

Abstract
OBJECTIVE
The Diabetes Control and Complications Trial (DCCT) was designed to test the glucose hypothesis and determine whether the complications of type 1 diabetes (T1DM) could be prevented or delayed. The Epidemiology of Diabetes Interventions and Complications (EDIC) observational follow-up determined the durability of the DCCT effects on the more-advanced stages of diabetes complications including cardiovascular disease (CVD).
RESEARCH DESIGN AND METHODS
The DCCT (1982–1993) was a controlled clinical trial in 1,441 subjects with T1DM comparing intensive therapy (INT), aimed at achieving levels of glycemia as close to the nondiabetic range as safely possible, with conventional therapy (CON), which aimed to maintain safe asymptomatic glucose control. INT utilized three or more daily insulin injections or insulin pump therapy guided by self-monitored glucose. EDIC (1994–present) is an observational study of the DCCT cohort.
RESULTS
The DCCT followed >99% of the cohort for a mean of 6.5 years and demonstrated a 35–76% reduction in the early stages of microvascular disease with INT, with a median HbA1c of 7%, compared with CONV, with a median HbA1c of 9%. The major adverse effect of INT was a threefold increased risk of hypoglycemia, which was not associated with a decline in cognitive function or quality of life. EDIC showed a durable effect of initial assigned therapies despite a loss of the glycemic separation (metabolic memory) and demonstrated that the reduction in early-stage complications during the DCCT translated into substantial reductions in severe complications and CVD.
CONCLUSIONS
DCCT/EDIC has demonstrated the effectiveness of INT in reducing the long-term complications of T1DM and improving the prospects for a healthy life span.
Introduction
The plight of people with type 1 diabetes changed dramatically with the introduction of insulin therapy in 1922 (1). Type 1 diabetes was transformed from a uniformly fatal disease in the preinsulin era, with mortality occurring either acutely from diabetic ketoacidosis or subsequently from inanition owing to a chronic catabolic state, to a chronic degenerative disease. In the first 15 to 20 years of insulin therapy, a host of complications that had never been seen before was discovered in people with long-term diabetes (2). These complications, affecting the eyes, kidneys, and peripheral nervous system, were collectively called microvascular complications, to distinguish them from the less diabetes-specific but highly prevalent macrovascular disease complications. Microvascular disease and peripheral neuropathy resulted in blindness, kidney failure, and amputations (3); and macrovascular disease, exacerbated by renal dysfunction and autonomic neuropathy, increased the risk for myocardial infarctions and stroke to levels that were 10-fold or more than in the age-matched nondiabetic population (2,3).
The pathoetiology of the microvascular complications was vigorously debated during the mid-20th century (4–6). Some practitioners considered the complications a result of nonphysiologically controlled hyperglycemia; others thought that they were a glycemia-independent feature of diabetes. Perhaps the most sensible opinion regarding the role of glucose control, expressed by R.D. Lawrence, the preeminent diabetologist of his time and who had type 1 diabetes himself, was as follows: “The attempt to keep the blood sugar constantly normal may be ideal in theory, but in practice it is very difficult to achieve and makes the diabetic life unnecessarily hard without adequate benefit” (7).
The devastating consequences of the long-term complications led in part to the formation of the National Diabetes Commission by an Act of Congress (PL 93-354). In 1975, the Commission issued The Long-Range Plan to Combat Diabetes, which included the recommendation for the National Institutes of Health (NIH) to “initiate and support a 5-year clinical study to assess the effects of treatment of juvenile-onset diabetes on the development of microvascular and macrovascular complications.”
The advances necessary to perform a definitive clinical trial were finally in place by the early 1980s. These included: the ability to manage glucose levels in the near-normal range using multiple daily injection (MDI) therapy or continuous subcutaneous insulin infusion (CSII) with external pumps, guided by self-monitoring of blood glucose (SMBG); the means of measuring chronic glycemia objectively and accurately with the glycated hemoglobin (HbA1c) assay; and objective measures of long-term complications. With these tools available and with generous support from the National Institute of Arthritis, Diabetes, and Digestive and Kidney Diseases, which later became the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), 21 centers were selected in 1982 to plan and conduct a study that would test what had become known as the “glucose hypothesis.” Practically stated, the glucose hypothesis posited that achieving near-normal glucose would ameliorate the long-term complications of diabetes. Over the course of more than a year, the investigators planned the Diabetes Control and Complications Trial (DCCT) (8). The two primary aims of the DCCT consensus protocol were to determine whether, compared with conventional therapy (CON), an intensive treatment program designed to achieve glycemic control as close to the nondiabetic range as safely possible would prevent or delay the appearance of early background retinopathy (primary prevention) and would prevent the progression of early retinopathy to more advanced forms of retinopathy (secondary intervention).
