

Abstract
Background & objectives:
The relationship between obesity and self perception, particularly in children and young adults has important implications for physical and psychosocial health and well-being. A better understanding of this relationship could help target psychology services and public health strategies more effectively. The aim of the present study was to assess the effect of body mass index (BMI) on physical self concept and cognition of the first year medical undergraduate students in a medical college in north India. The relationship between physical self concept and academic performance and presence of any gender differences were also examined.
Methods:
The study was carried out on 18-21 yr old first year M.B.B.S. students of Maulana Azad Medical College, New Delhi, India. Physical self concept was assessed using short version of Physical Self Description Questionnaire (PSDQ-S) which is a psychometrically strong instrument for measuring multiple dimensions of physical self-concept. Cognition was assessed by P300 evoked potentials and academic performance was evaluated on the basis of marks obtained in anatomy, physiology and biochemistry subjects.
Results:
There was no association between BMI and physical self-concept or between BMI and cognition. Gender differences on physical self-concept were also insignificant. No correlation was seen between physical self-concept and academic performance.
Interpretation & conclusion:
The present results suggest that negative consequences of high body mass index on physical self-concept and cognition are not seen in young adults. It may be that academic achievement nullifies the effect on physical self-concept and the effect on cognition accumulates as the age progresses, therefore, appears later in life.
Keywords: Academic performance, body mass index, cognition, PSDQ-S
The prevalence of obesity is increasing worldwide and the major causative factors are related to lifestyle changes occurring due to rapid socio-economic transition. Reduced physical activity at work due to mechanization, improved motorized transport, preferences for viewing television and video games during leisure time and consumption of fast food and sweetened carbonated drinks have resulted in positive energy balance in most of the Asian countries1,2. As youths move through adolescence, their participation in physical activity declines markedly3,4. The immediate risks of obesity for physical health are well established. However, studies based predominantly on western research have shown that obesity in childhood may have adverse effects on cognitive performance and self concept development5. Shavelson et al6 have defined self concept as an individual's perception of self formed through experience with environment, interactions with significant others and attributions of his/her own behaviour. It is multi-dimensional and hierarchically organized. Self-esteem or general self-concept is positioned at the apex and is divided into academic (English and Maths) and non-academic (Physical, social and emotional) components6. Marsh and Craven7 have shown that academic achievement though systematically related to academic self concept is nearly uncorrelated (or even negatively related) to non academic components of self concept. In another study, Crandall8 has observed that individuals are discriminated against on the basis of weight; that this discrimination generalizes over race, gender, age and socio-economic status, and that the associated stigmatization influences the individuals self-perceptions and perceptions by significant others.
Based upon Shavelson's model of self-concept, Marsh et al9 developed the Physical Self Description Questionnaire (PSDQ) in which nine components specific to physical self-concept (strength, body fat, activity, endurance, sports competence, co-ordination, health, appearance and flexibility) and two general components (global physical self concept, and global esteem) are measured. The PSDQ is a comprehensive, valid, stable and consistent instrument designed to measure multiple dimensions of physical self-concept.
There is a growing evidence that obesity is associated with impaired cognitive function including executive function, attention and memory not only in patients with co-morbid medical conditions like cerebrovascular pathology, hypertension and diabetes but also in healthy subjects10. The mechanisms underlying this effect are not understood. The P300 event-related potential (ERP) reflects neuroelectric activity related to cognitive processes such as attention allocation and activation of immediate memory. The P300 latency time is generally accepted as a measure of speed of cognitive processing, and its amplitude to reflect the number of neurons allocated to the eliciting task11,12. It is clinically used as an index of cognitive function.
Given that obesity and self perception are both amenable to intervention, an examination of the nature of relationship between obesity and self-perception has important implications for physical and psychosocial health and well-being. The present study was undertaken to assess the amplitude and latency of P300 along with PSDQ-S in 18-21 yr old first year undergraduate medical (M.B.B.S.) students to determine if any relationships exist between the body mass index (BMI) and physical self concept, gender and physical self concept, BMI and cognition, and physical self concept and academic performance.
