

Abstract
Priapism is a persistent penile erection that continues for hours beyond, or is unrelated to, sexual stimulation. Priapism requires a prompt evaluation and usually requires an emergency management. There are two types of priapism: 1) ischemic (veno-occlusive or low-flow), which is found in 95% of cases, and 2) nonischemic (arterial or high-flow). Stuttering (intermittent or recurrent) priapism is a recurrent form of ischemic priapism. To initiate appropriate management, the physician must decide whether the priapism is ischemic or nonischemic. In the management of an ischemic priapism, resolution should be achieved as promptly as possible. Initial treatment is therapeutic aspiration with or without irrigation of the corpora. If this fails, intracavernous injection of sympathomimetic agents is the next step. Surgical shunts should be performed in cases involving failure of nonsurgical treatment. The first management of a nonischemic priapism should be observation. Selective arterial embolization is recommended for the management of nonischemic priapism in cases that request treatment. The goal of management for stuttering priapism is prevention of future episodes. This article provides a review of recent clinical developments in the medical and surgical management of priapism and an investigation of scientific research activity in this rapidly developing field of study.
Keywords: Erectile dysfunction, Priapism, Surgery
INTRODUCTION
Priapism is defined as complete or partial penile tumescence that continues for 4 or more hours beyond sexual stimulation or that is not associated with sexual stimulation [1-3]. Typically, only the corpora cavernosa are affected without involvement of the corpus spongiosum and glans. The causes of priapism include various and apparently unrelated conditions. One larger study indicated that most cases of priapism were idiopathic: whereas 21% were associated with alcohol or drug abuse, 12% were associated with perineal trauma, and 11% were associated with sickle cell disease [4]. After the mid-1980s, intracavernous self-injection of drugs, such as phentolamine, prostaglandin, and papaverine, has become one of the main causes of priapism [5]. Whatever the cause, early involvement of a urologist in the patient's care is important.
Priapism can be ischemic (low-flow, veno-occlusive), nonischemic (high-flow, arterial), or stuttering (intermittent, recurrent ischemic). Each type of priapism has a distinctly different pathophysiological cause. Consequently, the options for treatment for the different types of priapism also differ. This retrospective review will focus on the current medical and surgical management of the different types of priapism.
DEFINITIONS
Priapism needs prompt evaluation and may require emergency management.
1. Ischemic (veno-occlusive or low-flow) priapism
Ischemic priapism, which accounts for 95% of priapism [1], is a persistent, nonsexually related erection characterized by a reduction or absence of intracavernous blood flow and marked by rigidity of the corpora cavernosa with little or no cavernous arterial inflow. Typically, painful and fully rigid corpora cavernosa with little or no involvement of the corpus spongiosum and glans penis is clinical evidence of ischemic priapism [5]. Analysis of cavernous blood gas shows acidosis and hypercarbia. Irreversible corporal damage occurs after 4 to 6 hours of ischemia [6]. Ischemic priapism is a compartment syndrome typified by a pressure within the closed space of the corpora cavernosa, intensely compromising circulation in the cavernous tissues.
A diversity of ischemic priapism is stuttering (intermittent or recurrent) priapism. Stuttering priapism causes recurrent unwanted, persistent, and painful erection with intervening periods of detumescence. This priapism often requires multiple visits to an emergency medical center for management. These episodes are often self-limiting and terminate within 3 hours [7]. Each episode carries a risk of fibrotic injury to the corpora cavernosa if the priapism continues and is not reduced promptly. The prevalence of stuttering priapism is greater in patients with sickle cell disease owing to hyperviscosity, increased adhesiveness of the blood to the vascular endothelium, and disrupted vascular homeostasis [8,9].
2. Nonischemic (arterial, high-flow) priapism
Nonischemic priapism is a persistent, nonsexual erection that is not considered an emergency. It is induced by an arteriolar-sinusoidal fistula causing unregulated arterial inflow, bypassing the regulatory, highly resistant helicine arteries to the corpora cavernosa [10]. Typically, the corpora cavernosa are not fully rigid, tender, or painful and cavernous blood gases are not hypoxic or acidotic. Antecedent perineal or penile trauma is the most common cause. The cavernous tissue is well oxygenated and the erection is usually painless; therefore, nonischemic priapism is not a medical emergency.
EVALUATION
The evaluation includes clinical history, physical examination, and other diagnostic procedures in order to define the clinical presentation and for development of a treatment plan. Most importantly, in diagnostic evaluation, distinguishing between ischemic and nonischemic priapism is critical because the former represents a urological emergency. Early treatment of ischemic priapism can be initiated on the basis of various clinical features even when awaiting confirmatory results of laboratory and radiologic study [4].