After the successful completion of a 1-year feasibility phase, during which a substantial separation of HbA1c levels between the intensive therapy (INT) (“experimental”) and CON (“standard”) groups was achieved (9), an additional eight centers were added, and full-scale recruitment began. Recruitment ended in 1989, and the DCCT was halted by its independent oversight committee in 1993, approximately 1 year ahead of schedule, owing to the uniform and conclusive results achieved (10). The original CON group was taught INT, and the entire cohort was invited to join a long-term observational study named the Epidemiology of Diabetes Interventions and Complications (EDIC) (11). EDIC is now in its 20th year.
Research Design and Methods
The eligibility criteria have been described in detail (8,10). Briefly, in order to address the primary prevention and secondary intervention questions, the following eligibility criteria were used: age 13–39 years with type 1 diabetes diagnosed based on clinically accepted criteria and with fasting c-peptide concentrations <0.2 nmol/L. The subjects had to be generally healthy with no history of cardiovascular disease (CVD) and without hypertension (blood pressure <140/90 mmHg) or dyslipidemia (8), and those with neuropathy requiring treatment were excluded. Additionally, the primary prevention cohort had to have a duration of 1–5 years with no evidence of retinopathy on fundus photography and an albumin excretion rate (AER) <40 mg per 24 h. The secondary intervention cohort could have a longer duration of diabetes (1–15 years) and had to have at least one microaneurysm in either eye. This cohort could have an AER as high as 200 mg per 24 h. Subjects in the primary prevention cohort and those in the secondary intervention cohort with <5 years duration could have 2-h stimulated c-peptide levels as high as 0.5 nmol/L; otherwise, it had to be ≤0.2 nmol/L.
DCCT Interventions and Metabolic Goals
The clinical goals for both treatment groups included absence of frequent symptoms of hyperglycemia or frequent or severe hypoglycemia, defined as requiring assistance from another person. DCCT INT aimed to achieve HbA1c levels that were <2 SD above the mean value determined for similarly aged nondiabetic volunteers (<6.05%, 42.6 mmol/mol). HbA1c was measured monthly to aid adjustment of INT and quarterly as a process outcome in both therapy groups. Only the quarterly results were used for study data. INT was adjusted based on four or more SMBG tests with the following self-monitored glucose targets: premeals 70–120 mg/dL (3.9–6.7 mmol/L) and 2-h postmeals <180 mg/dL (10 mmol/L). In addition, a weekly 3:00 a.m. blood glucose was to be >65 mg/dL (3.6 mmol/L) in order to protect against otherwise unappreciated nocturnal hypoglycemia. To achieve the glycemic goals, participants randomly assigned to INT used at least three insulin injections per day (MDI) or CSII. The subjects and DCCT clinic staff chose which modality to use. The insulins used were those that were available at the time: clear zinc (regular) insulin for premeal boluses and in the insulin pump and NPH, lente, and beef ultralente insulin for basal delivery in MDI regimens. There was no single MDI or CSII regimen, and clinic staff and participants worked together to individualize the regimens to match lifestyle factors and achieve the SMBG and HbA1c goals (12).
CON was consistent with standard care in the 1980s and usually included one or two daily injections of insulin with daily urine or SMBG. The only numeric glycemic target was if HbA1c exceeded 13.5%, the mean +2 SD of the cohort’s baseline value, in which case treatment was intensified independent of whether the subject had symptoms.
