

Abstract
Background
In view of the contemporary relevance of BMW Management, a system analysis of BMW management was conducted to ascertain the views of Service hospitals/HCE's on the current system in BMW management in-vogue; to know the composition and quantity of waste generated; to get information on equipment held & equipment required and to explore the possibility of outsourcing, its relevance and feasibility.
Methods
A qualitative study in which various stake holders in BMW management were studied using both primary (Observation, In-depth Interview of Key Personnel, Group Discussions: and user perspective survey) and secondary data.
Results
All the stake holders were of the opinion that where ever possible outsourcing should be explored as a viable method of BMW disposal. Waste generated in Colour code Yellow (Cat 1,2,3,5,6) ranged from 64.25 to 27.345 g/day/bed; in Colour code Red (Cat 7) from 19.37 to 10.97 g/day/bed and in Colour code Blue (Cat 4) from 3.295 to 3.82 g/day/bed in type 1 hospitals to type 5 hospitals respectively.
Conclusion
Outsourcing should be explored as a viable method of BMW disposal, were there are government approved local agencies. Facilities authorized by the Prescribed Authority should be continued and maintained where outsourcing is not feasible.
Keywords: Biomedical waste, Systems analysis, Qualitative study
Introduction
The Bio-Medical Waste (BMW) (Management and Handling) Rules 1998, prescribed by the Ministry of Environment and Forest, Government of India, came into force on 20 July 1998.1 The Armed Forces Medical Services (AFMS) took the lead in developing biomedical waste management systems across the wide spectrum of its Health Care Establishments (HCEs) across the country.
The existing policy on the subject is now due for review.2 In view of this; a qualitative study using the systems approach was conceptualized and undertaken concerning the existing BMW management system in the Armed Forces.
Why the systems approach to BMW?
A system is a group of elements (persons, organizations, equipment, concepts, etc.) that are related in such a way that they influence each other and the behaviour of the elements as a whole. System analysis is examination of various elements of a system with a view to ascertain whether the proposed solution to a problem will fit the system and in turn effect an overall improvement in the system.3
The systems doctrine is associated with the concept of integrative approach, which follows the principal of irreducibility of the whole to its parts, as the whole is understood to have properties more than the sum of its parts. The goal of system analysis is to define the significant feature of the problem under study and it is used for planning, improved methods of delivery, effectiveness analysis and decision analysis.4
There is no dearth of studies regarding BMW management in literature. These cover varied facets of BMW like awareness regarding BMW among health care workers,5,6 quantum of waste generated in HCEs,7 Infrastructure of Hospitals to handle BMW,8 Environmental and health risks associated with BMW management etc.9,10 While these studies are of great help in initiating corrective measures at the local level but they suffer from an inherent limitation of most quantitative studies viz. they view only one particular aspect at one point of time. There are multiple stake holders at all levels in the management of BMW in the AFMS and civil health care system. Since the holistic picture is not viewed by quantitative research methods, there cannot be intervention at the level of policy. In such a complex situation, qualitative research tools are often used to analyse the system at a macro level to suggest policy interventions. The BMW management system in the Armed Forces can be conceptualized as an open ended System (Fig. 1) where, on one hand the subsystems are in continuous interaction among each other and on the other hand these subsystems separately and the system as a whole, are constantly influenced by the external environment. The study design was accordingly formulated based on the above Systems Approach to review the current BMW disposal in the AFMS and recommend policy changes to improve it further.
Fig. 1.

BMW management system in armed forces.
Materials and methods
The study design was a cross sectional qualitative study in which various stake holders and facets of BMW management system (Fig. 1) in Armed Forces were taken into consideration. Samples drawn were purposive, with the objective of including maximum tertiary care hospitals as they generate maximum BMW. The following tools were used for data collection:
-
1)Observation:
-
(a)Visit to BMW management facilities in service HCEs in two cities.
-
(b)Visit to a corporate hospital each in three cities to observe their BMW management practices.
-
(c)Visit to two large tertiary care Government Hospitals in two cities.
-
(d)Visit to a Common Biomedical Waste Treatment Facility (CBWTF) managed by a private vendor, approved by local civic authority and the State Pollution Control Board.