Corporal aspiration and blood gas analysis is mandatory [1]. Results of blood gas analysis demonstrating acidosis (pH<7.25), hypoxia (PO2<30 mmHg), hypercapnia (PCO2>60 mmHg), or glucopenia can validate the diagnosis of ischemic priapism [4]. Priapism is deemed nonischemic if the results of the corporal blood gas analysis are consistent with normal arterial blood gas values (pH, 7.4; PO2, >90 mmHg; PCO2, <40 mmHg) [11].
Use of color Doppler ultrasonography (CDU) of the perineum and penis is not routine; however, it can be useful in diagnosis of both ischemic and nonischemic priapism in experienced hands. Typically, in ischemic priapism, there is little or no demonstrable arterial flow within the corpora cavernosa [12]. The normal, high, unregulated, or turbulent cavernosal arterial flow or even an arteriolar-sinusoidal fistula or pseudoaneurysm is firmly suggestive of nonischemic priapism [4,13]. Performance of CDU may also be advantageous in evaluation of the effect of management for ischemic priapism in the partially detumescent penis [13]. In this case, the evaluation can lead to further intervention if necessary owing to the finding of persistent ischemia or the consideration of other diagnostic possibilities such as resolved ischemia with penile edema or conversion to high-flow priapism. The study should be performed with placement of the patient in the lithotomy or frog-leg position in order to scan the perineum first and then the entire penile shaft. This technical feature acknowledges the possibility that an abnormality could occur in the perineal portion of the corpora cavernosa in circumstances of a straddle injury or direct scrotal damage [1,4,13].
For the initial diagnosis of priapism, penile arteriography is not used. It is performed to identify the site of a supposed arteriocavernous fistula in men with nonischemic priapism. Penile arteriography is usually used in conjunction with management of a fistula by embolization [13].
Currently, there has been interest in the use of magnetic resonance imaging (MRI) in patients with priapism because MRI produces excellent findings of the corpora cavernosa. However, MRI is not practical in the initial diagnosis of priapism, although it may be useful in imaging for unusual cases of priapism [1,14].
MANAGEMENT
The treatment schema for priapism initiates with the diagnostic differentiation of the clinical features as either ischemic or nonischemic priapism. The objective in the management of ischemic priapism is relief of the compartment syndrome of the penis. In the management of stuttering priapism, the objective is similar but also features ischemic effects. In contrast, in cases of nonischemic priapism, the objective is to cure the priapism without a need to relieve ischemia. For all types of priapism, the overarching objectives are maintenance of penile flaccidity in nonsexual conditions and retention of normal erectile ability for sexual activity when needed [1,4,15]. A management algorithm summary is shown in Fig. 1.
FIG. 1.

Management algorithm for priapism.
1. Ischemic (veno-occlusive or low-flow) priapism
1) Nonsurgical treatment
Conservative management alternatives, including ejaculation, micturition, ice-pack application, gentle exercise, oxygen, and hydration, have been showed to result in achievement of detumescence, possibly by reflex vasoconstriction. However, evidence to support the recommendation of these management alternatives is limited [1]. Oral sympathomimetics, e.g., etilefrine, phenylephrine, metaraminol, and terbutaline, are superior to placebo if prescribed within a short time frame (<4 hours) after onset, with achievement of detumescence in 28% to 36% of patients [1,9,16]. Nevertheless, there is scant evidence to support the application of oral sympathomimetics, and conservative management should not hold up corporal aspiration with or without intracavernosal treatment [11].
2) First-line treatment: corporal aspiration
Aspiration of corporal blood with or without saline irrigation has a 30% chance of resulting in termination of priapism [11]. After administration of penile anesthesia (dorsal nerve block or local penile shaft block), a 19 or 21 G butterfly needle is inserted into the corpus cavernosum at the peno-scrotal junction laterally at the 3 or 9 o'clock site to avoid damage of the dorsal neurovascular bundle [4,10]. The needle must penetrate the skin, subcutaneous tissue, and the tunica albuginea to enter the corpus cavernosum. It is important to persist with aspiration until fresh red, oxygenated blood is aspirated.