Outcomes
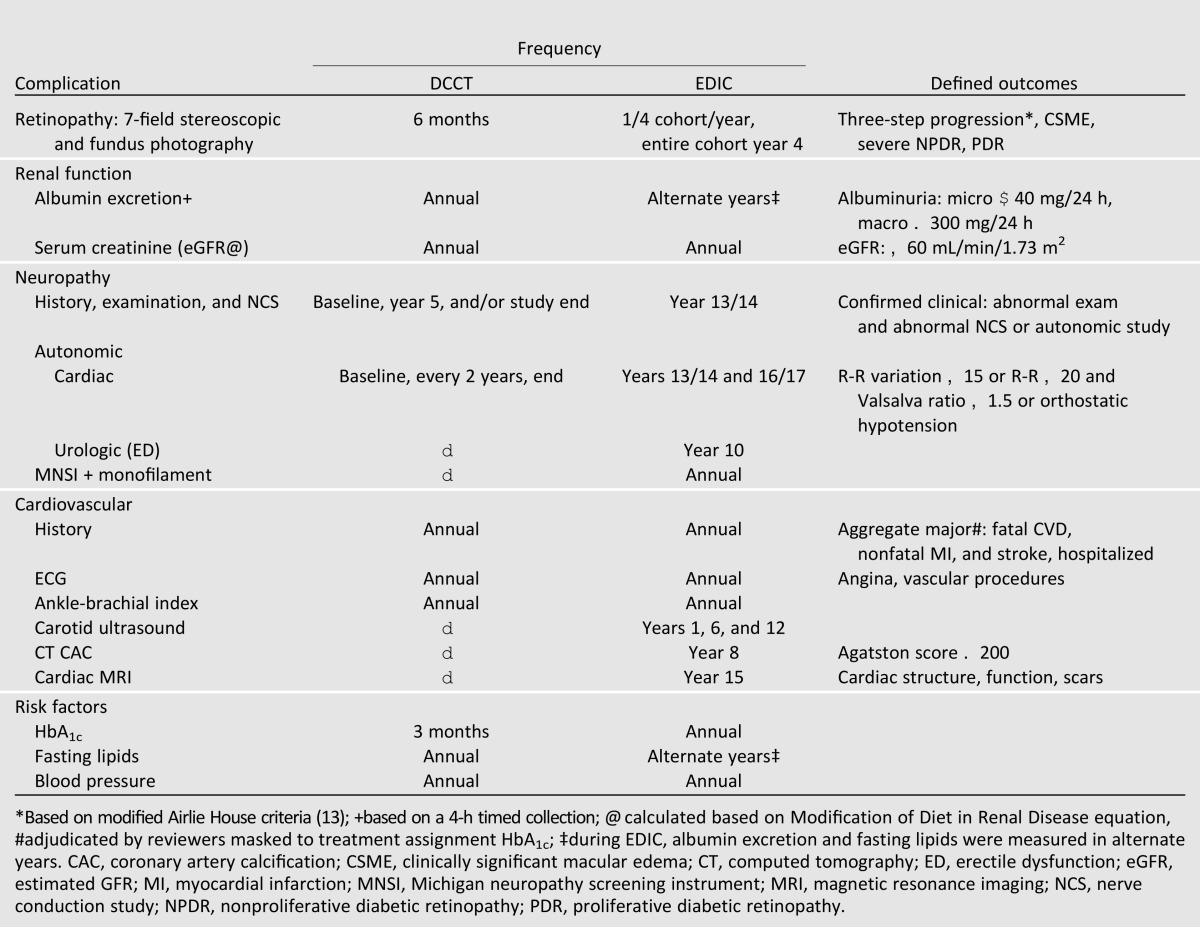
Retinopathy, which was measured objectively with stereoscopic fundus photography and graded with standardized methods by a central reading center (13), was the primary outcome used for power and sample-size calculations. Similarly important outcomes were nephropathy and retinopathy. The measurements and their frequency and definitions of outcomes are included in Table 1.
Table 1.
Major outcome measurements
EDIC Design and Outcomes
In the wake of the successful completion of the DCCT (10), the DCCT investigators and the NIDDK decided that longer-term follow-up would provide important information regarding the durability of the original DCCT INT effects and, in particular, the effects of INT on the more-advanced stages of complications and CVD (11). After the end of the DCCT and before initiating the long-term follow-up called EDIC, all of the CON participants were offered training in INT. In addition, diabetes care was returned to the subjects’ own care provider, some of whom were DCCT/EDIC investigators.