Material & Methods
The study was conducted in the department of Physiology, Maulana Azad Medical College, New Delhi, India, during December 2011.
Subjects: The study population consisted of 30 first year MBBS students of both sexes belonging to 2011-2012 batch of Maulana Azad Medical College, New Delhi. The height and weight of each student was recorded and BMI was calculated as the weight in kilograms divided by the square of height in meters. Subjects were divided into two groups depending on new BMI cut off point for Indian population13. All obese students with BMI ≥25 kg/m2 (n=30) were considered to form the study group. The students with normal weight and BMI of 18 to 22.9 kg/m2 (n=30) were selected randomly to form the control group. There were only a few students with BMI in the range 23-24.9 kg/m2. Therefore, the overweight category was excluded and the study was restricted to normal weight and obese categories. The average age for control and study groups was 18.58 ± 0.67 and 18.81 ± 1.11 yr, respectively.
Measuring instruments: The physical self concept was evaluated by using PSDQ-S and cognition by P300 event related potential (ERP). PSDQ-S is a short version of PSDQ with all the psychometric strength of the longer version plus the advantage of a reduced length from 70 to 47 items14. Each item is a simple declarative statement in which responses vary from false [1] to true [6] on a 6 point Likert Scale. The scoring for the negatively worded items [8,11,17,19,22,25,29,30,33,39,46,47] was reversed. Total score of the PSDQ-S ranged from 47 to 282. The scoring was done using multi-dimensional profile as self concept is better captured by multi-dimensional profile of self-concept scores rather than a single self-esteem score15.
Procedure: Written informed consent was obtained from the students and PSDQ was administered to all the students on a single occasion. Confidentiality of subject's information and data were maintained. The questionnaires were distributed during class time and instructions delivered verbally to complete the PSDQ-S sincerely and no discussion was allowed throughout the test. Ethical clearance was obtained from the Institutional ethics committee.
Event related potentials recording: ERPs are generated by subject's response to auditory, visual or other sensory stimuli. Auditory stimuli were used in this study. An auditory cognitive ERP is generated by playing a baseline series of frequently occurring rhythmic auditory stimuli for a subject and then presenting secondary auditory stimuli (rare stimulus) at random. The subject mentally counts the secondary auditory “oddball” (rare) stimuli, and this specific intellectual function generates a discrete waveform of cognitive evoked response called the P300 component since its latency is about 300 ms (millisecond) after the stimulus16. EB Neuro machine (Evoked potential measuring system- Galileo NT) supplied by Firenze, Italy was used to record the evoked potentials. The evoked potentials were recorded as per the guidelines of International Federation of Clinical Neurophysiologists (IFCN)17. The examination was conducted under standardized conditions in all the subjects. The subjects assumed a comfortable position in a standard audiometric, sound proof, and air conditioned room so that they were relaxed. The method was fully explained to all the subjects to get the best compliance. During the P300 recording session subject was instructed to fixate his/her eyes on a particular spot on the ceiling in order to avoid artefacts due to eye movements and improve his concentration and attention to target stimulus. Silver/silver chloride disc electrodes were used. Foremost the scalp sites were cleaned with a cotton pad moistened with alcohol and then rubbed with an appropriate amount of Neuprep skin prepping jelly to abrade the skin for impedance reduction. The disc electrodes with 10-20 EEG conducting paste were applied to the sites. The active electrodes were placed using the 10-20 international system on Fz, Pz and Cz sites referred to linked earlobes with a forehead ground. Electrode to skin impedance was kept below 5 kiloohms. P300 was measured in response to random application of two types of stimuli. “Odd-ball” acoustic paradigm was adopted, 200 stimuli were presented of which 40 were the rare or the target stimuli; 80 per cent of the tones were frequent (500 Hz stimuli) and 20 per cent were rare (2000 Hz stimuli), randomly received by patients. Acoustic stimuli were of 80 dB each. Linear tone with a starting condensation phase with a plateau phase of 100ms, rise/fall of 10ms and a rate of once every one second was used. The signals were in phase at the two ears. The Galileo NT settings were selected so as to filter the evoked responses to the frequent and the rare stimuli with a band pass of 0.1-20 Hz and averaged simultaneously for 40 responses.
