

Abstract
A young male patient was evaluated for a cardiac cause of ischaemic stroke. In the work-up, a tumour was detected on the subvalvular apparatus of the mitral valve for which operative removal was scheduled. A port-access procedure was applied as a novel way of treatment. On thoracoscopic intracardiac inspection, however, multiple tumours were seen attached to the chordae tendineae and to the anterior leaflet of the mitral valve. It was decided to not to perform a plasty but to remove the valve in toto and insert a mechanical valve prosthesis. The tumours were diagnosed as multiple giant Lambl's excrescences.
Background
Novel way of treatment; port-access mitralvalve replacement.
Multiple Lambl’s excrescences are rarely described in literature. In addition, to our knowledge, no report has been described multiple lesions that involved a relatively wide and mainly subvalvular area.
Case presentation
Apart from a history of one similar attack 2 months ago, a previously healthy 33-year-old man presented to the emergency department with transient symptoms of dysphasia and dizziness. The patient had always been at sinus rhythm. There was no previous hospitalisation with no conclusive medical or family history. As blood tests showed no infection, coagulopathy or vasculitis, and the patient did not appear to be ill, he was discharged and scheduled for further examination.
Investigations
A CT scan and MRI of the brain showed a recent ischaemic area in the right frontopariental region and the anterior part of the left thalamus. In order to evaluate a possible cardiac source of embolism echocardiography was performed. Transthoracic echocardiography (TTE) and transoesophageal echocardiography (TOE) revealed a solitary tumour (6×9 mm) attached to the chordae tendineae of the anterior leaflets of the mitral valve (figure 1).
Figure 1.

Transoesophageal echocardiography: solid tumour (arrow) attached to the subvalvular apparatus of the mitralvalve.
Differential diagnosis
Initially, the list of differential diagnosis included also other causes of juvenile stroke as patent foramena ovale, atrial fibrillation, vascular malformation at the base of the brain, coagulation and blood disorders.
Treatment
Since the patient had suffered two clinical episodes of ischaemic stroke, he was scheduled for cardiac surgery to remove the tumour through a port access (figures 2 and 3). Cardiopulmonary bypass was accomplished by double percutaneous cannulation of the right femoral vein and the right internal jugular veins, while the arterial cannulation was performed through the left femoral artery. Exposure of the heart was achieved by an endoscopic approach through four small incisions (figures 2 and 3) as usual in the port-access procedure.