Whereas the DCCT was a controlled clinical trial, EDIC was observational. The frequency of interactions with the subjects and of the outcome measurements decreased substantially (Table 1); however, the methods of measuring glycemia, other metabolic outcomes, and complications remained identical to those used during DCCT. Several procedures were added to measure atherosclerosis (Table 1).
Results
Subjects
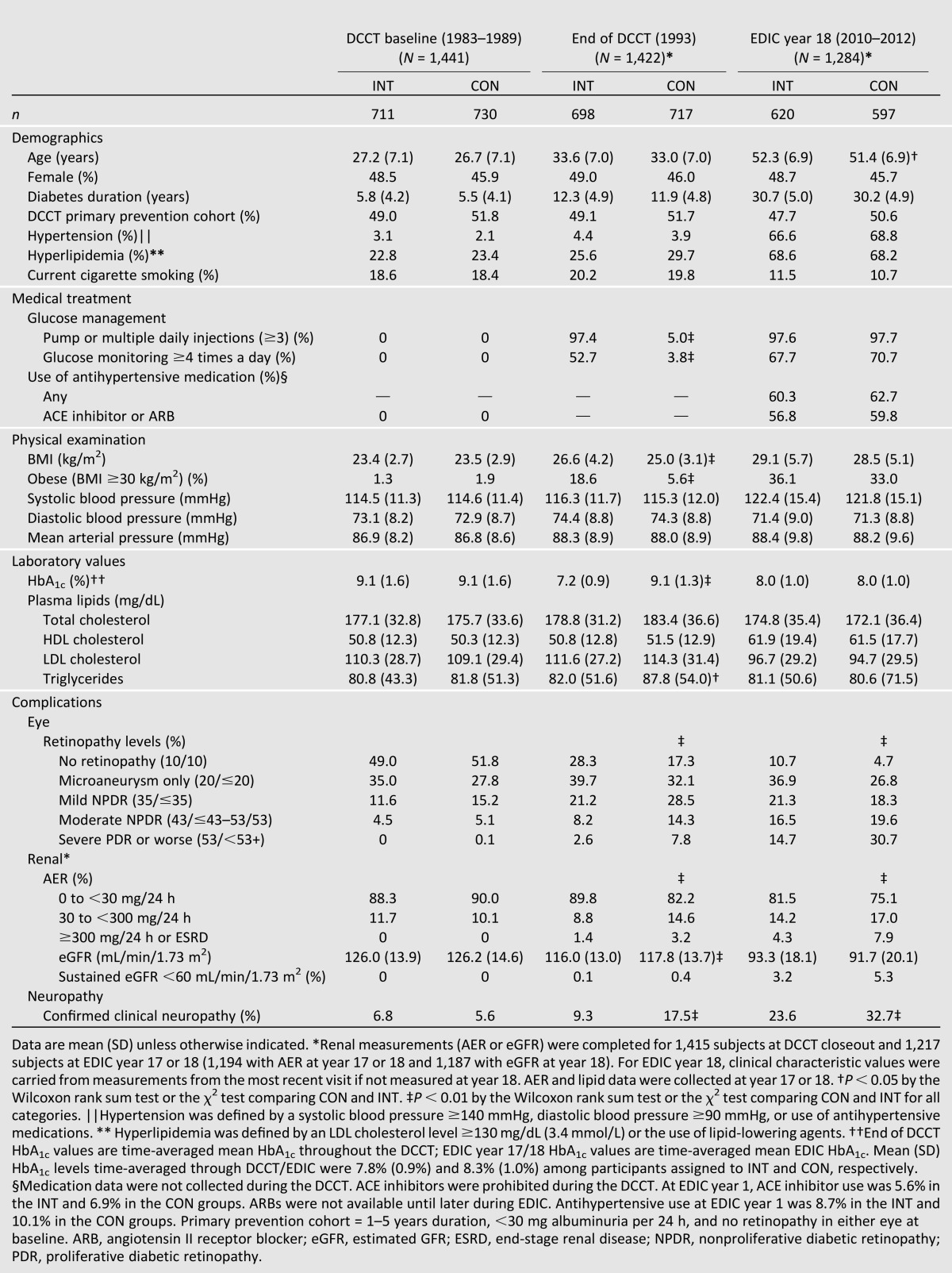
The characteristics of the DCCT cohort at baseline and at study end, which represents the EDIC baseline, and at the most recent EDIC annual examination in 2012 are shown in Table 2. The baseline characteristics were well matched between the INT and CON for the primary prevention and secondary intervention cohorts. The changes over time largely reflect the effects of INT versus CON. Although in most long-term studies loss to follow-up may compromise the integrity and interpretation of study results, the follow-up in DCCT and subsequently in EDIC has been virtually complete. At the end of DCCT, after an average of 6.5 years (range 3–9), more than 99% (1,422 of 1,441) completed the study. After another 20 years of follow-up in EDIC, 88% of the original cohort (95% of the survivors) is being actively followed in DCCT/EDIC clinical centers.