3) Second-line treatment: intracavernosal sympathomimetics
Intracavernosal sympathomimetics (Table 1) can stimulate contraction of cavernous smooth muscle for achievement of detumescence [17]. The reported overall success rate is up to 80% depending on the duration of priapism [18]. A lower response rate is predicted if the duration of corporal ischemia is >72 hours, because there is evidence that, despite exposure to alpha agonists, anoxia, acidosis, and glucopenia further impair contraction of cavernosal smooth muscle [19]. Options for sympathomimetic agents include phenylephrine, etilefrine, ephedrine, norepinephrine, and metaraminol, although the specific agent used may depend on pharmaceutical availability in various regions of the world [11]. To minimize undesired cardiac inotrophic and chronotrophic side-effects, phenylephrine, a selective alpha-1 adrenergic receptor agonist, is recommended [17]. Heart rate and blood pressure should be monitored closely owing to the potential for development of cardiac dysrhythmia [1]. Phenylephrine (200 µg) can be injected every 5 to 10 minutes to a maximum dose of 1 mg [7,15]. Higher doses of phenylephrine can be considered in younger patients without cardiovascular disease risk factors [20].
TABLE 1.
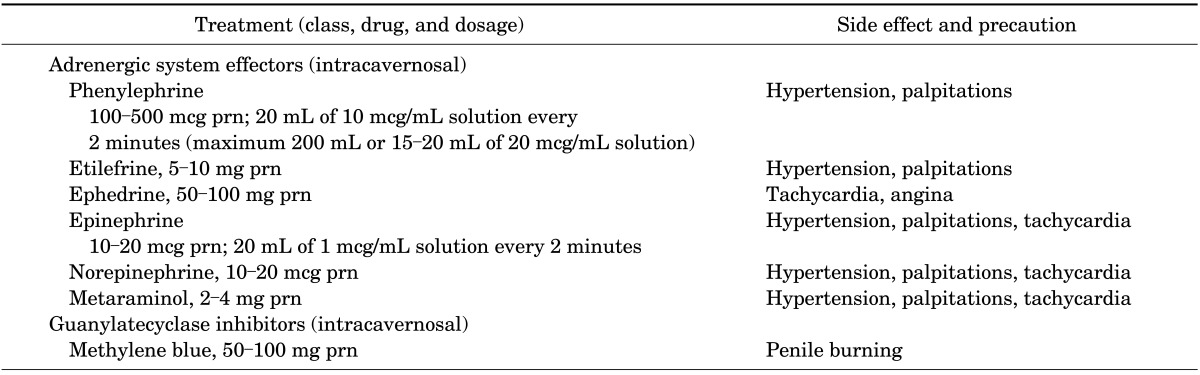
Concomitant management of verified underlying causes (e.g., analgesia, hydration, oxygenation, alkalinization, and even exchange transfusion for sickle cell disease in association with priapism) has generally been offered. However, such medical management should not replace second-line intracavernous procedures for treatment of major ischemic priapism [1,11,21].
First-line and second-line treatments are repeated as necessary according to urologist judgment. Although it is not clear that an unusual time gap is required to be met before proceeding with third-line intervention (e.g., penile shunt surgery), consensus recommendations have proposed a course of first-line and second-line treatments for at least 1 hour before proceeding to the next line of management. In some cases, after first-line and second-line treatments, the penis persists to feel semirigid owing to residual edema of the intracorporal or extracorporal tissues. Determining whether a priapism has been adequately treated may be difficult. Clinical signs suggesting failure of first-line and second-line treatments and persistence of the disorder at reassessment (e.g., corporal rigidity by exam, acidosis, and anoxia by cavernous blood gas testing, absence of cavernosal artery inflow by penile CDU, or elevated intracorporal pressures by pressure monitoring) may assist in decision making by clinicians [1,4,11].
4) Third-line treatment: surgical shunts
Third-line treatment is a surgical intervention typically in the form of penile shunt surgery. As with any surgery, consent and documentation are required, although in view of considered risks and benefits, such procedures are particularly necessary in this clinical setting. The function of the surgical shunt is to make an iatrogenic fistula in order to establish an outflow channel from the corpora cavernosa bypassing the pathological veno-occlusion [1,4].
Surgical shunts are divided into four anatomical subcategories. A description of the procedures is provided in Table 2: 1) percutaneous distal (corporoglanular) shunts (e.g., Winter [22], Ebbehoj [23], Brant et al. [24]); 2) open distal (corporoglanular) shunts (e.g., Hanafy et al. [25], Burnett and Pierorazio [26]); 3) open proximal (corporospongiosal) shunts (e.g., Quackels [27], Sacher et al. [28]); 4) vein anastomosis/shunts (e.g., saphenous vein, Grayhack et al. [29]); and superficial or deep dorsal vein shunt (e.g., Barry [30]).
TABLE 2.