Figure 2.

Four small intercostal incisions are being made between the mid-axillar and mid-clavicular line.
Figure 3.
Endoscopic surgery.
Once the left atrium was opened, a round-shaped tumour was identified. However, further inspection revealed multiple small-sized tumours situated along the full size of the chordae tendineae of the anterior leaflet of the mitral valve (figure 4). While, it seemed not possible to remove all the tumours selectively, the decision was made to replace the mitral valve after total chordae tendineae excision. The pathological examination of the excised tumours revealed its origin to be that of giant Lambl’s excrescences (figure 5).
Figure 4.
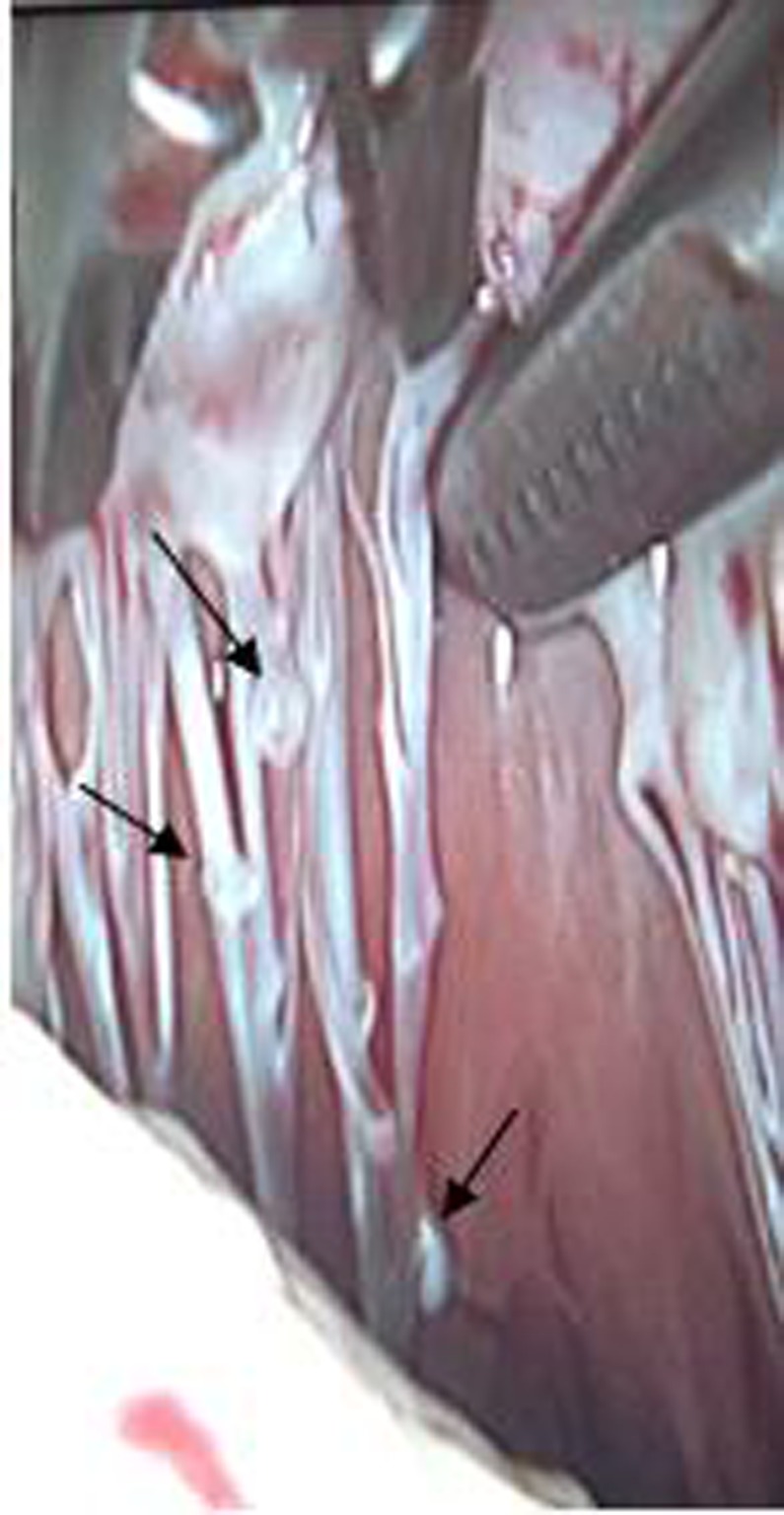
Multiple small tumours situated along the choldae tendinae.
Figure 5.
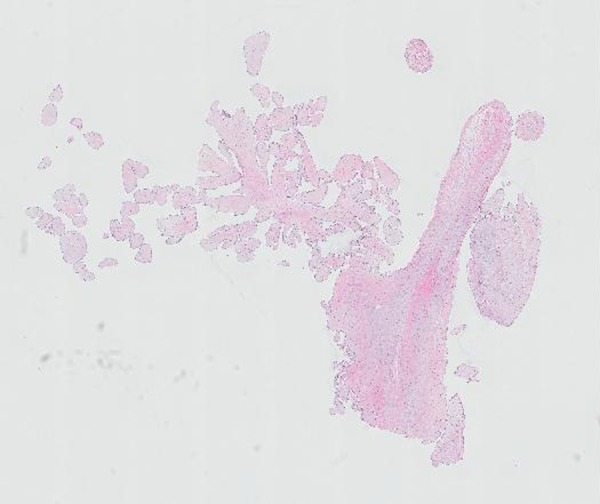
Histology of Lambl's excrescences: tumours situated along the choldae tendinae.
Outcome and follow-up
The procedure and postoperative recovery were uneventful.
Discussion
Lambl’s excrescences are rare cardiac structures, mostly described as filiform fronds usually occurring at sites of valve closure with a potential for embolisation. These tumours may be an incidental finding1 or can be a rare cause of stroke,2–5 or coronary artery obstruction.6 Histologically, they are composed of a cellular fibroelastic core covered by a layer of endothelial cells, and have to be distinguished from cardiac myxomas7 and fibroelastomas,8 9 of which the latter had been reported to be presented as ischaemic stroke.10 11
In general, the larger the tumour, the more likely it is that its presence will be detected, TOE being superior over TTE. However, as this case shows, small tumours, especially those located subvalvular, can be very difficult to visualise by echo.12 In this patient, only one tumour on the chordae tendineae was observed by TOE, while during surgery multiple smaller tumours were detected.
Multiple Lambl’s excrescences are rarely described in the literature. In addition, to our knowledge, no report has described multiple lesions that involve a relatively wide and mainly subvalvular area. This could be due to the fact that the spatial resolution of echocardiography is too low to detect these smaller lesions. Moreover, during conventional open heart surgery, small tumours which are situated just under the valve leaflets may be easily missed, while in the port-access setting, the visual exposure of the chordae tendineae is much better.