Table 2.
Clinical characteristics of DCCT/EDIC participants at DCCT baseline, DCCT closeout, and EDIC year 18
Glycemia
The DCCT INT did not uniformly achieve the goal HbA1c of <6.05%; however, 44% reached that level at least once during the trial (10). The median of the quarterly measured HbA1c levels in INT was 7% compared with 9% in CON (Fig. 1). There was almost no crossover between INT and CON during the DCCT, other than the protocol-dictated change to INT for women assigned to CON who were planning pregnancy and during pregnancy (14). 97% of study time was spent on assigned therapy. During EDIC, the adoption of INT by the original CON group and the transition for all subjects to their own health care providers resulted in a narrowing and then disappearance of the differences in HbA1c maintained during DCCT (Fig. 1).
Figure 1.

Median HbA1c concentrations during DCCT, the “training” period between DCCT and EDIC, and EDIC. P < 0.001 for INT vs. CON during entire DCCT and for the first 3 years during EDIC. Reprinted and modified with permission from Nathan et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study at 30 years: advances and contributions. Diabetes 2013;62:3976–3986.
Adverse Effects
The two major adverse events experienced by INT subjects were hypoglycemia and weight gain (15–17). The definition established for severe hypoglycemia, which has subsequently been adopted by many studies, was meant to be relatively inclusive but not to include episodes that were recognized and treated by the patients. To qualify as severe hypoglycemia, an episode had to require assistance from another and included coma or seizures or episodes requiring glucagon, IV dextrose, or oral carbohydrate administered by another person. Although the intent was to limit bias of ascertainment by collecting the hypoglycemia events at quarterly visits for both INT and CON subjects, INT subjects were seen and contacted more frequently than those in the CON group, and some of the differences in hypoglycemia may be attributable to differences in the frequency of ascertainment. The frequency of severe hypoglycemia (62/100 patient-years) and the subset of episodes involving coma or seizure (16/100 patient-years) were both threefold higher than in the CON group. Despite the increased frequency of hypoglycemia, there were no adverse effects of INT or of repeated severe episodes, on rigorously and repeatedly measured cognitive function in adults or adolescents, either during the DCCT or after even longer-term follow-up (18–20). Weight gain with INT resulted in significantly more subjects becoming overweight or obese compared with CON (17). The 4.6 kg difference in weight during the DCCT largely dissipated during the EDIC.
Outcomes
More detailed descriptions of the individual outcomes are presented in the subsequent articles in this series (21–25). In brief, DCCT INT reduced the early stages of microvascular complications by 35–76% compared with CON (Fig. 2) (10). The magnitude and consistent direction of the effects on retinopathy, neuropathy, and nephropathy led to the termination of the study 1 year ahead of schedule by the independent oversight group. Analyses of the relationship between metabolic control, measured by the “updated mean” HbA1c and including approximately 18,000 HbA1c measurements for each therapy group, revealed a strong association with each of the three complications (26,27). The difference in updated mean HbA1c levels between the therapy groups explained the vast majority (>98%) of the difference in complications between the groups (26), leaving little room for other established or putative risk factors to play a role in the trial’s differential outcomes.
Figure 2.

Summary of reduction in major complications with INT compared with CON during DCCT, EDIC, and combined study periods. 3+step devel, Prim: three-step or more development of retinopathy based on Early Treatment of Diabetic Retinopathy scale (ref. 13) in the primary prevention group. Scnd: secondary intervention group. Microalb: microalbuminuria defined as albumin excretion ≥40 mg/24 h. Macroalb: macroalbuminuria defined as albumin excretion >300 mg/24 h. Reduced GFR: estimated GFR <60 mL/min/1.73 m2. CVD events: CVD including myocardial infarctions, stroke, and CVD death. Reprinted with permission from Nathan et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study at 30 years: advances and contributions. Diabetes 2013;62:3976–3986.
