucinous cystadenoma of the appendix.
Figure 1.
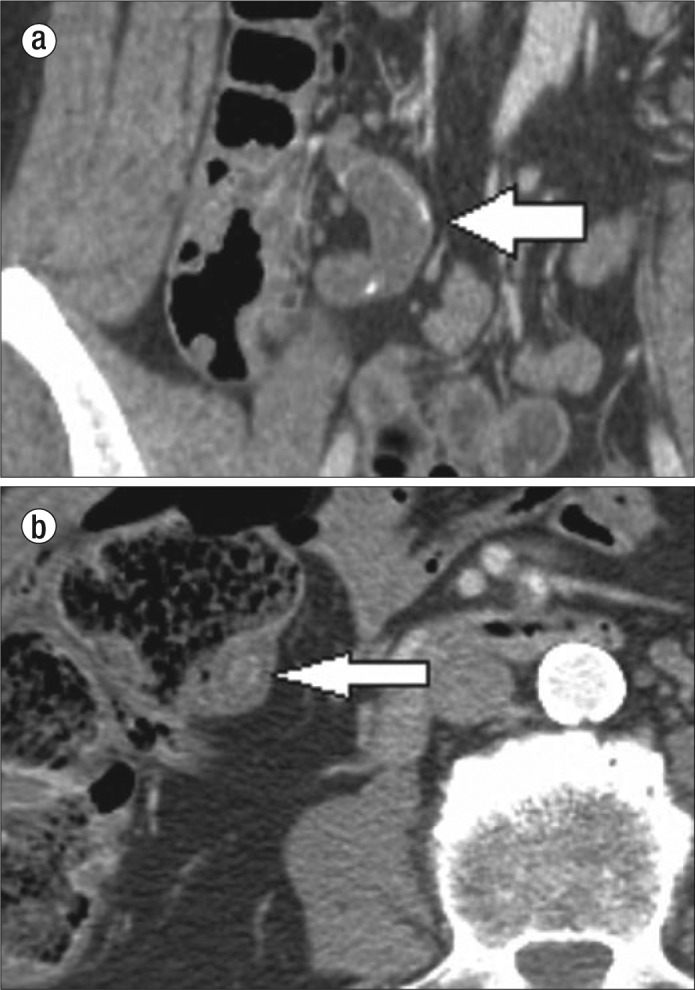
Mucocele of the appendix. (a) Coronal CT image of the right lower quadrant in patient 1 shows a dilated appendix with thin calcification in the wall (white arrow). (b) Axial CT image of the right lower quadrant in patient 2 shows a dilated appendix with an appendicolith.
Case 2. A 72-year-old man presented to the emergency department at Baylor University Medical Center at Dallas with vomiting and acute worsening of longstanding abdominal pain with localization to the right lower quadrant. He was in mild discomfort and had tenderness to palpation in the right lower quadrant, greatest at McBurney's point. The patient had no peritoneal signs. A contrast-enhanced CT study of the abdomen and pelvis showed the appendix to be dilated to 2.7 cm and filled with low-density material. An appendicolith was also present at the base of the appendix (Figure 1b). The CT findings were compatible with a mucocele of the appendix, and a laparoscopic appendectomy was performed. Histologic study of the excised appendix revealed both chronic and acute inflammatory changes with mucin accumulation and evidence of previously ruptured appendiceal diverticulum.
DISCUSSION
Mucocele of the appendix is a descriptive term that refers to dilation of the appendiceal lumen as a result of mucin accumulation and is based on the gross or macroscopic appearance of the appendix. Mucocele formation is most commonly caused by epithelial proliferation, either benign or malignant. Much less frequently, inflammatory or obstructive causes, to include appendicitis and obstruction by a fecalith or appendicolith, are the cause of mucocele formation.
Mucinous neoplasms of the appendix are classified on a spectrum from benign to malignant based upon certain features during histologic examination. On the benign end of the spectrum, there is the mucinous cystadenoma with no risk of recurrence. On the malignant end of the spectrum is the mucinous adenocarcinoma with a very poor survival rate and a high rate of metastases to lymph nodes and liver. In between these disparate entities lie the mucinous neoplasms with low and high rates of recurrence. There is controversy in using the descriptors low and high rates of recurrence with mucinous neoplasms, as the World Health Organization classifies both in the term “low-grade mucinous neoplasm.” Many prefer to use the descriptors because the risk of recurrence and associated morbidity and mortality differ greatly between the two (1). These intermediate-grade tumors are characterized by mucin dissecting into or through the wall of the appendix with or without epithelial cells. Extraappendiceal mucin with epithelial cells characterizes the mucinous neoplasm with a high rate of recurrence. This is the neoplasm of the appendix that is most commonly the cause of pseudomyxoma peritonei, a complication characterized by noninvasive mucinous deposits throughout the peritoneum (Figure 2).
Figure 2.

Coronal CT image of the abdomen and pelvis shows multiple low-density collections throughout the abdomen and pelvis causing mass effect on adjacent organs, compatible with pseudomyxoma peritonei (white stars).
Mucoceles are frequently discovered incidentally, as most are the result of a mucinous cystadenoma that causes no inflammation (2). When imaged with CT, a mucocele of the appendix will typically manifest as homogenous hypoattenuating material that has Hounsfield values similar to water filling the lumen of the appendix. The presence of curvilinear calcification in the wall of the appendix is highly suggestive of a mucocele (3). The spatial resolution of CT usually allows for a confident diagnosis of a dilated appendix. When extending into the pelvis of a woman, the appendix must be differentiated from the right ovary and fallopian tube, as a cystic ovarian neoplasm, tubo-ovarian abscess, and hydrosalpinx could have a similar appearance. Additional differential diagnoses include enteric duplication cyst, mesenteric cyst, and Meckel diverticulum.
Mucoceles are treated surgically, and the preoperative diagnosis aids in the planning of a careful mobilization and resection to prevent peritoneal contamination. A right hemicolectomy is frequently performed if a malignant cause is suspected based on imaging or on intraoperative frozen section (4). Right hemicolectomy was not performed in these cases because frozen section analysis at the time of surgery showed no malignant characteristics. Since the risk of developing an adenocarcinoma of the colon is six times greater in patients with a mucocele than in the general population, colonic surveillance is warranted in these cases (5).
References
- 1.Pai RK, Longacre TA. Appendiceal mucinous tumors and pseudomyxoma peritonei: histologic features, diagnostic problems, and proposed classification. Adv Anat Pathol. 2005;12(6):291–311. doi: 10.1097/01.pap.0000194625.05137.51. [DOI] [PubMed] [Google Scholar]
- 2.Persaud T, Swan N, Torreggiani WC. Giant mucinous cystadenoma of the appendix. Radiographics. 2007;27(2):553–557. doi: 10.1148/rg.272065134. [DOI] [PubMed] [Google Scholar]
- 3.Pickhardt PJ, Levy AD, Rohrmann CA, Jr, Kende AI. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. Radiographics. 2003;23(3):645–662. doi: 10.1148/rg.233025134. [DOI] [PubMed] [Google Scholar]
- 4.Dhage-Ivatury S, Sugarbaker PH. Update on the surgical approach to mucocele of the appendix. J Am Coll Surg. 2006;202(4):680–684. doi: 10.1016/j.jamcollsurg.2005.12.003. [DOI] [PubMed] [Google Scholar]
- 5.Federle MP, Anne VS. Mucocele of the appendix. In: Federle MP, editor. Diagnostic Imaging: Abdomen. Salt Lake City, UT: Amirsys; 2004. pp. 26–27. [Google Scholar]