

Abstract
Purpose
To assess the results of arthroscopic adhesiolysis for arthrofibrosis of the knee and to investigate possible prognostic factors.
Materials and Methods
Among the patients who developed arthrofibrosis after knee joint surgery, 68 patients who underwent arthroscopic adhesiolysis and were available for at least one-year follow-up were evaluated with regard to the Lysholm knee score, International Knee Documentation Committee (IKDC) subjective knee score, patient satisfaction, and range of motion (ROM) of the knee. The influence of possible prognostic factors including the cause of arthrofibrosis, duration of disease, and age of the patient on the postoperative ROM was analyzed.
Results
Sixty-one patients (89.7%) obtained an average increase of 48.6° in ROM; however, the remaining seven patients (10.3%) did not show any increase at the final follow-up. The Lysholm knee score and IKDC subjective knee score increased significantly at the final follow-up. Patient satisfaction was high or very high in 89.7% of the patients at the final follow-up. There was no association between the cause of arthrofibrosis and the increase in postoperative ROM. The duration of disease was significantly related to the postoperative recovery of ROM. Age had no significant influence on the postoperative recovery of ROM.
Conclusions
We believe that arthroscopic adhesiolysis is effective for the treatment of intraarticular arthrofibrosis. In particular, the duration of the disease had significant influence on the postoperative outcome.
Keywords: Knee, Arthrofibrosis, Range of motion, Arthroscopic adhesiolysis
Introduction
Range of motion (ROM) loss is one of the most serious sequelae of fractures and soft tissue injuries around the knee and knee surgery. Pyogenic infection, prolonged postoperative immobility of the knee, and improper rehabilitation can result in an ROM deficit, but soft tissue damage and adhesions around the knee after a distal femoral fracture are responsible in most cases1,2). Open surgery (quadricepsplasty) was undertaken frequently for arthrofibrosis of intraarticular or extraarticular origin in the past; however, it is a high-risk procedure that requires long rehabilitation and postoperative immobilization. Recently, the advent of arthroscopic ligament reconstruction techniques and accelerated rehabilitation programs has contributed to the reduced incidence of postoperative knee stiffness. Moreover, gentle manipulations under anesthesia and arthroscopic adhesiolysis have become accepted as viable treatment modalities for arthrofibrosis of the knee3-8). Arthroscopy allows the visualization of intraarticular structures without the need for a joint incision during adhesiolysis, facilitates early rehabilitation, and decreases the risk of surgery and postoperative complications. Thus, arthroscopic adhesiolysis can be an effective treatment method for patients with a ROM deficit caused by intraarticular adhesions after knee surgery.
The purpose of the current study was to investigate the relationship between the outcomes of arthroscopic adhesiolysis and the possible prognostic factors including the cause and duration of the disease and age in patients with arthrofibrosis of the knee.
Materials and Methods
Of the 76 patients who underwent arthroscopic adhesiolysis for knee stiffness between June 2003 and June 2009, 68 patients with arthrofibrosis of an intraarticular origin were included in this study. The study was conducted with Institutional Review Board approval and the minimum follow-up period was one year. The indications for surgery were types 3 and 4 arthrofibrosis that are characterized by the presence of a loss of flexion and patella infera, according to the classification proposed by Shelbourne et al.9).
Anteromedial and anterolateral portals that are commonly used for arthroscopic knee surgery do not allow accurate visualization in cases of arthrofibrosis due to intraarticular adhesions, and may cause meniscal damage during the insertion of an obturator. Accordingly, we used a superolateral portal as the initial viewing portal for arthroscopic adhesiolysis in our patients. An approximately 5-mm incision was made at the junction of the superior border and the lateral border of the patella. A Wissinger rod was inserted into the suprapatellar pouch and advanced superiorly, inferiorly, and medially to release the intraarticular adhesions. Subsequently, an anterolateral portal was established for the insertion of an arthroscope, and the released adhesions in the suprapatellar pouch and other intraarticular adhesions in the lateral gutter were debrided using an arthro-care and a motorized shaver introduced through the superolateral portal (Fig. 1). Then, an anteromedial portal was created, through which an arthro-care and a motorized shaver were inserted for debridement of the remaining adhesions in the medial gutter and the medial aspect of the suprapatellar pouch. During the procedure, the remaining adhesive and fibrosis tissues in the intercondylar notch of the femur and infrapatellar fat pad were removed. The principle of the lysis was to remove the adhesive fibrosis tissues in the suprapatellar pouch, intercondylar notch of the femur, and infrapatellar fat pad, and around the patella as much as possible to facilitate normal patellar tracking. When the extent of lysis was considered sufficient, gentle manipulations of the knee were performed with the goal of obtaining ≥140° of flexion until resistance was felt by the surgeon to prevent further complications, such as a fracture. Utmost care was taken to achieve normal ROM as much as possible by repeating extension and flexion motions.