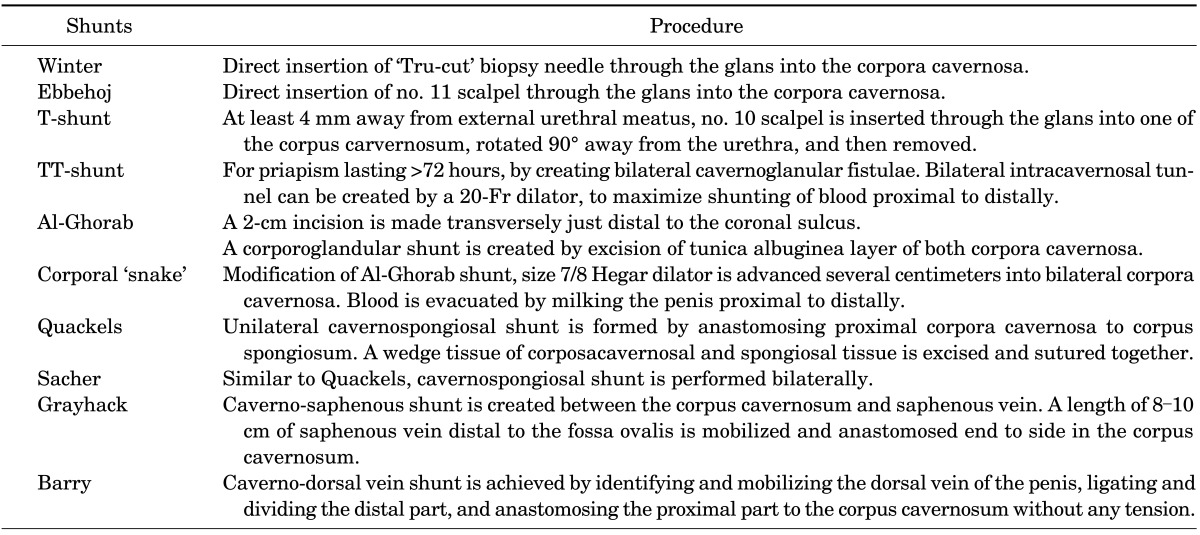
The success rate for distal shunts is 66% to 77%, whereas the response rates for proximal shunts and venous anastomosis are 50% and 25%, respectively. Distal shunts are less traumatic, easier to perform, and associated with fewer complications, e.g., urethral fistulae and purulent cavernositis [11]. If distal shunts are unsuccessful, proximal shunts can be considered [1].
After the shunt procedure, manual application of intermittent compression on the penis is important to maintain patency of the fistula. Serious penile edema may make the penis appear semirigid and may create uncertainly regarding the response to management. Corpora cavernosal blood gas analysis and repeat penile CDU may be helpful in determining treatment response in these circumstances. Intracavernosal pressure of <40 mmHg can provide further reassurance [15]. Failed correction of a priapism by such clinical signs at the time of initial operation usually prompts the immediate performance of an alternative shunt procedure. Additional shunt attempts may also be required in the event of recurrence of priapism verified during postoperative assessments, which should be serially performed for at least 24 hours after operation [1]. An added maneuver proposed by some experts to enhance the effect of distal shunt procedures is application of a small (baby) blood pressure cuff to the penile shaft that can be repeatedly inflated for maintenance of shunt patency and penile detumescence.
The extent of erectile function conservation after penile shunt surgery is controversial, and in settings of major ischemic priapism of a prolonged duration (e.g., >36 hours), this intervention may only serve to restrict pain sensations without reversing metabolically generated pathologic sequelae within the penis [1,4].
5) Penile prosthesis implantation
In all, 90% of patients with priapism lasting for >24 hours have erectile dysfunction. Dense fibrosis of the corpora cavernosa develops during extended priapism, which complicates the later insertion of penile prostheses [6]. Early implantation before the development of dense fibrosis might provide more satisfactory results. In addition, placement of a malleable prosthesis acts to prevent fibrosis and scarring of the corpora cavernosa, thus sustaining penile length [31,32]. Early implantation of a penile prosthesis also permits early reinstatement of sexual activity [6,31]. An additional potential benefit in proceeding early with this intervention is avoidance of surgical difficulty and complication risks (e.g., urethral injury, tunical erosions, infection) if surgery is performed some time later after the development of long-term corporal fibrosis [33]. There are no clear indications for implanting a penile prosthesis in priapism. Once the tissues have settled, the patient can be considered for implantation of an inflatable penile prosthesis. In the assessment of each case, decisions must be made on the basis of the surgeon's experience and patient preference [6,31].