What is also remarkable in this patient was the site of these tumours. Lambl’s excrescences are mostly described as preferably located at the sites of valve closure,1 13 14 and extremely rare at the papillary muscles.15 To our knowledge, multiple lesions situated along the chordae tendineae of the mitral valve were not described before. The current hypothesis is that wear and tear damage to the endothelium occurs at the site of contact between the valvular margins and the endocardial surfaces. Subsequently, small thrombi evolve and form the filiform fronds of Lambl's excrescences.16 17 The diffuse multiple lesions seen in this patient suggest that this hypothesis cannot be the sole explanation to the pathogenesis of these tumours.
Learning points.
Lambl's excrescences can present as multiple lesions involving not merely the valvular but also the subvalvular regions of the heart. Owing to its small size and uncommon location, these lesions can be difficult to visualise by echocardiography. Therefore, a careful examination during surgery should be performed to evaluate a possible extravalvular involvement. Endoscopic surgery seems to provide a superior visualisation compared with the standard approach.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Voros S, Nanda NC, Thakur AC, et al. Lambl's excrescences involving the pulmonary valve detected by transesophageal echocardiography. Echocardiography 1999;16:35–9 [DOI] [PubMed] [Google Scholar]
- 2.Wu TY, Gerber IL, Roxburgh RH. Thrombo-embolic cerebral infarction secondary to giant Lambl's excrescence. J Clin Neurosci 2013;20:1632–4 [DOI] [PubMed] [Google Scholar]
- 3.Kalavakunta JK, Peddi P, Bantu V, et al. J Heart Valve Dis 2010;19:669–70 [PubMed] [Google Scholar]
- 4.Liu RZ, Yu SY, Li Y. Migraine-like headache and ischemic strokes in two patients with Lambl's excrescences. Chin Med J (Engl) 2012;125:3346–8 [PubMed] [Google Scholar]
- 5.Aggarwal A, Bruce JL. Giant Lambl's excrescences. N Engl J Med 2003;349:e24. [DOI] [PubMed] [Google Scholar]
- 6.Dangas G, Dailey-Sterling FG, Sharma SK, et al. Non-Q-wave infarction and ostial left coronary obstruction due to giant Lambl's excrescences of the aortic valve. Circulation 1999;99:1919–21 [DOI] [PubMed] [Google Scholar]
- 7.Magaray FR. On the mode of formation of Lambl's excrescences and their relation to chronic thickening of the mitral valve. J Pathol Bacteriol 1949;61:203–8, 5 [DOI] [PubMed] [Google Scholar]
- 8.Boone SA, Campagna M, Walley VM. Lambl's excrescences and papillary fibroelastomas: are they different? Can J Cardiol 1992;8:372–6 [PubMed] [Google Scholar]
- 9.Jaffe W, Figueredo VM. An example of Lambl's excrescences by transesophageal echocardiogram: a commonly misinterpreted lesion. Echocardiography 2007;24:1086–9 [DOI] [PubMed] [Google Scholar]
- 10.Mishra PK, Davison P, Lakshmanan S, et al. Ventricular mass: a clinical and surgical conundrum. BMJ Case Rep 2011;2011.10.1136/bcr.04.2010.2875 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tejada J, Galiana A, Balboa O, et al. Mechanical endovascular procedure for the treatment of acute ischemic stroke caused by total detachment of a papillary fibroelastoma. BMJ Case Rep 2013.10.1136/neurintsurg-2013-010800.rep [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Samal AK, Nanda N, Thakur AC. Three-dimensional echocardiographic assessment of Lambl's excrescences on the aortic valve. Echocardiography 1999;16:437–41 [DOI] [PubMed] [Google Scholar]
- 13.Morgan JA, Paone G. Resection of Lambl's excrescence on the aortic valve in a patient with rheumatic mitral valve disease and a left atrial thrombus. Heart Surg Forum 2012;15:E215–17 [DOI] [PubMed] [Google Scholar]
- 14.Aziz F, Baciewicz FA., Jr Lambl's excrescences: review and recommendations. Tex Heart Inst J 2007;34:366–8 [PMC free article] [PubMed] [Google Scholar]
- 15.Pomerance A. Papillary “tumours” of the heart valves. J Pathol Bacteriol 1961;81:135–40 [DOI] [PubMed] [Google Scholar]
- 16.Bhagwandien NS, Shah N, Costello JMJ, et al. Echocardiographic detection of pulmonary valve papillary fibroelastoma. J Cardiovasc Surg (Torino) 1998;39:351–4 [PubMed] [Google Scholar]
- 17.Wolf RC, Spiess J, Vasic N, et al. Valvular strands and ischemic stroke. Eur Neurol 2007;57:227–31 [DOI] [PubMed] [Google Scholar]