

Introduction
Calcinosis cutis is an uncommon disorder caused by an abnormal deposit of calcium phosphate in the skin in various parts of the body.1 Four main types of calcinosis cutis have been recognized according to etiology: dystrophic, metastatic, iatrogenic and idiopathic.2 Very few cases of idiopathic calcinosis cutis have been reported in the literature.3
We report one such case of idiopathic calcinosis cutis.
Case report
A 2-year-old male child, the only product of a non-consanguineous marriage, presented to our hospital with complaints of multiple hard, raised, flat skin lesions since 4 months of age. The lesions first appeared on the back of the neck, gradually increased in number and size for a few months. Subsequently, the skin lesions decreased in size and finally healed. Similar lesions appeared on the thorax followed by right thigh, leg and foot. At present lesions in the thoracic region are decreasing in size but right lower extremity lesions are persisting. The lesions were not itchy nor was there any discharge. There was no history of bony swellings, bony deformity, fracture, and muscle weakness, pain in the joints or abnormal postures. The parents did not give history of failure to thrive, vomiting, seizures, and dysphagia. Also, there were no symptoms related to Raynaud's phenomenon, or photosensitivity. The child was born full term by normal vaginal delivery but with a low birth weight of 1.5 kg. The child was given top feeds but there was no history of excessive milk intake and developmental milestones were normal. No family member was suffering from similar illness.
General and systemic examinations were within normal limits. Dermatological examination revealed hard plaque like confluent lesions over chest wall, right thigh, knee, leg and foot (Figs. 1 and 2). A few lesions were also present on thorax and lower abdomen mostly on the right side.
Fig. 1.

Plaque like subcutaneous lesions on chest wall.
Fig. 2.

Plaque like subcutaneous lesions on leg and lower abdomen.
Investigations done revealed Hb to be 10.6 g %, reticulocyte count was 1.2%, liver function tests, blood urea S. creatinine and S. electrolytes were within normal limits. Parathyroid hormone assay was normal. Other investigations done were: S. calcium 8.7 mg/dl, phosphate 4.4 mg/dl, Alk phosphatase 489 IU/l (145–420), LDH 267 IU/l (150–500), Creatine Phosphokinase 83 IU/l (25–200), S. uric acid 7 mg/dl, urine spot calcium 4.2, creatinine 6.2 mg/dl, ANA-negative. X-ray showed soft tissue calcification around right hip, knee and ankle joint (Figs. 3 and 4) and features of sheet like calcification involving lower limb and chest wall on the right side. Histopathology of muscle biopsy was normal. Skin biopsy revealed deposits of calcium in the dermis with evidence of ossification, no foreign-body giant cell reaction, dermal adnexae unremarkable, no inflammatory infiltrate (Fig. 5).
Fig. 3.

Calcification around hip and knee joint.
Fig. 4.

