

Introduction
Placental site trophoblastic tumor (PSTT) is a rare form of gestational trophoblastic disease arising from invasive intermediate gestational trophoblasts and constitutes 1–2% of all GTN.1 Historically, it was first described in 1895 and was considered a benign lesion until Scully and Young recognized its malignant potential in 1981.2 Unlike other forms of gestational trophoblastic diseases it produces less quantity of beta HCG and is less chemo sensitive. Thus surgery is the mainstay of treatment. Adjuvant chemotherapy is increasingly being offered in cases of metastasis, high mitotic count and large tumor volume.2,3 In this case report we present a case of PSTT with vaginal and lung metastasis managed with surgery and adjuvant chemotherapy.
Case report
A 35-year-old, para 3, living 3, abortion 0 (P3L3A0) lady, presented with a recent history of irregular vaginal bleeding of six weeks duration. Her last delivery was 07 months ago. She had not undergone tubectomy. All her deliveries were normal without any antenatal or postnatal complications. Prior to her last pregnancy her periods were always regular. She was having lactational amenorrhea for six months after her last normal delivery. For the present illness she went to a local hospital with complaints of irregular bleeding per vaginum of two to three weeks duration where an ultrasonography showed thickened endometrium with no other abnormalities. A suction evacuation was carried out in a private hospital, the histopathology report of which was unavailable. She presented to this institution with persistent symptoms. On examination the patient was found to have some vaginal growths resembling skin tags (Fig. 1). The uterus was found to be bulky with no other abnormalities. A transvaginal sonography was suspicious for vesicular mole remnants which could not be confirmed. A Curettage done showed proliferative endometrium with only intermediate trophoblast cells in one fragment and was suggestive of Placental Site Trophoblastic Tumor (PSTT). The vaginal biopsy specimen showed similar nests of intermediate trophoblasts. The beta HCG level was mildly elevated to a value of 450 mIU/ml. X-ray chest was normal but CECT-scan Chest and CT abdomen showed heterogeneously enhancing mass lesions involving the uterus and evidence of pulmonary metastasis. There was no evidence of any retroperitoneal lymph node involvement on CECT Abdomen and Pelvis.
Fig. 1.

Gross photograph of vaginal growth.
A total abdominal hysterectomy with bilateral salpingo-oopherectomy was done. Postoperative recovery was normal. Repeat β-HCG following the surgery showed a fall to 339 mIU/ml. The histopathology examination of the specimen confirmed the diagnosis of Placental Site Trophoblastic Tumor with vaginal metastasis (Figs. 2–4) Stains for β-hCG and human placental lactogen (HPL) could not be done. After three weeks of surgery, the patient was started on combination chemotherapy. She was started on EMA-CO regime. Five cycles of chemotherapy was given following which the β-HCG value has fallen to 3 mIU/ml and repeat CECT chest and abdomen has shown resolution of pulmonary metastasis. The vaginal metastases have also resolved completely. She was given two more cycles of chemotherapy and is presently on follow up.
Fig. 2.
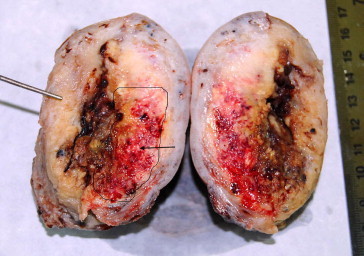
Gross photograph of cut section of uterus showing a diffusely infiltrating tumor in the uterine wall (outline and arrow).
Fig. 3.

Microphotograph showing infiltrating intermediate trophoblastic cells in the myometrium (H&E, 400×).
Fig. 4.