EDIC/Metabolic Memory
Considering the powerful effect that glycemic separation had on the outcomes during DCCT, the subsequent narrowing and then disappearance of the difference in HbA1c levels between the two original therapy groups during EDIC could logically have been expected to result in the subsequent parallel development of complications. However, the first 4 years of the EDIC follow-up demonstrated a further widening of the differences in outcomes, after adjusting for EDIC baseline outcomes (28). This phenomenon of a durable effect on complications of prior metabolic control was named “metabolic memory.” It affects all of the microvascular complications (29–32). Studies during EDIC suggested that glycation of long-lived proteins, such as dermal collagen, might account for this persistent effect (33). Regardless of the mechanism, metabolic memory has lasted for at least 10 years.
The long-term EDIC follow-up has allowed the study of the impact of INT versus CON on more advanced complications than were studied during the DCCT. Major beneficial effects of INT on advanced complications (34), including retinopathy (35), nephropathy (reduced glomerular filtration rate [GFR]) (36), and autonomic manifestations of neuropathy (37), have been demonstrated (Fig. 2). Finally, measurements of atherosclerosis in several macrovascular beds, including carotid intima media thickness (38) and computed tomography–measured coronary artery calcification (39), have revealed less atherosclerosis in the INT group. The clinical expression of these changes, fatal and nonfatal myocardial infarctions and stroke, were also reduced by INT, with a 58% reduction in CVD events after a mean of 18 years of follow-up from the beginning of the DCCT (40).
Conclusions
The DCCT and its observational EDIC follow-up were designed to determine whether the long-term complications that affect people with type 1 diabetes could be ameliorated by intensive glycemic therapy. The DCCT/EDIC convincingly demonstrated that the glucose hypothesis was correct and that an intervention that aimed to achieve glycemia as close to the nondiabetic range as safely possible reduced all of the microvascular and cardiovascular complications of diabetes. Translating the findings of the DCCT/EDIC into clinical care has substantially improved the long-term health of people with type 1 diabetes.
Article Information
Funding. The DCCT/EDIC has been supported by U01 Cooperative Agreement Grants (1982–1993, 2011–2016) and contracts (1982–2011) with the Division of Diabetes Endocrinology and Metabolic Diseases of the National Institute of Diabetes and Digestive and Kidney Diseases (current grant numbers U01 DK094176 and U01 DK094157), and through support by the National Eye Institute, the National Institute of Neurological Disorders and Stroke, the Genetic Clinical Research Centers Program (1993–2007), and the Clinical Translational Science Center Program (2006–present), Bethesda, MD.
The following industry contributors have had no role in the DCCT/EDIC study but have provided free or discounted supplies or equipment to support participants’ adherence to the study: Abbott Diabetes Care (Alameda, CA); Animas (Westchester, PA); Bayer Diabetes Care (North America Headquarters, Tarrytown, NY); Becton, Dickinson and Company (Franklin Lakes, NJ); CanAm (Atlanta, GA); Eli Lilly (Indianapolis, IN); LifeScan (Milpitas, CA); Medtronic Diabetes (Minneapolis, MI); Nova Diabetes Care (Billerica, MA); Omron (Shelton, CT); OmniPod Insulin Management System (Bedford, MA); Roche Diabetes Care (Indianapolis, IN); and Sanofi (Bridgewater, NJ).
Duality of Interest. No potential conflicts of interest relevant to this article were reported.
Author Contributions. D.M.N. researched the data and wrote the manuscript. D.M.N. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Clinical trial reg. nos. NCT00360815 and NCT00360893, clinicaltrials.gov.
*A complete list of participants in the DCCT/EDIC Research Group can be found in N Engl J Med 2011;365:2366–2376.