Calcification around ankle joint.
Fig. 5.
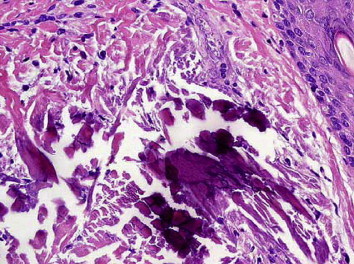
Biopsy of the lesion showing deposits of calcium in the dermis with evidence of ossification.
The case was diagnosed as a case of idiopathic calcinosis cutis and was put on Aluminum hydroxide gel 10 ml 4 times a day.
Discussion
Calcinosis cutis is a term used to describe a group of disorders in which aberrant calcium deposits form in the skin. Virchow initially described calcinosis cutis in 1855.4 It may be divided into 4 main groups, associated with localized or widespread tissue changes or damage (dystrophic calcification), that associated with an abnormal calcium and phosphorus metabolism (metastatic calcification), not associated with any tissue damage or demonstrable metabolic disorder (idiopathic calcification). Iatrogenic calcinosis cutis arises secondary to a treatment or a procedure.5
Idiopathic calcinosis cutis is a rare phenomenon and occurs in the absence of known tissue injury or systemic metabolic defect. Pathogenesis is not clearly understood and underlying mechanism is not known. It is postulated that there may be some abnormality in the metabolism of gamma carboxy glutamic acid (GCGA), a unique amino acid, which is normally found in bones and tissues. It has calcium and phospholipid binding properties. Probably GCGA gets deposited in the skin due to some aberration in its metabolism, leading to deposition of calcium phosphate in the skin.6
Very few cases of idiopathic calcinosis cutis are reported in early childhood in the literature. The various types of idiopathic calcinosis cutis are: Idiopathic calcinosis of scrotum/penis/vulva, Milia like idiopathic calcinosis cutis, sub epidermal calcified nodule, tumoral calcinosis, calcinosis cutis circumscripta and calcinosis universalis.
Investigations should be done to exclude any underlying pathology. Histological examination of the lesions reveals calcium deposits in the dermis on biopsy, which may or may not be surrounded by foreign-body giant cell reaction. Alternatively, massive calcium deposits may be located in the subcutaneous tissue. Small and medium-sized blood vessels may contain calcium deposits in areas of necrosis.4 Our case fits into the category of Idiopathic calcinosis cutis since no cause could be identified despite extensive investigations.
Medical therapy of calcinosis cutis is of limited and variable benefit. If secondary to any underlying disease the cause should be treated. Intralesional corticosteroids may be beneficial. Probenecid and colchicine have been useful in some patients. Magnesium or aluminum antacids may be effective phosphate binders in patients with hyperphosphatemia. However, use in patients with renal insufficiency may result in magnesium or aluminum toxicity.7 Sodium etidronate and diphosphonates may be helpful in some individuals by reducing bone turnover and inhibit the growth of ectopic hydroxyapatite crystals. However, treatment is prolonged and paradoxical hyperphosphatemia may result. Warfarin has shown benefit in some. There have been variably beneficial effects with the use of the calcium-channel blocker diltiazem over a period of at least 5 years. The therapeutic effect of this is believed to be the antagonism of the calcium–sodium ion pump.4 Introduction of low calcium diet, use of cellulose phosphate/sodium sulphate have been proposed by some authors but without much benefit.8
Indications for surgical removal include pain, recurrent infection, ulceration, and functional impairment. Because surgical trauma may stimulate calcification, initially treat a test site before a large excision is pursued. Following excision, however, recurrence is common.4
Conflicts of interest
All authors have none to declare.
References
- 1.Walsh J.S., Fairley J.A. Cutaneous mineralization and ossification. In: Wolff Klauss, Goldsmith L.A., Katz S.I., editors. Fitzpatrick's Dermatology in General Medicine. 7th ed. 2008. p. 1293. [Google Scholar]
- 2.Sato K., Nakamura T., Toyama Y., Ikegami H., Kameyama K., Takayama S. Idiopathic calcinosis cutis in fingertip treated with occlusive dressing using aluminum foil: a case report. Hand Surg. 2007;12(3):149–154. doi: 10.1142/S0218810407003602. [DOI] [PubMed] [Google Scholar]
- 3.Sardesai V.R., Gharpuray M.B. Calcinosis cutis. Indian J Dermatol Venereol Leprol. 2003;69(1):45–46. [PubMed] [Google Scholar]
- 4.Julia R Nunley, Lydia M E Jones. emedicine.medscape.com/dermatology. Updated 27 Jan 2009.
- 5.Moss J., Syrengelas A., Antaya R., Lazova R. Calcinosis cutis: a complication of intravenous administration of calcium gluconate. J Cutan Pathol. 2006;33(suppl 2):60–62. doi: 10.1111/j.1600-0560.2006.00519.x. [DOI] [PubMed] [Google Scholar]
- 6.Lanka P., Lanka L.R., Ethirajan N. Idiopathic calcinosis cutis. Indian J Dermatol. 2009;54(4):388–389. doi: 10.4103/0019-5154.57624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang Wen-Jen, Lo Wen-Lin, Wong Chu-Kwan. Calcinosis cutis in juvenile dermatomyositis: remarkable response to aluminum hydroxide therapy. Arch Dermatol. 1988;124:1721–1722. [PubMed] [Google Scholar]
- 8.Arora A., Agarwal A., Kumar S. Iatrogenic calcinosis cutis – a rare differential diagnosis of soft tissue infection in a neonate. J Orthop Surg. 2005;13(2):195–198. doi: 10.1177/230949900501300218. [DOI] [PubMed] [Google Scholar]