-
(a)
-
2)In-depth Interview of Key Personnel:
-
(a)Commandant/Secretary BMW Management Committee of four service hospitals in different stations
-
(b)Senior executives dealing with policy making of BMW Management in the Ministry of Environment & Forests (MOEF) and Central Pollution Control Board (CPCB) at New Delhi.
-
(c)Administrative Head of a Corporate Hospital and a private laboratory
-
(d)Head of the BMW management in a large Medical College Hospital.
-
(a)
-
3)
Focus Group Discussions: Focus group discussions with Major General (MG) Medical of one of the Commands, Col Health (Nodal officers for implementation of BMW management programme in his area of responsibility) and faculty members concerned with BMW management of a service medical college.
-
4)
Survey Method: User perspective concerning BMW disposal was obtained through a self administered structured questionnaire sent to a purposive sample of HCEs in Armed Forces. Since the maximum BMW is expected to be generated from tertiary care hospitals, all Command Hospitals (CH) were included in this Survey. Response was received from 51 HCEs (Army-39, Navy-08 & Air Force-04). Stratification of 51 HCE's was done as per Table 1:
Table 1.
Stratification of Health Care Establishments according to bed strength.
| Strata | Hospitals | Number |
|---|---|---|
| Type 1 Hospitals | CHs, Army Hospital (R&R) and Base Hospital, Delhi Cantt. | 8 |
| Type 2 Hospitals | ≥500 bedded | 5 |
| Type 3 Hospitals | 300–499 bedded | 7 |
| Type 4 Hospitals | 50–299 bedded | 17 |
| Type 5 Hospitals | <50 bedded | 14 |
Quantity generated in different waste categories was clubbed in three categories viz. Yellow comprising of Cat 1,2,3,5,6; Red having Cat 7 and Blue Cat 4. Due to wide variation in quantity of waste generated in all the five categories of HCEs, median waste generated was used for analysis. The wide variation was attributed to the variance in the workload, which was directly related to the dependent clientele strength. Two hospitals with similar bed strength and staff could have a marked difference in their strength of dependent population. Hence the variation was not attributed to error in data compilation by the hospital.
Results
Since this study is using a systems approach to analyse all aspects of BMW management in Armed Forces, results are being presented collating all inputs, with a view to identify gaps in the existing system and suggest measures for improvement.
Visit to service hospitals
The various service hospitals visited were having their own facility for collection and final disposal of BMW. In one city having multiple service HCEs, the concept of a service CBWTF was in place and the other service hospitals were sending their BMW for final disposal to this CBWTF. The collection and disposal was satisfactory. However, some key interview informants admitted that there was no backup in case of any failure of the final disposal mechanism due to mechanical defect or environmental disruptions like storm, flash floods and exigencies of service and security reasons, especially in disturbed areas. During such times, there will be problem in disposal of BMW. They were of the unanimous opinion that in case vendors are available for outsourcing the final disposal, all such service hospitals should outsource the same to an approved vendor from their kerb site. Due to security reasons the collection, segregation and transportation to kerb site should be the responsibility of the service hospital. They stated that funds need to be earmarked from Annual Contingency Grant (ACG) for the same by the service hospitals.
Key informant interview with MOE&F and CPCB officials
MOE&F and CPCB officials were unanimously of the opinion during the key informant interview that as the pollution norms for incinerators are becoming more and more stringent, it would be economically and legally unviable for every hospital to have its own incinerator. Moreover, with some service hospitals being located in the vicinity of civil areas, the local civil authorities would not permit incinerators to operate and service hospitals may also have problem with environmental activists. They stated that the Courts are also not going to allow incinerators in populous areas. Therefore, the CPCB encourages vendors to establish a CBWTF in a city and the rates are negotiated with the local civic authority and the State PCB.2 They suggested that the AFMS should also join in, sending their BMW to the outsourced CBWTF for final disposal, rather than setting up in-house facility. However the MOEF and CPCB were aware of the peculiar problem of the Armed Forces concerning isolation of certain hospitals in far flung and disturbed areas, which would require stand-alone and dedicated final disposal modalities.