Microphotograph showing infiltrating intermediate trophoblastic cells in the vaginal wall (H&E, 400×).
Discussion
PSTT is a tumor of intermediate trophoblast. It is one of four trophoblastic lesions that arise from the intermediate trophoblast – the others being the exaggerated placental site reaction, placental site nodule and epithelioid trophoblastic tumor.1 PSTT can occur after any type of gestation. The duration from the preceding conception event is also highly variable.
Most patients present with abnormal bleeding per vaginum with varying periods of amenorrhea and/or effects of metastasis to various organs. A wide range of other presenting symptoms have been reported including galactorrhea, virilization, nephrotic syndrome, polycythemia and cutaneous metastases. It is difficult to distinguish between PSTT, ETT, and choriocarcinoma on the basis of clinical history and imaging alone.1 These patients often have persistent low levels of serum HCG (100–1000 mIU/mL). However, higher serum HCG titers have been reported in patients with placental site trophoblastic tumors.1,3 Initial curettage is often equivocal and the diagnosis can be missed if fragments showing muscle invasion by intermediate trophoblasts are not seen. Failure to respond or persistence of raised HCG levels in a GTN case treated with methotrexate can raise the suspicion of a PSTT.
Grossly it is a poorly circumscribed mass with a diffuse infiltration of intermediate trophoblasts between muscle fibers and around blood vessels. Invasion of the vessel wall with fibrinoid change and preservation of lumen can also be seen.1–4 Mitosis is variable and is an important prognostic differentiator.3,5 On immunohistochemistry, PSTT characteristically show a high proportion of cells positive for human placental lactogen (hPL) than positivity for human chorionic gonadotropin (hCG). The Ki-67 index, which is a surrogate marker for mitotic activity, shows 10–20% positivity in PSTT and is useful for differentiating this lesion from exaggerated placental site reaction where the Ki-67 index is less than 1% and choriocarcinoma, which shows >50% positivity.2,6 However estimations of serum HCG is still the most useful marker for investigation and follow up. A more recent marker for differentiating between choriocarcinoma and PSTT is the association of free non-hyperglycosylated β-hCG with PSTT, while in choriocarcinoma hyperglycosylated hCG is present and there is no free β-hCG.7 Imaging studies are useful especially when metastasis is present but are not specific as a diagnostic differentiator.
The clinical and biological behavior of PSTT is difficult to predict and no definitive prognostic index or scheme exits. The FIGO staging and WHO prognostic system for GTN are currently being used but do not correlate very well in PSTT. Poor prognostic factors are an interval of more than 2 years from known antecedent pregnancy, mitotic count >5/10 HPF, extensive necrosis and extension outside the uterus.5 Risk of death is reported 14 times greater if mitotic figures were greater than 5/10 HPF. High mitotic index is associated with not only metastatic disease but appears to be an indicator of recurrence too.3
Currently GTN are classified into non-metastatic, low-risk metastatic and high-risk metastatic categories.8 However as the biological behavior of PSTT is highly variable it does not fit into well defined prognostic groups, hence the first diagnostic and therapeutic intervention is usually surgical in the form of hysterectomy. Most patients with localized disease are effectively treated by total abdominal hysterectomy. With locally advanced or metastatic disease, tumor reductive surgery should be performed if disease is considered resectable.1,3,9
Non-metastatic tumors (FIGO Stage I) can be treated with a variety of single-agent methotrexate or actinomycin D protocols, resulting in cure of essentially all patients. In addition metastatic low-risk tumors (FIGO Stages II and III, WHO score <8) should be treated with 5-day dosage schedules of methotrexate and actinomycin D, with cure rates approaching 100%. Metastatic high-risk tumors (FIGO Stage IV, WHO score >7) require combination chemotherapy with etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine (EMA-CO) with or without adjuvant radiation therapy and surgery to achieve cure rates of 80–90%.1,8–12
Conclusion
PSTT is a rare subset of the Gestational trophoblastic neoplasms (GTN). Due to its rarity and varied biological behavior it presents a diagnostic challenge and treatment dilemma to both the pathologist and clinicians. It is important to make this specific diagnosis as it is distinct from other GTN. As it is relatively chemoresistant and has a varied prognosis, there is no consensus on appropriate chemotherapy especially in metastatic disease. A review of the current treatment protocols concluded that no firm conclusion about the best combination chemotherapy regimen for high-risk GTT exits. More high quality studies are required. Meanwhile institutions and centers develop and practice their own guidelines based on experience.
Conflicts of interest
All authors have none to declare.
References
- 1.Cole M.E., Broaddus R., Thaker P. vol. 5. March 2008. www.nature.com/clinicalpractice/onc (Placental-site Trophoblastic Tumors: A Case of Resistant Pulmonary Metastasis). no 3. [DOI] [PubMed] [Google Scholar]
- 2.Piura B. Placental site trophoblastic tumor – a challenging rare entity. Eur J Gynaecol Oncol. 2006;27(6):545–551. [PubMed] [Google Scholar]
- 3.Agarwal N., Parul Kriplani A., Vijayaraghavan M. Placental site trophoblastic tumour. J Postgrad Med [serial online] 2002;48:211–212. [cited 2009 Mar 5] [PubMed] [Google Scholar]
- 4.Gulati D., Bahal A., Tevatia M.S., Mehta A., Muttagikar M.P. Placental site trophoblastic tumour – a case report. Indian J Pathol Microbiol. 2006;49:281–283. [PubMed] [Google Scholar]
- 5.Baergen R.N., Rutgers J.L., Young R.H. Placental site trophoblastic tumor: a study of 55 cases and review of the literature emphasizing factors of prognostic significance. Gynecol Oncol. 2006;100(3):511–520. doi: 10.1016/j.ygyno.2005.08.058. [DOI] [PubMed] [Google Scholar]
- 6.Shih I.M., Kurman R.J. Molecular basis of gestational trophoblastic diseases. Curr Mol Med. 2002;2:1–12. doi: 10.2174/1566524023362960. [DOI] [PubMed] [Google Scholar]
- 7.Cole L.A., Dai D., Butler S.A., Leslie K.K., Kohorn E.I. Gestational trophoblastic diseases: pathophysiology of hyperglycosylated hCG. Gynecol Oncol. 2006;102:145–150. doi: 10.1016/j.ygyno.2005.12.047. [DOI] [PubMed] [Google Scholar]
- 8.Lurain J.R. Treatment of gestational trophoblastic tumors. Curr Treat Options Oncol Springer Boston. April, 2002;3(2):113–124. doi: 10.1007/s11864-002-0057-5. [DOI] [PubMed] [Google Scholar]
- 9.Hancock B.W., Welch E.M., Gillespie A.M., Newlands E.S. A retrospective comparison of current and proposed staging and scoring systems for persistent trophoblastic disease. Int J Gynecol Cancer. 2000;10:318–322. doi: 10.1046/j.1525-1438.2000.010004318.x. [DOI] [PubMed] [Google Scholar]
- 10.Escobar P.F., Lurain J.R., Singh D.K. Treatment of high-risk gestational trophoblastic neoplasia with etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine chemotherapy. Gynecol Oncol. 2003;91(3):552–557. doi: 10.1016/j.ygyno.2003.08.028. [DOI] [PubMed] [Google Scholar]
- 11.FIGO Oncology Committee FIGO staging for gestational trophoblastic neoplasia. Int J Obstet Gynecol. 2002;77:285–287. doi: 10.1016/s0020-7292(02)00063-2. [DOI] [PubMed] [Google Scholar]
- 12.Deng L., Yan X., Zhang J., Wu T. Combination chemotherapy for high-risk gestational trophoblastic tumour. Cochrane Database Syst Rev. 2006 doi: 10.1002/14651858.CD005196.pub3. Issue 3. Art. No.: CD005196. [DOI] [PubMed] [Google Scholar]