The P300 wave was identified as the largest positive peak occurring for all electrode sites with latency more than 250ms. The latency and amplitude of the waveform were recorded. The latency was calculated from the point of stimulation. It has already been demonstrated by other researchers that the quality of cognitive response is interrelated to amplitude and latency of the P300 wave, with higher amplitudes and shorter latencies being linked with improved cognitive function18.
Academic performance was evaluated on the basis of marks obtained in all the tutorials, completion tests and first terminal exams of Anatomy, Physiology and Biochemistry subjects.
Statistical analysis: Descriptive statistics were used to calculate the means and standard deviations of the BMI, P300 amplitude and latency and the eleven PSDQ subscales scores for the subjects. Pearson's product moment correlations were used to examine the relationships between BMI and P300 amplitude and latency and also between BMI and scores on the PSDQ with significance set at <0.05. Independent t-tests were employed to examine gender differences and also the differences between obese and non-obese subjects. All analyses were carried out on SPSS Version 17 (SPSS Inc. Chicago, IL). The Cronbach's alpha coefficients for this sample were found to be adequate for all eleven subscales.
Results
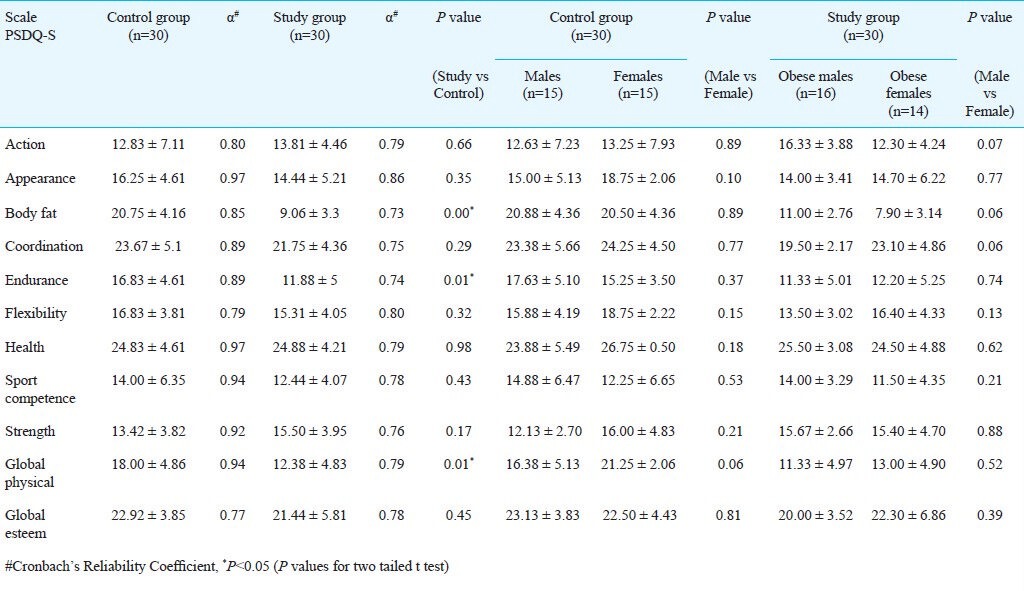
The characteristics of the study and control groups are summarized in Table I. The mean weight and BMI of the study group were significantly higher (P<0.05) than that of control group. The scores of eleven subscales of PSDQ-S, comparison of scores between the study and control group and between obese males and females of the study group are presented in Table II. Except for body fat, endurance and global physical all other subscales did not differ significantly between the two groups (study vs control). No differences were found for the physical self-concept scales between males and females in both study and control groups.
Table I.
Characteristics of study and control population
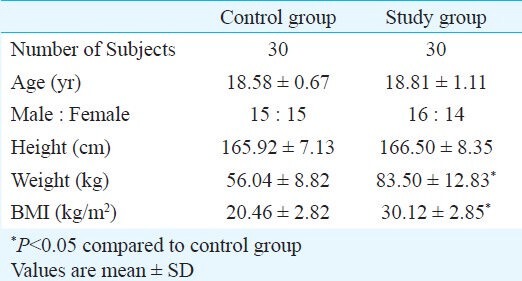
Table II.