References
- 1.Banting FG, Best CH. The internal secretion of the pancreas: 1922. Indian J Med Res 2007;125:251–266 [PubMed] [Google Scholar]
- 2.Nathan DM. Long-term complications of diabetes mellitus. N Engl J Med 1993;328:1676–1685 [DOI] [PubMed] [Google Scholar]
- 3.Deckert T, Poulsen JE, Larsen M. Prognosis of diabetes with diabetes onset before the age of thirty-one. Diabetologia 1978;14:363–377 [DOI] [PubMed] [Google Scholar]
- 4.Siperstein MD, Foster DW, Knowles HC, Jr, Levine R, Madison LL, Roth J. Control of blood glucose and diabetic vascular disease. N Engl J Med 1977;296:1060–1063 [DOI] [PubMed] [Google Scholar]
- 5.Boyd JD, Jackson RL, Allen JH. Avoidance of degenerative lesions in diabetes mellitus. JAMA 1942;118:694 [Google Scholar]
- 6.Dolger H. Clinical evaluation of vascular damage in diabetes mellitus. J Am Med Assoc 1947;134:1289–1291 [DOI] [PubMed] [Google Scholar]
- 7.Lawrence RD. The Diabetic Life: It’s Control by Diet and Insulin. 13th ed. J&A Churchill, 1944 [Google Scholar]
- 8.The DCCT Research Group The Diabetes Control and Complications Trial (DCCT): design and methodologic considerations for the feasibility phase. Diabetes 1986;35:530–545 [PubMed] [Google Scholar]
- 9.The DCCT Research Group Diabetes Control and Complications Trial (DCCT): results of feasibility study. Diabetes Care 1987;10:1–19 [DOI] [PubMed] [Google Scholar]
- 10.The Diabetes Control and Complications Trial Research Group The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977–986 [DOI] [PubMed] [Google Scholar]
- 11.Epidemiology of Diabetes Interventions and Complications (EDIC) Research Group Epidemiology of Diabetes Interventions and Complications (EDIC): Design and implementation of a long-term follow-up of the Diabetes Control and Complications Trial cohort. Diabetes Care 1999;22:99–111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Diabetes Control and Complications Trial Research Group Implementation of treatment protocols in the Diabetes Control and Complications Trial. Diabetes Care 1995;18:361–376 [DOI] [PubMed] [Google Scholar]
- 13.Early Treatment Diabetic Retinopathy Study Research Group Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology 1991;98(Suppl.):786–806 [PubMed] [Google Scholar]
- 14.The Diabetes Control and Complications Trial Research Group Pregnancy outcomes in the Diabetes Control and Complications Trial. Am J Obstet Gynecol 1996;174:1343–1353 [DOI] [PubMed] [Google Scholar]
- 15.The DCCT Research Group Epidemiology of severe hypoglycemia in the Diabetes Control and Complications Trial. Am J Med 1991;90:450–459 [PubMed] [Google Scholar]
- 16.The Diabetes Control and Complications Trial Research Group Hypoglycemia in the Diabetes Control and Complications Trial. Diabetes 1997;46:271–286 [PubMed] [Google Scholar]
- 17.The Diabetes Control and Complications Trial Research Group Adverse events and their association with treatment regimens in the Diabetes Control and Complications Trial. Diabetes Care 1995;18:1415–1427 [DOI] [PubMed] [Google Scholar]
- 18.The Diabetes Control and Complications Trial Research Group Effects of intensive diabetes therapy on neuropsychological function in adults in the Diabetes Control and Complications Trial. Ann Intern Med 1996;124:379–388 [DOI] [PubMed] [Google Scholar]
- 19.Jacobson AM, Musen G, Ryan CM, et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study Research Group Long-term effect of diabetes and its treatment on cognitive function. N Engl J Med 2007;356:1842–1852 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Musen G, Jacobson AM, Ryan CM, et al. DCCT/EDIC Research Group The impact of diabetes and its treatments on cognitive function among adolescents who participated in the DCCT. Diabetes Care 2008;31:1933–1938 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Aiello LP; DCCT/EDIC Research Group. Diabetic retinopathy and other ocular findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study. Diabetes Care 2014;37:17–23 [DOI] [PMC free article] [PubMed]
- 22.de Boer IH; DCCT/EDIC Research Group. Kidney disease and related findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study. Diabetes Care 2014;37:24–30 [DOI] [PMC free article] [PubMed]
- 23.Martin CL, Albers JW, Pop-Busui R; DCCT/EDIC Research Group. Neuropathy and related findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study. Diabetes Care 2014;37:31–38 [DOI] [PMC free article] [PubMed]
- 24.Lachin JM, Orchard TJ, Nathan DM; DCCT/EDIC Research Group. Update on cardiovascular outcomes at 30 years of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study. Diabetes Care 2014;37:39–43 [DOI] [PMC free article] [PubMed]