Fig. 1.

(A) Severe adhesion around the patellar fracture site. (B) The adhesion is debrided using a motorized shaver.
From the first postoperative day, if the pain decreased, joint exercises using a continuous passive motion device were started taking effort to obtain full ROM as much as possible. Patients were instructed to perform passive/active flexion/extension exercises on the bed when the device was not in use. Quadriceps femoris strengthening exercises and active/passive joint exercises were continued for a minimum of three consecutive months.
Follow-up examinations were performed at 2 weeks, 3 months, 6 months, and 12 months after surgery, and every six months thereafter. The mean follow-up period was 17.8 months (range, 13 to 57 months). The Lysholm knee score, International Knee Documentation Committee (IKDC) subjective knee score, and patient satisfaction were assessed. The influence of possible prognostic factors including the cause of the arthrofibosis, duration of disease, and age on the postoperative ROM was analyzed on an outpatient basis during the follow-up period. The ROM was measured using a goniometer in 1° increments: one arm of the goniometer was placed along the greater trochanter and the lateral epicondyle of the femur and the other arm was aligned with the fibular head and the lateral malleolus of the fibula.
Statistical analysis was done using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). The Lysholm knee score, IKDC subjective knee score, and ROM were assessed using paired sample t-tests. The relationship between the prognostic factors and the postoperative ROM was assessed using independent sample t-tests. A p<0.05 was considered statistically significant.
Results
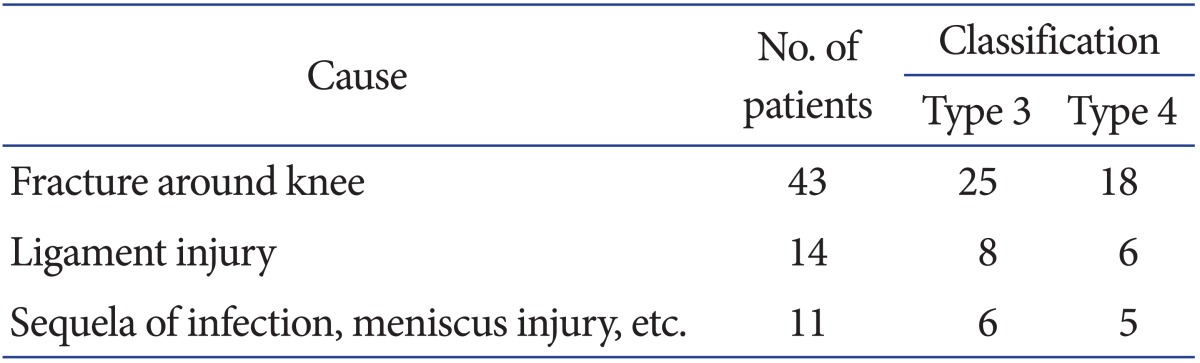
The study population consisted of 57 males and 11 females. Their mean age at the time of surgery was 39.3 years (range, 17 to 64 years), and the mean value for each gender group was also 39.3 years for males (range, 17 to 61 years) and females (range, 23 to 64 years). The most common cause of arthrofibrosis was a fracture around the knee in 43 patients (type II in 25 and type IV in 18). Other causes included a ligament injury in 14 patients (type III in 8 and type IV in 6) and an infection or a meniscus injury in 11 patients (type III in 6 and type IV in 5) (Table 1).
Table 1.
Causes of Arthrofibrosis of the Knee
The mean degree of preoperative flexion contracture was 16.0° (range, 11° to 60°) and the mean range of further flexion was 77.6° (range, 26° to 108°). At two weeks after surgery, the mean flexion contracture was 10.5° (range, 0° to 35°) and the mean range of further flexion was 102.3° (range, 43° to 135°). At the last follow-up, the mean flexion contracture was 8.2° (range, 0° to 20°) and the mean range of further flexion was 118.4° (range, 60° to 135°) (Table 2). Statistical significance was found in the mean increase in ROM (48.6°) from the preoperative value of 67.6° to the last follow-up value of 116.2° (p=0.000) (Table 3). Notable improvement in the ROM was observed regardless of the cause of the arthrofibrosis (fracture around the knee, ligament injury, and knee infection, meniscus injury, etc.) and the mean ROM increase was not significantly different among the three groups when they were divided according to the cause (Table 4).