Descriptive statistics and internal consistency reliability for short version of Physical Self Description Questionnaire (PSDQ-S)
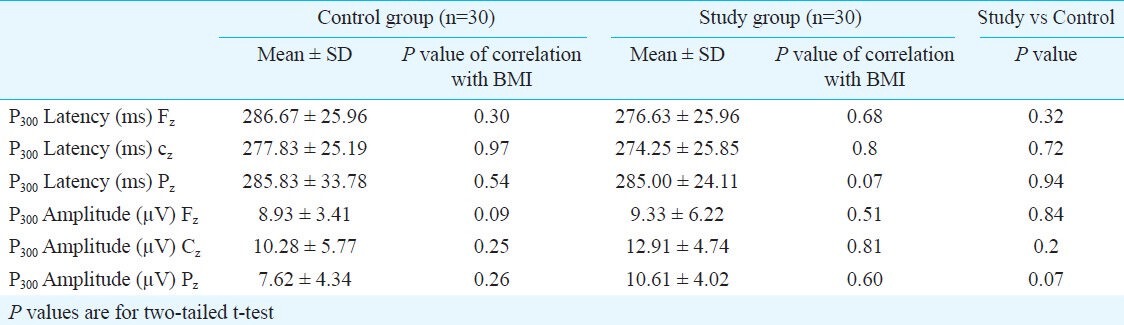
The findings of cognitive evaluation are summarized for both groups in Table III. There was no correlation between BMI and the P300 amplitude and latency.
Table III.
Evoked potentials in the study and control groups
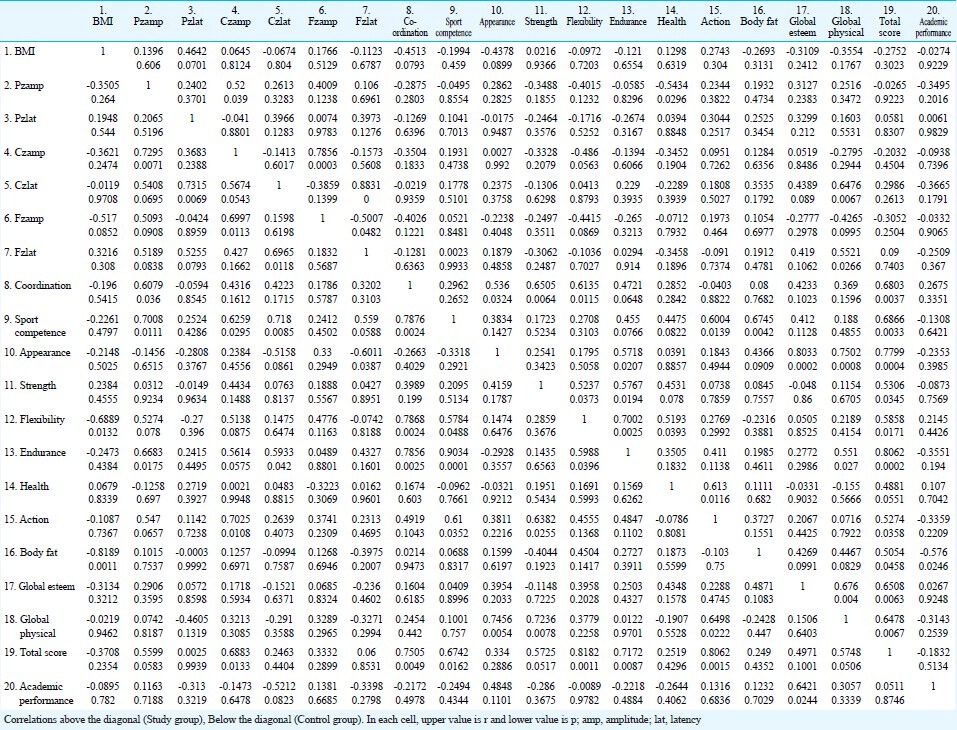
For comparison, correlations among the PSDQ-S sub-scales and BMI, academic performance and P300 amplitude and latency are presented separately for control and study groups in Table IV.
