

Abstract
Aim/background
To evaluate how the use of volumetric-modulated arc therapy (VMAT) with RapidArc® can improve treatment delivery efficiency based on the analysis of the beam-on times and monitor units (MU) needed to deliver therapy for multiple clinical applications in a large patient population.
Materials and methods
A total of 898 treatment courses were delivered in 745 patients treated from October 2008 to March 2013 using RapidArc® treatment plans generated in Eclipse™ TPS. All patients were treated with curative or palliative intent using different techniques including conventional fractionation (83%) and radiosurgery or SBRT (17%), depending on the clinical indications. Treatment delivery was evaluated based on measured beam-on time and recorded MU values delivered on a Varian Trilogy™ linear accelerator.
Results
For conventional fractionation treatments using RapidArc®, the delivery times ranged from 38 s to 4 min and 40 s (average 2 min and 6 s). For radiosurgical treatments the delivery times ranged from 1 min and 42 s to 9 min and 22 s (average 4 min and 4 s). The average number of MU per Gy was 301 for the entire group, with 285 for the conventional group and 317 for the radiosurgical group.
Conclusions
In this study with a large heterogeneous population, treatments using RapidArc® were delivered with substantially less beam-on time and fewer MUs than conventional fractionation. This was highly advantageous, increasing flexibility of the scheduling allowing treatment of radiosurgery patients during the regular daily work schedule. Additionally, reduction of leakage radiation dose was achieved.
Keywords: IMRT, RapidArc, VMAT, SBRT, SRS, Treatment Planning software
1. Introduction
1.1. Background
RapidArc® (Varian Medical Systems, Palo Alto, CA) is a novel technique developed to deliver highly focused volumetric-modulated arc therapy6 approved for clinical use in 2008 [1]. The basic concept of arc therapy is the delivery of radiation from a continuous rotation of the radiation source. In the case of RapidArc® it delivers a precisely sculpted 3D dose distribution with a 360° rotation of the accelerator gantry made possible by a treatment planning algorithm that varies simultaneously 3 parameters during treatment: (1) gantry rotation speed, (2) treatment aperture shape using the movement of multileaf collimator leaves and (3) delivery dose rate [2]. This technique can achieve highly conformal dose distributions with improved target volume coverage and sparing of normal tissues compared with conventional radiotherapy techniques. In addition, it also has the potential to offer reduced treatment delivery time and less MUs compared with conventional static field intensity modulated radiotherapy.7
In the case of radiosurgery, delivery of high-dose-per-fraction SRS or SBRT with multi-field IMRT can be highly time-consuming because of the many beam angles required to conform to the target shape and the large number of monitor units8 needed to deliver the dose [3].
In this retrospective review we analyze the beam-on times and MU per fraction needed to deliver therapy with RapidArc® at several sites in a large patient population of multiple clinical applications including conventional fractionation and radiosurgery/SBRT.
2. Materials and methods
From October 2008 to March 2013 a total of 745 patients received 898 treatment courses using RapidArc®: 749 (83%) with conventional fractionation and 149 (17%) with radiosurgery/SBRT. Diagnosis and treatment sites characteristics are shown in Table 1. For conventional RapidArc® the number of arcs ranged from 1 to 5, but most frequently 2 arcs were used. For RapidArc® Radiosurgery/SBRT the number of arcs ranged from 2 to 6 depending on the size, location, and volume of the target. Partial arcs and multiple coplanar/non-coplanar arcs were used depending on the case specification (see Table 2).
Table 1.
Total number of RapidArc® treatment courses/site.
| Site/diagnosis | No. treatment courses |
|---|---|
| Prostate | 156 |
| Gynecological | 137 |
| Lung | 106 |
| H/N | 91 |
| Spine | 87 |
| Pelvis | 87 |
| Brain | 60 |
| Abdomen | 58 |
| Chest | 19 |
| Breast | 18 |
| Liver | 18 |
| Rectum | 17 |
| Skin | 15 |
| Bladder | 11 |
| Pancreas | 10 |
| Esophagus | 8 |
| Total | 898 |
Table 2.