Table 2.
Degrees of Flexion Contracture and Flexion
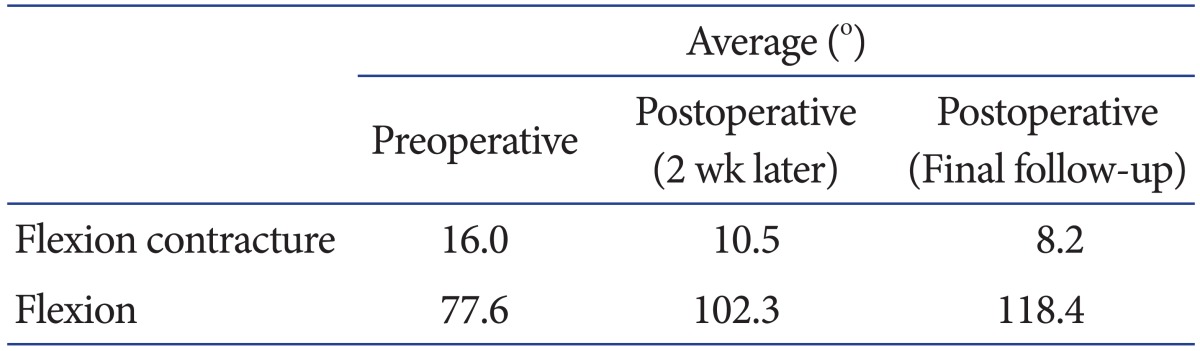
Table 3.
Summary of Range of Motion and Knee Scores
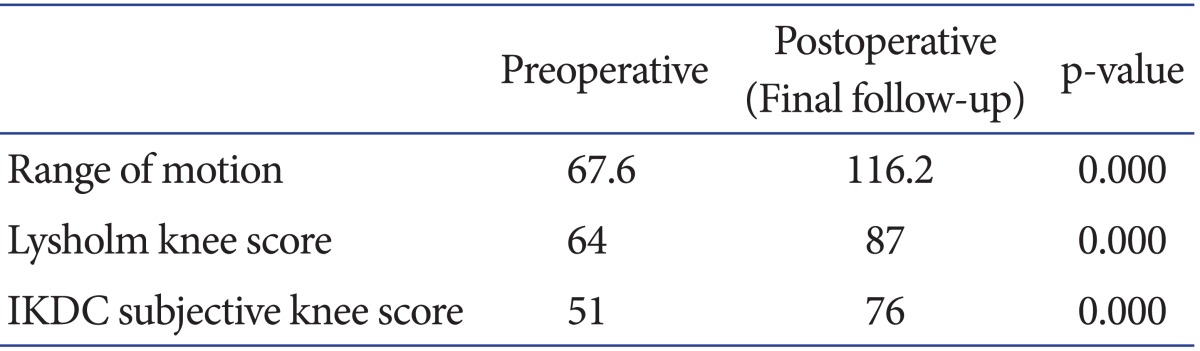
IKDC: International Knee Documentation Committee.
Table 4.
Summary of Preoperative Factors and Postoperative Outcomes

There were significant increases in the mean Lysholm knee score from 64 points (range, 30 to 86 points) preoperatively to 87 points (range, 39 to 100 points) at the last follow-up (p=0.000) and in the mean IKDC subjective knee score from 51 points (range, 26 to 63.2 points) preoperatively to 76 points (range, 40.2 to 93.1 points) at the last follow-up (p=0.000) (Table 3). The level of patient satisfaction at the last follow-up was high or very high in 89.7% of the patients.
The mean increase in ROM at the last follow-up was higher in patients with <7 months of duration of disease (46 patients, 58.4° [range, 35° to 105°]) than in patients with ≥7 months of duration of disease (22 patients, 41.7° [range, 20° to 85°], p=0.026).
The mean increase in ROM at the last follow-up was 45.9° (range, 35° to 105°) in 31 patients who were ≤40 years of age and 52.7° (range, 20° to 100°) in 37 patients who were >40 years of age, indicating that there was no significant relationship between age and the postoperative ROM (p=0.873).