Table IV.
Correlations of PSDQ-S subcales with BMI, P300 and academic performance among normal weight and obese first year medical student
Discussion
The study was designed to examine the relationships between BMI and cognition and between BMI and physical self-concept. The effect of gender differences on physical self-concept and the relationship between physical self-concept and academic performance were also studied.
In concurrence to a previous study on self-concept research19, our results have shown small declines in the scores of the 11 subscales of physical self-concept in the obese subjects. However, this trend was found to be significant only for the endurance, body fat and the global physical subscales. There were no significant differences between the two groups in terms of global self esteem. These results demonstrate that being obese i.e. the presence of a socially undesirable characteristic has little negative consequence on the self perceptions of Indian students. Similar results have been reported earlier in a study carried out on Chinese students aged 8-15 yr15. The authors have suggested that apparently the negative stigma associated with obesity varies from culture to culture and, therefore, there are no negative consequences in Chinese students. Studies based predominantly on western research have shown that obese children and adolescents have significantly lower self esteem20,21.
BMI showed no significant correlation with the 11 subscales of physical self-concept. This further suggests that factors associated with self esteem may be related to culture and, therefore, obesity apparently does not have the socially undesirable connotations for Indian youth. The pattern of obesity stigmatization is not uniform across race and gender. A study by Michelle and Julie22 indicates that standards and ideals of weight differ among White and Black Americans. They have concluded that the consequences of obesity may differ by race as a result of cultural differences in ideal body size and obesity stigma. Similarly, Lee and Lee23 have shown that the desire for thin body varies as a function of location. They carried out a research on high school girls in three cities which differed substantially in the degree of westernization and modernization (Hong Kong, Shenzhen and rural Hunan) and found that the desire for a lower BMI was highest in the most modern city (Hong Kong) and lowest in the least modern city (rural Hunan)23.
Marsh et al24 reported reciprocal effects between self-concept and accomplishment i.e. self-concept is both a cause of subsequent accomplishments and an effect of prior accomplishments. Our study subjects were first year undergraduate medical students of a prestigious medical college which in itself is a big academic achievement. It may be inferred that academic achievement has nullified the negative impact, if any, of obesity on self concept and hence there are no differences between the obese and non-obese medical students. The absence of significant association between BMI and self perception could be a consequence of small sample size.
No gender differences have been observed in the overall self-concept. However, it was observed that females have scored more on co-ordination and flexibility while males have scored more on sports competence. These findings support the earlier views that there was no evidence for sex differences in overall self-concept at any age level, however, sex differences do exist in specific components of self-concept25.
In the present study, no association between BMI and cognition was established. There were no significant differences in the P300 amplitude and latency at Fz, Cz and Pz sites between the obese and non-obese students. This was in contrast to a previous prospective study which has shown that those with a higher BMI in midlife were at a higher risk of cognitive impairment later in life26. The authors have suggested that perhaps obesity leads to thickening and hardening of cerebral blood vessels and the development of insulin resistance25. In another study, Raji et al27 have reported that BMI>30kg/m2 was associated with atrophy in frontal lobes, the anterior cingulated gyrus, hippocampus and thalamus as compared to normal weight individuals. The reason for discrepancy in the present study may be due to the young age (18-21 yr) of subjects, as the steepest decline in cognition occurs in late middle age. It appears that the effect of obesity on cognition accumulates over the adult life course and, therefore, it is important to use a life-course approach to study the association between BMI and cognition28. Another limitation for the present study was that the physical activity was not measured; thus, it is not possible to rule out its contribution, particularly because physical activity has already been shown to have a beneficial effect on cognition29.