Range and average values of beam-on time for conventional fractionation and SRS/SBRT using RapidArc®.
| Beam-on time | Conventional | SRS/SBRT |
|---|---|---|
| Min | 0.63 | 1.7 |
| Max | 4.68 | 9.36 |
| Average | 2.08 | 4.06 |
Patient specific quality assurance9 was performed prior to first day of treatment delivery using a XWU-IMRT Phantom (Best Medical Canada Ltd.) with MOSFETS and film dosimetry and/or the ArcCHECK® System (Sun Nuclear Corporation). Dose agreement was within 3%.
Patients were selected for RapidArc® following the same indications as conventional IMRT: anytime that critical structure protection required the creation of complex dose distributions; if the target volume was irregularly shaped and in close proximity to critical structures that needed to be protected, the volume of interest was covered with narrow margins to adequately protect immediately adjacent structures; an immediately adjacent area that had been previously irradiated and abutting portals were established with high precision in all cases of salvage radiation. Several fractionation schemes were used depending on the indications. One, 3, or 5 fractions were delivered in radiosurgery/SBRT, and anywhere from 15 to 45 daily fractions for conventional regimens. In general for conventional treatments, shorter schemes where used for palliative cases and longer ones for curative intent.
All patients were treated using a Trilogy™ Linear accelerator (Varian Medical Systems, Palo Alto, CA) with energies of 6 or 16 MV and a 120 multi-leaf collimator, planned with Eclipse™ system using inverse treatment planning. Cone Beam CT (CBCT)10 was used daily for image guidance before delivering the treatment.
For treatment planning, CT simulation was acquired with various immobilization devices including customized Aquaplast and body-frame. For head and neck, thoracic and CNS tumors IV contrast was routinely used to aid tumor delineation unless contraindicated. The gross and/or clinical tumor volume11,12 were defined using CT, MRI, and/or PET/CT. MRI was used in most CNS and in GYN patients unless contraindicated. PET/CT was generally used, particularly for lung and head and neck tumors. RTOG guidelines for treatment and normal tissue constrains were used.
For comparison purposes, we reviewed the data of a group of 19 patients who were treated with conventional IMRT in our institution prior to the implementation of the RapidArc® system.
The treatment time and MUs for every treatment were extracted from the patients’ electronic medical record in ARIA®.
Fig. 1.
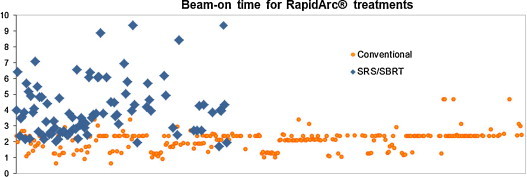
Beam-on times for all patients treated in our center with RapidArc®. The orange and blue points show the times for conventional fractionation and SRS/SBRT, respectively. The time range and average is shown in Table 2.
3. Results
When using RapidArc® for conventional treatments, the delivery times ranged from 38 s to 4 min and 40 s (average 2 min and 6 s). For radiosurgical/SBRT treatments using RapidArc® the delivery times ranged from 1 min and 42 s to 9 min and 22 s (average 4 min and 4 s). Due to the short treatment time there was no need to significantly modify the schedule when radiosurgery/SBRT procedures were performed. The average number of MUs per Gy was 301 for the entire group, with 285 for the conventional group and 317 for the radiosurgical group. Acute toxicity was minimal even in patients undergoing systemic chemotherapy. In the conventional IMRT group, 12 patients were treated for prostate cancer, 4 for head and neck cancer, and 3 for lung cancer. The comparison of these groups as seen in Fig. 2 showed that MUs were reduced by 45% in prostate cancer, 58% in head and neck cancer, and 39% in lung cancer.
Fig. 2.