Visit to civil hospitals
All civil hospitals visited were outsourcing BMW management to the vendor approved by the local civic body and the state PCBs, from there kerb site. One Government medical college had gone a step further and outsourced the facility from the point of generation in wards, ICU, OT, dispensaries itself. All civil hospitals were of the opinion that outsourcing reduced their workload and ensured that they complied with the existing legislations, thus reducing their legal liabilities. However, one key informant clearly spelt out that the current BMW Rules require the Hospital Authorities to ensure that the final disposal is satisfactory, as there is no legal liability on the vendor. In other words, even if the vendor fails to discharge his duty properly, the HCE will be held responsible.
Visit to outsourcing vendor
The outsourcing vendor visited had State-of-the-Art facilities for outsourcing at rates approved by the local civic body and State PCB. It charged Rs 4.00 per bed per day, for collection of BMW from kerb point to final disposal site.11
User survey: quantity of BMW generated
Maximum waste generated was from the Wards followed by Operation Theater and Laboratory Services in Type 1 to Type 4 HCE's i.e. hospitals which are more than 50 bedded. In HCEs with less than 50 beds (Type 5), MI Rooms generated maximum bio-medical waste followed by Wards.
There was wide variation in the amount of BMW generated per bed across various HCEs even within the same level of HCEs (Table 2). Therefore, the median values were taken to calculate BMW in each category of hospitals. None of the Users had any complaints as regards collection, segregation and transportation of BMW to kerb site was concerned.
Table 2.
Summary of interquartile range (IR) and median values of waste generated among different categories.
| Yellow (Cat 1,2,3,5,6) | Red (Cat 7) | Blue (Cat 4) | |
|---|---|---|---|
| Type 1 Hospitals | |||
| IR | 5.78–187.37 | 2.00–69.32 | 1.11–75 |
| Median | 64.25 | 19.37 | 3.295 |
| Type 2 Hospitals | |||
| IR | 26.03–38.41 | 2.00–69.32 | 0.94–4.61 |
| Median | 34.325 | 3.91 | 2.16 |
| Type 3 Hospitals | |||
| IR | 15.46–138.51 | 4.50–43.88 | 1.02–12.31 |
| Median | 23.865 | 8.015 | 7.39 |
| Type 4 Hospitals | |||
| IR | 0.96–59.32 | 0.064–30.33 | 0.22–11.74 |
| Median | 28.06 | 8.86 | 2.00 |
| Type 5 Hospitals | |||
| IR | 1.25–267.67 | 5.55–15.55 | 0.68–33.26 |
| Median | 27.345 | 10.97 | 3.82 |
User survey: BMW final disposal equipment held by HCEs
There appears to be overkill as far as incinerators are concerned in service HCEs (Table 3). This is because all service units are also authorized Beehive incinerators for disposal of normal solid waste as per existing scales of accommodation. Most hospitals are using the same for BMW disposal also. Autoclaves, microwaves and shredders, though adequately scaled, are deficient in a large number of HCEs. This deficiency could be attributed to the fact that either the equipment has become vintage/obsolete or is unserviceable. Manual destruction of plastics is being done in hospitals deficient of shredders. It was seen that non-bedded HCEs like Field Hospitals and peripheral MI Rooms are not aware that they are authorized microwaves and hence have not procured the same. They are transporting BMW to nearest military hospital for disposal.
Table 3.
Summary of BMW handling equipment held by hospitals.
| Incinerator | Shredder | Microwave | Autoclave | |
|---|---|---|---|---|
| Type 1 Hospitals | ||||
| Authorized | 08 | 16 | 08 | 08 |
| Held | 09 | 11 | 15 | 01 |
| Type 2 Hospitals | ||||
| Authorized | 05 | 10 | 05 | 05 |
| Held | 05 | 05 | 05 | Nil |
| Type 3 Hospitals | ||||
| Authorized | 07 | 14 | 07 | Nil |
| Held | 06 | 07 | 07 | Nil |
| Type 4 Hospitals | ||||
| Authorized | 05 | 17 | 17 | Nil |
| Held | 14 | 03 | 2 | 01 |
| Type 5 Hospitals | ||||
Outsourcing
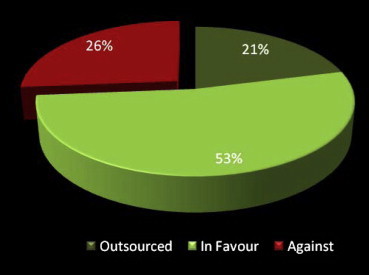
Out of 19 respondents who gave their comments regarding outsourcing of BMW to an approved vendor from the kerb site for final disposal, 14 were in favour of outsourcing and five were against it. All HCEs which were opposed to outsourcing were located in field area where no outsourcing agency was present (Fig. 2). Four of the fourteen respondents who were in favour of outsourcing have successfully outsourced their BMW handling to government approved local agencies. These were hospitals of the Air Force and Navy only. The Army has no experience regarding outsourcing of BMW. Since the bed occupancy of service hospitals is less than the authorized beds, one Type I hospital has negotiated with the vendor to charge them as per average bed occupancy in the last three years.