- 25.Gubitosi-Klug RA; DCCT/EDIC Research Group. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study at 30 years: summary and future directions. Diabetes Care 2014;37:44–49 [DOI] [PMC free article] [PubMed]
- 26.The Diabetes Control and Complications Trial Research Group The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the Diabetes Control and Complications Trial. Diabetes 1995;44:968–983 [PubMed] [Google Scholar]
- 27.Lachin JM, Genuth S, Nathan DM, Zinman B, Rutledge BN, DCCT/EDIC Research Group Effect of glycemic exposure on the risk of microvascular complications in the Diabetes Control and Complications Trial—revisited. Diabetes 2008;57:995–1001 [DOI] [PubMed] [Google Scholar]
- 28.Lachin J, Genuth S, Nathan D, Davis M, The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N Engl J Med 2000;342:381–389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lipps J, Lorenzi G, Genuth S, Nathan D, Davis M, Lachin J, Cleary P; for the DCCT/EDIC Research Group. The effect of intensive therapy on the microvascular complications of type 1 diabetes mellitus. JAMA 2002;287:2563–2569 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.White NH, Sun W, Cleary PA, et al. Prolonged effect of intensive therapy on the risk of retinopathy complications in patients with type 1 diabetes mellitus: 10 years after the Diabetes Control and Complications Trial. Arch Ophthalmol 2008;126:1707–1715 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Pop-Busui R, Low PA, Waberski BH, et al. DCCT/EDIC Research Group Effects of prior intensive insulin therapy on cardiac autonomic nervous system function in type 1 diabetes mellitus: the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study (DCCT/EDIC). Circulation 2009;119:2886–2893 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Albers JW, Herman WH, Feldman EL, et al. ; the DCCT/EDIC Research Group. Effect of prior intensive insulin treatment during the Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type 1 diabetes during the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. Diabetes Care 2010;33:1090–1096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Monnier VM, Bautista O, Kenny D, et al. ; the DCCT Collagen Ancillary Study Group. Skin collagen glycation, glycoxidation, and crosslinking are lower in subjects with long-term intensive versus conventional therapy of type 1 diabetes: relevance of glycated collagen products versus HbA1c as markers of diabetes complications. Diabetes 1999;48:870–880 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nathan DM, Zinman B, Cleary PA, et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Research Group Modern-day clinical course of type 1 diabetes mellitus after 30 years’ duration: the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications and Pittsburgh Epidemiology of Diabetes Complications Experience (1983-2005). Arch Intern Med 2009;169:1307–1316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Aiello LP, Sun W, Cleary P, Lachin SM, Gangaputra S, Davis MD, Klein R, Das A, Kiss S, Domalpally A, Danis R; DCCT/EDIC Research Group. Intensive diabetes therapy reduces ocular surgeries in patients with type 1 diabetes: twenty-eight year follow-up of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study (Abstract). ARVO Meeting Abstracts 2013;54:4024
- 36.de Boer IH, Sun W, Cleary PA, et al. DCCT/EDIC Research Group Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes. N Engl J Med 2011;365:2366–2376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wessells H, Penson DF, Cleary P, et al. ; the DCCT/EDIC Research Group: effect of intensive glycemic therapy on erectile function in men with type 1 diabetes. J Urol 2011;185:1828–1836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nathan DM, Lachin J, Cleary P, et al. Diabetes Control and Complications Trial. Epidemiology of Diabetes Interventions and Complications Research Group Intensive diabetes therapy and carotid intima-media thickness in type 1 diabetes mellitus. N Engl J Med 2003;348:2294–2303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cleary PA, Orchard TJ, Genuth S, et al. DCCT/EDIC Research Group The effect of intensive glycemic treatment on coronary artery calcification in type 1 diabetic participants of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study. Diabetes 2006;55:3556–3565 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Nathan DM, Cleary PA, Backlund JY, et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005;353:2643–2653 [DOI] [PMC free article] [PubMed] [Google Scholar]