There was no increase of ROM in 7 patients (10.3%) at the last follow-up, and one of these patients (1.5%) exhibited a loss of ROM. No postoperative complication was observed except for one case of wound infection.
Discussion
The currently available treatment options for arthrofibrosis of the knee include knee manipulations4), quadroplasty10-13), and arthroscopic adhesiolysis5,8,9,14-16). In particular, arthroscopic lysis of adhesions has been reported as a minimally invasive procedure with low morbidity and good results5,15,17). Unfortunately, the procedure is technically challenging and can be especially difficult to perform in the initial phase of surgery due to joint space narrowing and adhesions7,8).
On the other hand, the procedure allows for intraoperative visualization of intraarticular lesions; thus, we could intraoperatively examine lesions within the joint, such as anterior/posterior cruciate ligament injuries and meniscal damage, during the procedure in this study. Arthroscopic adhesiolysis is advantageous in that it produces low morbidity, facilitates early joint motion, and requires minimal incisions, although its use is limited to knee stiffness of intraarticular origin and complete healing may be hindered due to remaining extraarticular adhesions. Therefore, adhesiolysis produces limited improvement in cases of knee stiffness combined with surrounding soft tissue damage. Studies have shown that arthroscopic adhesiolysis is more effective for obtaining gain in flexion than extension of the knee14). Our results were in agreement with those reports: knee flexion and flexion contracture increased by 40.8° and 7.8°, respectively, at the last follow-up. Moreover, we believe that parapatellar release, manipulation under anesthesia, and continuous passive joint motion exercises after surgery contributed to the improvement of symptoms even though posterior joint capsule release for flexion contracture was not conducted.
According to a study by Nicoll18), surgical intervention should be considered for arthrofibrosis if ≥70° of knee flexion is necessary for the patient's work or lifestyle or if flexion is not improved to ≥70° with brisement force following several months of physical treatment. In our study, the need for adhesiolysis was determined according to the criteria suggested by Nicoll18), and ≥10° of extension deficit, ≥25° of flexion deficit, restriction of patellar movement, and difficulty with daily living activities were also considered as indications for the operation.
Regarding the timing of adhesiolysis, Cosgarea et al.19) reported that flexion/extension gains and functional outcomes were satisfactory when the procedure was performed within six months after the prior surgery. In our study, the outcomes of adhesiolysis were better when the procedure was performed within seven months after the injury, which is because quadriceps femoris muscle shortening resulting from contracture of the muscle worsens over time after arthrofibrosis.
Postoperative care is crucial for the successful outcome of arthroscopic adhesiolysis. For example, an ROM gain may be lost due to a prolonged period of immobility caused by postoperative pain. In our study, no evidence of improvement in ROM was observed at the last follow-up in seven patients (10.3%), which we attributed to the difficulty of performing proper postoperative care in these patients due to the presence of pain. Noyes et al.20) reported that manipulations under anesthesia after arthroscopic adhesiolysis resulted in improvement in ROM. In our study, passive flexion/extension exercises were performed for the day and continuous passive motion exercises were additionally carried out during the early postoperative rehabilitation period, and these were progressively replaced by active exercises. Considering that the patients who started passive joint exercises immediately after surgery could better maintain their ROM gain, it seems desirable to initiate passive exercises immediately after surgery depending on the patient's tolerance.
The limitations of this study include those inherent in retrospective studies, and the small number of cases involved, especially cases with ligament surgery, knee infection, and meniscal injury. Therefore, we think that the clinical outcomes of arthroscopic adhesiolysis for arthrofibrosis of the knee need to be further investigated in studies involving large study populations.