Fig. 2.
Outsourcing in armed forces.
Range of price quoted (Rs/day/bed) by various HCEs for outsourcing was between Rs 1.89 and Rs 8.60 with average of approx. Rs 5.00 per day per bed. The cost varied as per the location of the HCE.
Discussion
The Systems approach adopted in this Study aims to identify organizational, technical and social factors involved in the BMW disposal system. The ultimate goal of this approach is to suggest methods of improvement keeping in mind the current environment in which the system works.
There was wide variation in the amount of BMW generated per bed across various HCEs even within the same level of HCEs. Therefore, the median values were taken to calculate BMW in each category of hospitals. The Users had no complaints as regards collection, segregation and transportation of BMW to kerb site was concerned. The results of our study are similar to that of studies conducted at PGI, Chandigarh and by Passco Environmental Solutions Pvt. Ltd, outsourcing company recognized by Maharashtra Pollution Control Board, on a 1000 bedded hospital in Pune. These have come up with results of 60–250 g per day per bed12 and 75 g per day per bed11 respectively, which are almost similar to results we found in our Type 1 HCEs. The wide variation in BMW generated could be due to the confusion in colour coding as various categories have multiple options as per BMW Rules.13 The CPCB has attempted to address this problem by now giving new colour coding options which are mutually exclusive to various categories of BMW.14
Deficiency of BMW Equipment authorized by Director General Armed Forces Medical Services (DGAFMS) needs to be made up in concerned service hospitals. Shredder shows almost 50% deficiency in Type 1, 2 & 3 HCEs and more than 80% in Type 4 HCEs. Provision of shredder will reduce man-hours lost in manually shredding plastics. HCEs should upgrade their inventories to the authorized numbers and deficiencies if any should be corrected on priority.
Overwhelming majority of hospitals have recommended for outsourcing as a viable method of disposal of bio-medical waste. A Comparative Study of Economics involved in common bio-medical waste treatment facility (CBWTF) versus individual setup by a private vendor (handling BMW of one Command hospital and one less than 300 bedded service hospital) has concluded that cost of running CBWTF is approx. 52.12% lower than running one's own facility.15 Outsourcing is being successfully carried out in four of our service HCEs.
Therefore, in cities where a State PCB approved vendor is available for outsourcing final disposal of BMW, the service HCEs should enter into a rate contract based on the rate approved by the local civic body. The basis of calculation should not be authorized beds but the average bed occupancy over the last three years,2 as has been done by one of our service hospital. The reasons for suggesting this are:-
-
(a)
In almost all our peace stations, facilities for outsourcing exist.
-
(b)
During our user survey, all HCEs in peace areas were for outsourcing the BMW.
-
(c)
The MOE&F and CPCB officials were unanimously of the opinion that with the pollutions norms for incinerators becoming more and more stringent, it would be economically and legally unviable for every hosp to have its own incinerator. Moreover, as our service hospitals are located in the vicinity of civil areas, the local civil authorities would not permit incinerators to operate in our set up. We could also have a problem with environmental activists.
-
(d)
Four of our own service hospitals have successfully outsourced their biomedical waste disposal.
-
(e)
The Draft BMW Rules 2011 have clearly outlined the duties of the vendor, thus ensuring that the legal liability of the Hospital Authority is restricted till the kerb site only.2
The approx rate for outsourcing comes to Rs 5 per bed per day (ranging from Rs 1.89 to Rs 8.60 depending on the classification of the city). This needs to be catered for by projecting for extra ACG from the Government. Entering into a rate contract would not be a problem as the rates have been fixed by the local civic body.