2. Stuttering (intermittent or recurrent) priapism
Management of stuttering priapism should also be vigorous with attention to its ischemic risk to the penis and its inclination to evolve into a major priapism episode. Several therapeutic strategies have been advocated for control of this disorder, with the intent to administer either reactive treatment upon recurrence (e.g., on-demand self-injection of sympathomimetic agents) or to avert its recurrence altogether (e.g., systemically administered hormonal agents, digoxin, terbutaline, baclofen, phosphodiesterase 5 [PDE5] inhibitors, or penile prosthesis surgery) [1,11]. These agents are summarized in Table 3. Most widely used are hormonal treatments (e.g., androgen receptor antagonists, gonadotropin-releasing hormone agonists, and 5-alpha reductase inhibitors); limitations are associated with their antiandrogenic effects on sexual function and physical composition. In particular, hormonal agents should not be used in patients who have not reached full sexual maturation and adult size owing to the risks of these complications. Because the success of these strategies is unpredictable and largely based on case reports and case series, evidence-based recommendations for any particular treatment are currently limited [7]. Interest in a preventive, molecular-mechanism-based therapeutic strategy entailing long-term, low-dose PDE5 inhibitor therapy has increased, although further investigations will be necessary to define the role of this treatment [7,34].
TABLE 3.
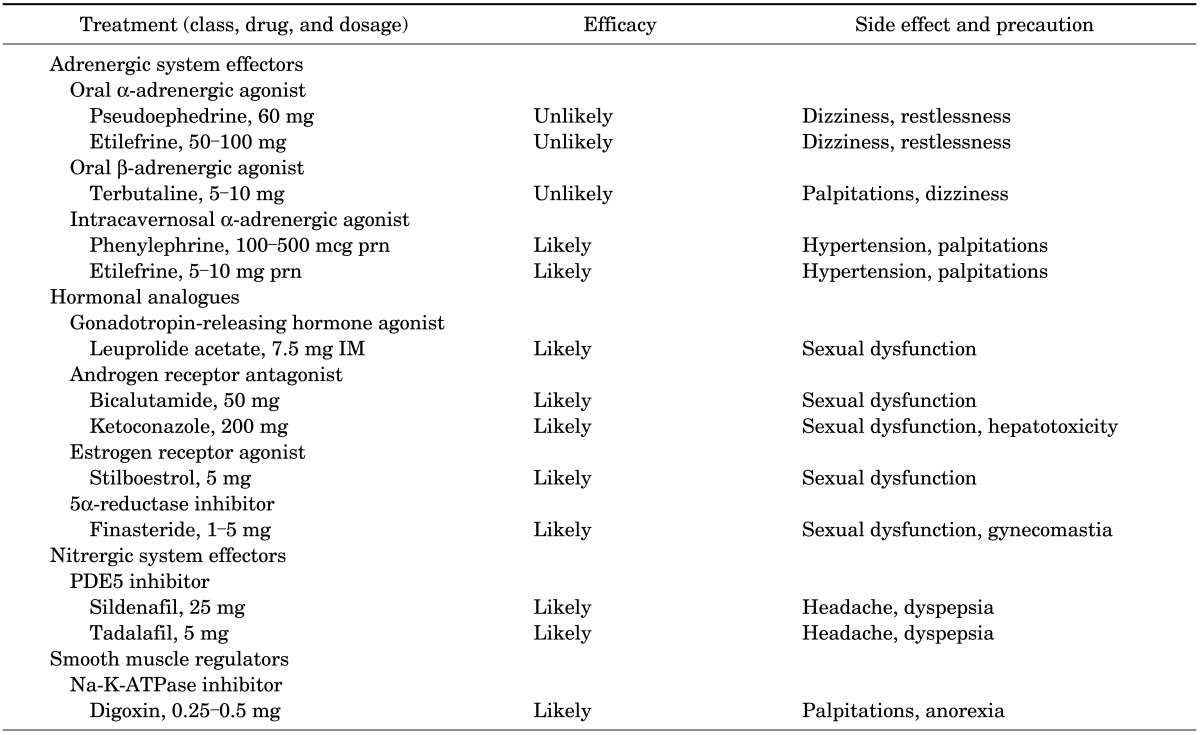
IM, intramuscularly; PDE5, phosphodiesterase 5.
Self-injection of intracavernosal sympathomimetics can result in termination of a major acute ischemic priapism episode and thus prevent hospitalization. This is not the recommended single treatment for stuttering priapism, however, because it only treats acute priapism events rather than preventing recurrence [11]. Nevertheless, it is an option for priapism in patients who cannot tolerate or whose symptoms are refractory to systemic preventative managements [1]. Ralph et al. [35] have also fabricated an implanted sympathomimetic delivery system specifically for stuttering priapism. Surgical options can be offered in men with stuttering priapism refractory to medical therapy, including penile prosthesis implantation [17,36].