Conclusions
Arthroscopic adhesiolysis can be effective for the treatment of intraarticular arthrofibrosis of the knee. In particular, the duration of disease was related to the treatment outcomes.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Mira AJ, Markley K, Greer RB., 3rd A critical analysis of quadriceps function after femoral shaft fracture in adults. J Bone Joint Surg Am. 1980;62:61–67. [PubMed] [Google Scholar]
- 2.Ikpeme JO. Quadricepsplasty following femoral shaft fractures. Injury. 1993;24:104–108. doi: 10.1016/0020-1383(93)90199-g. [DOI] [PubMed] [Google Scholar]
- 3.Achalandabaso J, Albillos J. Stiffness of the knee: mixed arthroscopic and subcutaneous technique: results of 67 cases. Arthroscopy. 1993;9:685–690. doi: 10.1016/s0749-8063(05)80507-9. [DOI] [PubMed] [Google Scholar]
- 4.Dodds JA, Keene JS, Graf BK, Lange RH. Results of knee manipulations after anterior cruciate ligament reconstructions. Am J Sports Med. 1991;19:283–287. doi: 10.1177/036354659101900313. [DOI] [PubMed] [Google Scholar]
- 5.Fisher SE, Shelbourne KD. Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med. 1993;21:558–564. doi: 10.1177/036354659302100413. [DOI] [PubMed] [Google Scholar]
- 6.Hughston JC. Complications of anterior cruciate ligament surgery. Orthop Clin North Am. 1985;16:237–240. [PubMed] [Google Scholar]
- 7.Paulos LE, Rosenberg TD, Drawbert J, Manning J, Abbott P. Infrapatellar contracture syndrome: an unrecognized cause of knee stiffness with patella entrapment and patella infera. Am J Sports Med. 1987;15:331–341. doi: 10.1177/036354658701500407. [DOI] [PubMed] [Google Scholar]
- 8.Reider B, Belniak RM, Preiskorn D. Arthroscopic arthrolysis for flexion contracture following intraarticular reconstruction of the anterior cruciate ligament. Arthroscopy. 1996;12:165–173. doi: 10.1016/s0749-8063(96)90006-7. [DOI] [PubMed] [Google Scholar]
- 9.Shelbourne KD, Patel DV, Martini DJ. Classification and management of arthrofibrosis of the knee after anterior cruciate ligament reconstruction. Am J Sports Med. 1996;24:857–862. doi: 10.1177/036354659602400625. [DOI] [PubMed] [Google Scholar]
- 10.Bellemans J, Steenwerckx A, Brabants K, Victor J, Lammens J, Fabry G. The Judet quadricepsplasty: a retrospective analysis of 16 cases. Acta Orthop Belg. 1996;62:79–82. [PubMed] [Google Scholar]
- 11.Ebraheim NA, DeTroye RJ, Saddemi SR. Results of Judet quadricepsplasty. J Orthop Trauma. 1993;7:327–330. doi: 10.1097/00005131-199308000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Hahn SB, Lee WS, Han DY. A modified Thompson quadricepsplasty for the stiff knee. J Bone Joint Surg Br. 2000;82:992–995. doi: 10.1302/0301-620x.82b7.10590. [DOI] [PubMed] [Google Scholar]
- 13.Blanco CE, Leon HO, Guthrie TB. Endoscopic quadricepsplasty: a new surgical technique. Arthroscopy. 2001;17:504–509. doi: 10.1053/jars.2001.24062. [DOI] [PubMed] [Google Scholar]
- 14.Mariani PP, Ferretti A, Conteduca F, Tudisco C. Arthroscopic treatment of flexion deformity after ACL reconstruction. Arthroscopy. 1992;8:517–521. doi: 10.1016/0749-8063(92)90018-7. [DOI] [PubMed] [Google Scholar]
- 15.Sprague NF, 3rd, O'Connor RL, Fox JM. Arthroscopic treatment of postoperative knee fibroarthrosis. Clin Orthop Relat Res. 1982;(166):165–172. [PubMed] [Google Scholar]
- 16.Christie WR, Sprague NF, 3rd, Kim L. Arthroscopic evaluation and treatment of the symptomatic previously operated knee. Arthroscopy. 1988;4:194–198. doi: 10.1016/s0749-8063(88)80026-4. [DOI] [PubMed] [Google Scholar]
- 17.Bae DK, Yim CM, Cho CH. Total knee arthroplasty in ankylosed knee with previous infecton. J Korean Knee Soc. 1997;9:43–49. [Google Scholar]
- 18.Nicoll EA. Quadricepsplasty. J Bone Joint Surg Br. 1963;45:483–490. [PubMed] [Google Scholar]
- 19.Cosgarea AJ, DeHaven KE, Lovelock JE. The surgical treatment of arthrofibrosis of the knee. Am J Sports Med. 1994;22:184–191. doi: 10.1177/036354659402200206. [DOI] [PubMed] [Google Scholar]
- 20.Noyes FR, Mangine RE, Barber SD. The early treatment of motion complications after reconstruction of the anterior cruciate ligament. Clin Orthop Relat Res. 1992;(277):217–228. [PubMed] [Google Scholar]