In Field areas and places not having outsourcing facilities for final disposal, ideally combination technologies could be a viable option. These could be combinations of chemical and shredder or shredder and autoclave, etc. However, even the Draft BMW Rules 2011 are silent on the use of combination technology for biomedical waste treatment. Therefore, it is felt that microwaves in use should be replaced by autoclaves (of appropriate sizes) in all HCEs as the former cannot treat metallic BMWs. Similarly, hydroclaves are expensive equipment with no additional tangible benefits and hence should be phased out. For the incinerable wastes, after the existing incinerators have outlived their lives, the service hospitals should use CBWTFs of the local civil hospitals. In case the same is not available, then deep burial is recommended.
Conclusion
For analysis of the BMW disposal network in the Armed Forces, a Systems Approach was undertaken. Since the AFMS took up the lead in proper disposal of BMW in the early part of this millennium, service HCEs, established their own disposal facilities. With the rapid advancement in health care industry in the civil, there are now plenty of vendors available who have established CBWTF in most cities. The civil HCEs have by and large reduced their own burden by outsourcing final BMW disposal to these approved vendors. The Armed Forces may also consider joining the “civil bandwagon” and thus reduce some of their legal and administrative liabilities.
Conflicts of interest
All authors have none to declare.
Acknowledgements
Office of DGAFMS.
References
- 1.Bhalwar R. 1st ed. Dept of Community Medicine, AFMC; Pune: 2009. Text Book of Public Health and Community Medicine. [Google Scholar]
- 2.Jindal A.K., Chatterjee A., Chatterjee K., Mahen A. Biomedical waste disposal: the way forward. MJAFI. 2011;67:309–310. doi: 10.1016/S0377-1237(11)60099-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ratcliffe J.W., Gonzalez de Valle. Rigor in health related research: towards an expanded conceptualization. Int J Health Serv. 1988;18(3) doi: 10.2190/E6E5-R0TP-PB1C-V4PK. [DOI] [PubMed] [Google Scholar]
- 4.Skeet, M. Report on meeting on the Role of Operational Studies in health services and education for these services, WHO: Project South East Asia Regional Organization 0116, WHO Regional Office for South East Asia, New Delhi.
- 5.Sharma Shalini. Awareness about bio-medical waste management among health care personnel of some important medical centers in Agra. Int J Environ Sci Develop. August 2010;1(3) [Google Scholar]
- 6.Yadavannavar M.C., Berad Aditya S., Jagirdar P.B. Biomedical waste management: a study of knowledge, attitude, and practices in a tertiary health care institution in Bijapur. Indian J Community Med. 2010 January;35(1):170–171. doi: 10.4103/0970-0218.62591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Patil A.D., Shekdar A.V. Health-care waste management in India. Indian J Environ Manage. October 2011;63(2):211–220. doi: 10.1006/jema.2001.0453. [DOI] [PubMed] [Google Scholar]
- 8.Rao S.K.M., Ranyal R.K., Bhatia S.S., Sharma V.R. Biomedical waste management: an infrastructural survey of hospitals. MJAFI. 2004;60:379–382. doi: 10.1016/S0377-1237(04)80016-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mastorakis Nikos E., Bulucea Carmen A., Oprea Tatiana A., Bulucea Cornelia A., Dondon Philippe. Environmental and health risks associated with biomedical waste management. Develop Energy Environ Economics. 2010:288–294. [Google Scholar]
- 10.Mohankumar S. Hospital waste management and environmental problems in India. IJPBA. 2011;2(6) [Google Scholar]
- 11.Passco Environmental Solutions Private Limited Pune, at: http://passco.in.
- 12.Singh K., Arora S.K., Dhadwal P.J., Singla A., John S. Bio-medical waste management in the U.T. Chandigarh J Environ Sci Eng. 2004 Jan;46(1):55–60. [PubMed] [Google Scholar]
- 13.Park K. 21st ed. m/s. Banrsidas Bharat Publishers; Jabalpur: 2009. Park's Text Book of Preventive and Social Medicine. [Google Scholar]
- 14.Draft Bio-Medical Waste (Management & Handling) Rules, 2011, at: http://moef.nic.in/downloads/public-information/salient-features-draft-bmwmh.pdf.
- 15.Maridi Eco Industries Private Limited Bangalore, at: www.icrihealth.com/ppt/Economic_Issues_Involved_BMW.pps.