3. Nonischemic (arterial, high-flow) priapism
Nonischemic priapism does not characteristically exert ischemic damage to the penis, and delaying interventions is not perceived to impart significant consequences. Therefore, the standard primary intervention is observation (clinical surveillance). In addition, reports have proposed that as many as two-thirds of cases show spontaneous resolution [4,11,37]. However, some nonischemic priapisms develop erectile dysfunction [11]. This may be secondary to nonphysiological, continuously elevated intracavernosal PaO2 [38,39].
Angiography with super-selective embolization is the gold-standard treatment for nonischemic priapism. The aim of this treatment is to disrupt the aberrant arteriovenous connection. Alternatively, occlusion of the cavernous artery is performed [40]. However, these procedures can be complicated by gluteal ischemia, penile gangrene, or purulent cavernositis. In addition, the recurrence rate after a single embolization is 30% to 40% with a concomitant hazard of erectile dysfunction of 5% and 39%, for absorbable and nonabsorbable materials, respectively [1,40]. Erectile dysfunction can be transient if nonabsorbable materials, e.g., gelatin foam or autologous clots, are used. In this situation, vessel recanalization will cause preservation of erectile function [41,42]. Combination of super-selective embolization and CDU-guided compression has currently been reported to achieve higher rates of success [40].
Open surgery is associated with a critical erectile dysfunction rate of up to 50%. Consequently, open surgery is not shown as a first-line treatment option [11,13]. Thus, open surgery is used for cases that are refractory to all other management options.
CONCLUSIONS
A fundamental aim of the management of priapism is to reduce the extent of physical injury to the penis and erectile dysfunction as well as combined psychosocial complications as much as possible. To this end, appropriate management at a minimum entails prompt recognition of the disorder and timely initiation of clinical interventions that relieve recognized risks such as penile ischemia and anoxia. With further achievement of scientific progress in the field, management aims should turn to application of preventive or corrective procedures for the disease that are consistent with maximal preservation of sexual health.
Footnotes
The authors have nothing to disclose.
References
- 1.Broderick GA, Kadioglu A, Bivalacqua TJ, Ghanem H, Nehra A, Shamloul R. Priapism: pathogenesis, epidemiology, and management. J Sex Med. 2010;7(1 Pt 2):476–500. doi: 10.1111/j.1743-6109.2009.01625.x. [DOI] [PubMed] [Google Scholar]
- 2.Canguven O, Cetinel C, Horuz R, Tarhan F, Hamarat B, Goktas C. Transient distal penile corporoglanular shunt as an adjunct to aspiration and irrigation procedures in the treatment of early ischemic priapism. Korean J Urol. 2013;54:394–398. doi: 10.4111/kju.2013.54.6.394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim JH, Choi HJ, Ryu KH, Jeong YS, Choi YS, Lee SW. High flow priapism developed after treatment of low flow priapism. Korean J Urol. 2005;46:876–878. [Google Scholar]
- 4.Burnett AL, Bivalacqua TJ. Priapism: new concepts in medical and surgical management. Urol Clin North Am. 2011;38:185–194. doi: 10.1016/j.ucl.2011.02.005. [DOI] [PubMed] [Google Scholar]
- 5.Burnett AL, Bivalacqua TJ. Priapism: current principles and practice. Urol Clin North Am. 2007;34:631–642. doi: 10.1016/j.ucl.2007.08.006. [DOI] [PubMed] [Google Scholar]
- 6.Ralph DJ, Garaffa G, Muneer A, Freeman A, Rees R, Christopher AN, et al. The immediate insertion of a penile prosthesis for acute ischaemic priapism. Eur Urol. 2009;56:1033–1038. doi: 10.1016/j.eururo.2008.09.044. [DOI] [PubMed] [Google Scholar]
