

Abstract
Azygos vein aneurysm is very rare and most cases are detected incidentally. We report a safe resection of azygos vein aneurysm by video-assisted thoracoscopic surgery (VATS) under preoperative evaluation of thrombus by multidetector computed tomography (MDCT). A 60-year old woman presented to our department due to a mediastinal mass revealed by enhanced CT. A dynamic enhanced-CT scan showed a dilated azygos vein with great enhancement in the early phase. Under the diagnosis of azygos vein aneurysm, we analysed the aneurysm by MDCT and confirmed that there was no thrombus within the aneurysm. The resection of the aneurysm by VATS was performed safely. She was discharged 4 days after surgery.
Keywords: Azygos vein aneurysm, Multidetector computed tomography, Video-assisted thoracic surgery
CASE REPORT
A 60-year old female patient was admitted to our hospital for evaluation of a mediastinal mass. The mass was revealed by enhanced chest computed tomography (CT) for screening of malignancies. Because enhanced CT showed a dilated azygos vein, which was a well-circumscribed mass 25 mm in diameter (Fig. 1), we diagnosed it as an azygos vein aneurysm. The results of blood tests, including fibrin D-dimer measurement, were within the normal limits. In order to preoperatively evaluate the existence of a thrombus within the azygos vein aneurysm, a dynamic contrast-enhanced multidetector CT (MDCT) was performed. The MDCT showed the retrograde flow of the contrast agent from the superior vena cava (SVC) to the azygos vein aneurysm during the early phase. The filling defect was apparently detected, but washout of the contrast medium was shown during the equilibrium phase. As a result, we judged the azygos vein aneurysm as without thrombus.
Figure 1:
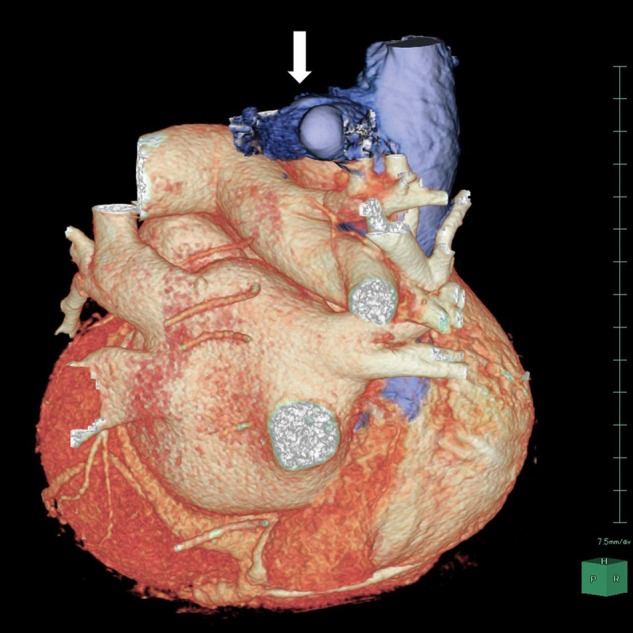
Three-dimensional construction revealing a 25 mm-sized posterior mediastinal mass which shows dilated azygos vein (arrow).
Surgical resection was performed by video-assisted thoracic surgery (VATS). Under general anaesthesia with one-lung ventilation, a thoracoscopic trocar was placed at the seventh intercostal space on the midaxillary line, a 20 mm-long incision was made at the sixth intercostal space on the angulus inferior scapulae and a 40 mm-long incision was made at the fourth intercostal space on the anterior axillary line. At first, in order to prevent pulmonary embolism caused by microthrombus, we clamped the central site of the aneurysm attached to the SVC using a multifire Endo TA 30 stapler. Then, we resected the distal site of the azygos vein aneurysm at the level of the junction to the highest intercostal vein, using an Endo GIA ultra universal tristapler camel 45 mm. There were no postoperative complications, and the patient was discharged 4 days after surgery. The diagnosis of the azygos vein aneurysm was confirmed by pathological examination. There were no abnormal findings 3 months after the operation.
DISCUSSION
An azygos vein aneurysm is very rare, and it is often detected as a mediastinal tumour on chest CT without symptoms. Concerning the aetiology, an azygos vein aneurysm is considered to occur secondarily due to portal hypertension, inferior vena cava occlusion, heart failure or trauma. However, some cases have been regarded as idiopathic lesions [1]. This case was regarded as an idiopathic lesion because there were no complications, as described above, and there was no history of injury.
The treatment strategy for azygos vein aneurysm is still unclear because appropriate management of an asymptomatic aneurysm has not been established. To our knowledge, there has been no report of a case of ruptured azygos vein aneurysm. However, it has been reported that the forming of thrombus in an aneurysm caused severe pulmonary embolism [2]. A thrombus forming suddenly during 6 years has also been reported [3]. On the other hand, it is difficult to resect the azygos vein aneurysm by small incision operation when it is enlarged or thrombosed. Considering these circumstances, earlier treatment of surgical resection might be needed even if there is no thrombus within the azygos vein aneurysm.
The efficacy of surgical resection by VATS has been reported [4]. In addition, surgical resection by VATS is considered to be safe when the azygos vein aneurysm has no thrombus. Therefore, it is important to confirm no thrombus preoperatively. A previous study has documented the ability of MDCT to detect and visualize coronary atherosclerotic plaque [5]. In this case, we applied MDCT for evaluation of thrombus and judged there was no thrombus. In fact, we confirmed no thrombus inside the specimen of aneurysm. MDCT might be useful for preoperative evaluation of thrombus.
Conflict of interest: none declared.
REFERENCES
- 1.Icard P, Fares E, Regnard JF, Levasseur P. Thrombosis of an idiopathic saccular azygos aneurysm. Eur J Cardiothorac Surg. 1999;15:870–2. doi: 10.1016/s1010-7940(99)00127-x. [DOI] [PubMed] [Google Scholar]
- 2.Nakamura Y, Nakano K, Nakatani H, Fukuda T, Honda K, Homma N. Surgical exclusion of a thrombosed azygos vein aneurysm causing pulmonary embolism. J Thorac Cardiovasc Surg. 2007;133:834–5. doi: 10.1016/j.jtcvs.2006.11.012. [DOI] [PubMed] [Google Scholar]
- 3.Kurihara C, Kiyoshima M, Asato Y, Suzuki H, Kitahara M, Satou M, et al. Resection of an azygos vein aneurysm that formed a thrombus during a 6-year follow-up period. Ann Thorac Surg. 2012;94:1008–10. doi: 10.1016/j.athoracsur.2012.01.086. [DOI] [PubMed] [Google Scholar]
- 4.Person TD, Komanapalli CB, Chaugle H, Schipper PH, Sukumar MS. Thoracoscopic approach to the resection of an azygos vein aneurysm. J Thorac Cardiovasc Surg. 2005;130:230–1. doi: 10.1016/j.jtcvs.2004.11.054. [DOI] [PubMed] [Google Scholar]
- 5.Achenbach S, Moselewski F, Ropers D, Ferencik M, Hoffmann U, MacNeill B, et al. Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multidetector spiral computed tomography: a segment-based comparison with intravascular ultrasound. Circulation. 2004;109:14–7. doi: 10.1161/01.CIR.0000111517.69230.0F. [DOI] [PubMed] [Google Scholar]