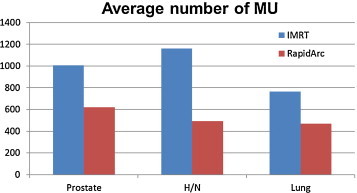
Comparison of the average number of MUs in patients treated with RapidArc® and IMRT for prostate, head and neck, and lung cancer in our institution.
4. Discussion
IMRT represented a significant advance in conformal Radiotherapy allowing the delivery of dose distributions with complex isodose profiles as reported in 2000 by Nutting et al. [4].
The advantages of this technique were clearly demonstrated in early reports particularly in head and neck cancer cases where sparing of the salivary glands was successfully accomplished. IMRT provides better dose distribution in the target volume and lower dose for organs at risk, such as for the parotid glands [5].
However, a good conventional IMRT often requires more fixed fields with higher MUs, resulting in lengthy treatment delivery times. The development of RapidArc® software has included many of the IMRT benefits, but given in shorter treatment times. In a recently published study, 20 patients with nasopharyngeal tumors treated by Zheng et al. [6] using RapidArc® showed better dosimetry compared with conventional IMRT. In their study, two treatment plans were developed for each patient, one with RapidArc® and the other with fixed 9-field coplanar dynamic IMRT. The Eclipse™ system was used for both plans with 6 MV-energy and a 120 multi-leaf collimator. The mean treatment time of RapidArc® and IMRT was 165 versus 447 s. The mean MU values of RapidArc® and IMRT were 550 and 1379 respectively. Comparing to IMRT, the delivery time and the MU values of RapidArc® were reduced by 63% and 60%, respectively [6] In the case of prostate cancer treated with RapidArc®, Yoo et al. [7] recently reported a reduction of MUs ranging from 37% to 66% depending on the number of arcs and the primary and boost plan. With the comparable equipment, our experience is in agreement with both of these studies: the reduction in MUs was 58% for head and neck cancer and 45% for prostate cancer in our patient population treated with RapidArc®.
We reviewed our preliminary data in intrathoracic tumors from October 2008 to March 2012. Eighty-one treatment courses in 62 patients with thoracic tumors: 53 using conventional fractionation, 25 using SBRT, and in 3 patients for Lattice Radiation Therapy. In conventional fractionation planning we used between 1 and 4 arcs, mostly 2 arcs. The dose per fraction ranged from 1.8 Gy to 3 Gy. The average number of MUs per Gy was 260. Treatment times ranged from 1.1 min to 2.9 min depending on the total arc length. For SBRT, 4 non-coplanar partial arcs were typically used. The number of arcs ranged from 1 to 6. An average of 330 MU/Gy was resulted and the “beam-on” time ranged from 2.2 to 10.3 min depending on the number of MUs used. Dose per fraction ranged from 5 to 20 Gy given in 1–5 fractions. Acute toxicity was minimal for all the patients. No interruptions during the course of treatment occurred for patients who had a high Karnofsky score and the treatments were well tolerated. Reproducibility of the patient setup was achieved using IGRT/CBCT. The shorter treatment time eased patient's tolerance and minimized movement during treatment. No acute toxicity was encountered in this series of patients treated with RapidArc® [8].
In Ong et al's study of stereotactic radiotherapy for peripheral lung tumors the average MUs per Gy was 240 with VMAT versus 445 with IMRT [9]. This is close to our results of 330 MU per Gy for SRS/SBRT patients using RapidArc®. Our comparison of lung conventional fractionation with RapidArc® versus IMRT resulted in an average reduction from 425 MU/Gy with IMRT to 260 MU/Gy with RapidArc®.
Rapid delivery of SRS and SBRT with RapidArc® improves workflow on the Linac and minimizes the potential for intrafraction organ and patient motion.
5. Conclusions
In this study of a large heterogeneous population using RapidArc®, substantially less beam-on time and fewer MUs than conventional fractionation were observed. Our results support several benefits including reduction of leakage radiation dose with potential decrease of risk of secondary malignancies, less intra-fraction movement and more accurate treatment delivery. The treatment time reduction was highly advantageous allowing more flexibility of treating radiosurgery patients without altering the regular daily work schedule.