- 7.Chow K, Payne S. The pharmacological management of intermittent priapismic states. BJU Int. 2008;102:1515–1521. doi: 10.1111/j.1464-410X.2008.07951.x. [DOI] [PubMed] [Google Scholar]
- 8.Kato GJ. Priapism in sickle-cell disease: a hematologist's perspective. J Sex Med. 2012;9:70–78. doi: 10.1111/j.1743-6109.2011.02287.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Keoghane SR, Sullivan ME, Miller MA. The aetiology, pathogenesis and management of priapism. BJU Int. 2002;90:149–154. doi: 10.1046/j.1464-410x.2002.02825.x. [DOI] [PubMed] [Google Scholar]
- 10.Broderick GA. Priapism. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh urology. 10th ed. Philadelphia: Saunders; 2011. pp. 749–769. [Google Scholar]
- 11.Montague DK, Jarow J, Broderick GA, Dmochowski RR, Heaton JP, Lue TF, et al. American Urological Association guideline on the management of priapism. J Urol. 2003;170(4 Pt 1):1318–1324. doi: 10.1097/01.ju.0000087608.07371.ca. [DOI] [PubMed] [Google Scholar]
- 12.LeRoy TJ, Broderick GA. Doppler blood flow analysis of erectile function: who, when, and how. Urol Clin North Am. 2011;38:147–154. doi: 10.1016/j.ucl.2011.03.003. [DOI] [PubMed] [Google Scholar]
- 13.Ciampalini S, Savoca G, Buttazzi L, Gattuccio I, Mucelli FP, Bertolotto M, et al. High-flow priapism: treatment and long-term follow-up. Urology. 2002;59:110–113. doi: 10.1016/s0090-4295(01)01464-9. [DOI] [PubMed] [Google Scholar]
- 14.Ralph DJ, Borley NC, Allen C, Kirkham A, Freeman A, Minhas S, et al. The use of high-resolution magnetic resonance imaging in the management of patients presenting with priapism. BJU Int. 2010;106:1714–1718. doi: 10.1111/j.1464-410X.2010.09368.x. [DOI] [PubMed] [Google Scholar]
- 15.Huang YC, Harraz AM, Shindel AW, Lue TF. Evaluation and management of priapism: 2009 update. Nat Rev Urol. 2009;6:262–271. doi: 10.1038/nrurol.2009.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lowe FC, Jarow JP. Placebo-controlled study of oral terbutaline and pseudoephedrine in management of prostaglandin E1-induced prolonged erections. Urology. 1993;42:51–53. doi: 10.1016/0090-4295(93)90338-b. [DOI] [PubMed] [Google Scholar]
- 17.Burnett AL. Surgical management of ischemic priapism. J Sex Med. 2012;9:114–120. doi: 10.1111/j.1743-6109.2011.02446.x. [DOI] [PubMed] [Google Scholar]
- 18.Kulmala RV, Tamella TL. Effects of priapism lasting 24 hours or longer caused by intracavernosal injection of vasoactive drugs. Int J Impot Res. 1995;7:131–136. [PubMed] [Google Scholar]
- 19.Muneer A, Minhas S, Freeman A, Kumar P, Ralph DJ. Investigating the effects of high-dose phenylephrine in the management of prolonged ischaemic priapism. J Sex Med. 2008;5:2152–2159. doi: 10.1111/j.1743-6109.2008.00862.x. [DOI] [PubMed] [Google Scholar]
- 20.Munarriz R, Wen CC, McAuley I, Goldstein I, Traish A, Kim N. Management of ischemic priapism with high-dose intracavernosal phenylephrine: from bench to bedside. J Sex Med. 2006;3:918–922. doi: 10.1111/j.1743-6109.2005.00140.x. [DOI] [PubMed] [Google Scholar]
- 21.Morrison BF, Burnett AL. Priapism in hematological and coagulative disorders: an update. Nat Rev Urol. 2011;8:223–230. doi: 10.1038/nrurol.2011.28. [DOI] [PubMed] [Google Scholar]
- 22.Winter CC. Cure of idiopathic priapism: new procedure for creating fistula between glans penis and corpora cavernosa. Urology. 1976;8:389–391. doi: 10.1016/0090-4295(76)90498-2. [DOI] [PubMed] [Google Scholar]
- 23.Ebbehoj J. A new operation for priapism. Scand J Plast Reconstr Surg. 1974;8:241–242. doi: 10.3109/02844317409084400. [DOI] [PubMed] [Google Scholar]
- 24.Brant WO, Garcia MM, Bella AJ, Chi T, Lue TF. T-shaped shunt and intracavernous tunneling for prolonged ischemic priapism. J Urol. 2009;181:1699–1705. doi: 10.1016/j.juro.2008.12.021. [DOI] [PubMed] [Google Scholar]