Use of RapidArc® for conventional fractionation, SRS, and SBRT improved the efficiency of our radiation therapy practice with great patient acceptance. This technology also improves cost-effectiveness compared with other more time-consuming radiation techniques. These benefits may potentially represent significant cost savings for our healthcare system while providing better access to radiation treatments, increasing patient convenience, and boosting quality of life for patients.
Financial disclosure statement
All authors are members of the Speaker Bureau of Varian Medical Systems; however, they received no financial support for their work on this manuscript.
Conflict of interest statement
All authors declare no conflict of interest regarding the preparation of this manuscript.
Acknowledgments
The authors would like to thank Christina Cascante for providing assistance with manuscript preparation.
Footnotes
Volumetric-modulated arc therapy (VMAT).
Intensity modulated radiotherapy (IMRT).
Monitor unit (MU).
Quality assurance (QA).
Cone Beam CT (CBCT).
Gross tumor volume (GTV).
Clinical tumor volume (CTV).
References
- 1.Otto K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med Phys. 2008;35:310–318. doi: 10.1118/1.2818738. [DOI] [PubMed] [Google Scholar]
- 2.Teoh M., Clark C.H., Wood K., Whitaker S. Volumetric modulated arc therapy: a review of current literature and clinical use in practice. Br J Radiol. 2011;84:967–996. doi: 10.1259/bjr/22373346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Roa D.E., Schiffner D.C., Zhang J. The use of RapidArc® volumetric-modulated arc therapy to deliver stereotactic radiosurgery and stereotactic body radiotherapy to intracranial and extracranial targets. Med Dosim. 2012:257–264. doi: 10.1016/j.meddos.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 4.Nutting C., Dearnaley D.P., Webb S. Intensity modulated radiation therapy: a clinical review. Br J Radiol. 2000;73(May (869)):459–469. doi: 10.1259/bjr.73.869.10884741. [DOI] [PubMed] [Google Scholar]
- 5.Kam K.M., Chau R.M., Suen J. Intensity modulated radiotherapy in nasopharyngeal carcinoma: dosimetric advantage over conventional plans and feasibility of dose escalation. Int J Radiat Oncol Biol Phys. 2003;56:145–157. doi: 10.1016/s0360-3016(03)00075-0. [DOI] [PubMed] [Google Scholar]
- 6.Zheng B.M., Dong X.X., Wu H. Dosimetry comparison between volumetric modulated arc therapy with RapidArc® and fixed field dynamic imrt for local-regionally advanced nasopharyngeal carcinoma. Chin J Cancer Res. 2011;23(December (4)):259–264. doi: 10.1007/s11670-011-0259-0. doi: 10.1007/s11670-011-0259-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yoo S., Wu Q.J., Lee W.R., Yin F.F. Radiotherapy treatment plans with RapidArc® for prostate cancer involving seminal vesicles and lymph nodes. Int J Radiat Oncol Biol Phys. 2010 Mar 1;76(3) doi: 10.1016/j.ijrobp.2009.07.1677. doi: 10.1016/j.ijrobp.2009.07.1677. Epub 2010 January 8. [DOI] [PubMed] [Google Scholar]
- 8.Amendola B.E., Amendola M., Perez N. Volumetric modulated arc therapy (VMAT) reduces treatment time compared to conventional intensity modulated radiation treatment (IMRT) of thoracic tumors. J Thorac Oncol. 2012;7(September (9)):S264. [Google Scholar]
- 9.Ong C.L., Verbakel W.F., Cuijpers J.P. Stereotactic radiotherapy for peripheral lung tumors: a comparison of volumetric modulated arc therapy with 3 other delivery techniques. Radiother Oncol. 2010;97(December (3)):437–442. doi: 10.1016/j.radonc.2010.09.027. doi: 10.1016/j.radonc.2010.09.027. Epub 2010 November. [DOI] [PubMed] [Google Scholar]