- 25.Hanafy HM, Saad SM, El-Rifaie M, Al-Ghorab MM. Early arabian medicine: contribution to urology. Urology. 1976;8:63–67. doi: 10.1016/0090-4295(76)90059-5. [DOI] [PubMed] [Google Scholar]
- 26.Burnett AL, Pierorazio PM. Corporal "snake" maneuver: corporoglanular shunt surgical modification for ischemic priapism. J Sex Med. 2009;6:1171–1176. doi: 10.1111/j.1743-6109.2008.01176.x. [DOI] [PubMed] [Google Scholar]
- 27.Quackels R. Treatment of a case of priapism by cavernospongious anastomosis. Acta Urol Belg. 1964;32:5–13. [PubMed] [Google Scholar]
- 28.Sacher EC, Sayegh E, Frensilli F, Crum P, Akers R. Cavernospongiosum shunt in the treatment of priapism. J Urol. 1972;108:97–100. doi: 10.1016/s0022-5347(17)60651-7. [DOI] [PubMed] [Google Scholar]
- 29.Grayhack JT, McCullough W, O'conor VJ, Jr, Trippel O. Venous bypass to control priapism. Invest Urol. 1964;1:509–513. [PubMed] [Google Scholar]
- 30.Barry JM. Priapism: treatment with corpus cavernosum to dorsal vein of penis shunts. J Urol. 1976;116:754–756. doi: 10.1016/s0022-5347(17)58998-3. [DOI] [PubMed] [Google Scholar]
- 31.Sedigh O, Rolle L, Negro CL, Ceruti C, Timpano M, Galletto E, et al. Early insertion of inflatable prosthesis for intractable ischemic priapism: our experience and review of the literature. Int J Impot Res. 2011;23:158–164. doi: 10.1038/ijir.2011.23. [DOI] [PubMed] [Google Scholar]
- 32.Deveci S, Martin D, Parker M, Mulhall JP. Penile length alterations following penile prosthesis surgery. Eur Urol. 2007;51:1128–1131. doi: 10.1016/j.eururo.2006.10.026. [DOI] [PubMed] [Google Scholar]
- 33.Salem EA, El Aasser O. Management of ischemic priapism by penile prosthesis insertion: prevention of distal erosion. J Urol. 2010;183:2300–2303. doi: 10.1016/j.juro.2010.02.014. [DOI] [PubMed] [Google Scholar]
- 34.Burnett AL. Against: no surgery for stuttering priapism. J Urol. 2009;181:450–451. doi: 10.1016/j.juro.2008.11.075. [DOI] [PubMed] [Google Scholar]
- 35.Ralph DJ, Pescatori ES, Brindley GS, Pryor JP. Intracavernosal phenylephrine for recurrent priapism: self-administration by drug delivery implant. J Urol. 2001;165:1632. [PubMed] [Google Scholar]
- 36.Carson CC. For: surgery for stuttering priapism. J Urol. 2009;181:449–450. doi: 10.1016/j.juro.2008.11.052. [DOI] [PubMed] [Google Scholar]
- 37.Pryor J, Akkus E, Alter G, Jordan G, Lebret T, Levine L, et al. Priapism. J Sex Med. 2004;1:116–120. doi: 10.1111/j.1743-6109.2004.10117.x. [DOI] [PubMed] [Google Scholar]
- 38.Bertolotto M, Zappetti R, Pizzolato R, Liguori G. Color Doppler appearance of penile cavernosal-spongiosal communications in patients with high-flow priapism. Acta Radiol. 2008;49:710–714. doi: 10.1080/02841850802027026. [DOI] [PubMed] [Google Scholar]
- 39.Marotte JB, Brooks JD, Sze D, Kennedy WA., 2nd Juvenile posttraumatic high-flow priapism: current management dilemmas. J Pediatr Surg. 2005;40:E25–E28. doi: 10.1016/j.jpedsurg.2005.01.023. [DOI] [PubMed] [Google Scholar]
- 40.Cakan M, Altu Gcaron U, Aldemir M. Is the combination of superselective transcatheter autologous clot embolization and duplex sonography-guided compression therapy useful treatment option for the patients with high-flow priapism? Int J Impot Res. 2006;18:141–145. doi: 10.1038/sj.ijir.3901373. [DOI] [PubMed] [Google Scholar]
- 41.Numan F, Cantasdemir M, Ozbayrak M, Sanli O, Kadioglu A, Hasanefendioglu A, et al. Posttraumatic nonischemic priapism treated with autologous blood clot embolization. J Sex Med. 2008;5:173–179. doi: 10.1111/j.1743-6109.2007.00560.x. [DOI] [PubMed] [Google Scholar]
- 42.Takao T, Osuga K, Tsujimura A, Matsumiya K, Nonomura N, Okuyama A. Successful superselective arterial embolization for post-traumatic high-flow priapism. Int J Urol. 2007;14:254–256. doi: 10.1111/j.1442-2042.2007.01574.x. [DOI] [PubMed] [Google Scholar]