No significant correlation was found between the 11 subscales of physical self-concept and academic performance. Alexander30 and Castor31 in two independent separate studies have shown that non-academic self-concept does not correlate significantly with measures of academic performance whereas academic self-concept strongly correlates with academic achievement. It seems that certain groups of people may be less susceptible to experiencing academic decline due to being obese. However, obese females exhibited higher academic performance than obese males. This was consistent with the earlier findings which documented gender differences in relation between obesity levels and academic achievement32.
In conclusion, no association was observed between BMI and physical self-concept and also between BMI and cognition. Gender differences on physical self-concept were also insignificant. Further research is needed in large number of subjects of different age groups (preadolescents, adolescents and adults) and economic/professional groups to evaluate the generalizability of present results.
References
- 1.Parizkova J, Chin MK, Chia M, Yang J. An international perspective on obesity, health and physical activity: current trends and challenges in China and Asia. J Exerc Sci Fit. 2007;5:7–23. [Google Scholar]
- 2.Cheng TO. Fast food and obesity in China. J Am Coll Cardiol. 2003;42:773. doi: 10.1016/s0735-1097(03)00792-7. [DOI] [PubMed] [Google Scholar]
- 3.Caspersen CJ, Pereira MA, Curran KM. Changes in physical activity patterns in the United states, by sex and cross-sectional age. Med Sci Sports Exerc. 2000;32:1601–9. doi: 10.1097/00005768-200009000-00013. [DOI] [PubMed] [Google Scholar]
- 4.Kimm SY, Glynn NW, Kriska AM, Barton BA, Kronsberg SS, Daniels RS, et al. Decline in physical activity in Black girls and White girls during adolescence. N Engl J Med. 2002;347:709–15. doi: 10.1056/NEJMoa003277. [DOI] [PubMed] [Google Scholar]
- 5.Braet C, Mervielde I, Vandereycken W. Psychological aspects of childhood obesity: A controlled study in a clinical and nonclinical sample. J Pediatr Psychol. 1997;22:59–71. doi: 10.1093/jpepsy/22.1.59. [DOI] [PubMed] [Google Scholar]
- 6.Shavelson RJ, Hubner JJ, Stanton GC. Validation of construct interpretations. Rev Educ Res. 1976;46:407–41. [Google Scholar]
- 7.Marsh HW, Craven RG. Reciprocal effects between academic self-concept, self-esteem, achievement, and attainment over seven adolescent years: Unidimensional and multidimensional perspectives of self-concept. Perspect Psychol Sci. 2006;1:133–63. doi: 10.1177/0146167207312313. [DOI] [PubMed] [Google Scholar]
- 8.Crandall CS. Do heavy weight students have more difficulty paying for college? Pers Soc Psychol B. 1991;17:606–11. [Google Scholar]
- 9.Marsh HW, Richards GE, Johnson S, Roche L, Tremayne P. Physical Self Description Questionnaire: Psychometric properties and a multitrait-multimethod analysis of reactions to existing instruments. J Sport Exerc Psychol. 1994;16:270–305. [Google Scholar]
- 10.Gunstad D, Paul RH, Cohen RA, Tate DF, Spitznagel MB, Gordon E. Elevated body mass index is associated with executive dysfunction in otherwise healthy adults. Compr Psychiatry. 2007;48:57–61. doi: 10.1016/j.comppsych.2006.05.001. [DOI] [PubMed] [Google Scholar]
- 11.Kutas M, MacCarthy G, Donchin E. Augmenting mental chronometry: The P300 as a measure of stimulus evaluation. Science. 1977;197:792–5. doi: 10.1126/science.887923. [DOI] [PubMed] [Google Scholar]
- 12.Wickens C, Kramer A, Vanasse L, Donchin E. The performance of concurrent tasks: A psychophysiological analysis of the reciprocity of information processing resources. Science. 1983;221:1080–2. doi: 10.1126/science.6879207. [DOI] [PubMed] [Google Scholar]
- 13.Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus Statement for Diagnosis of Obesity, Abdominal Obesity and the Metabolic Syndrome for Asian Indians and Recommendations for Physical Activity, Medical and Surgical Management. J Assoc Physicians India. 2009;57:163–70. [PubMed] [Google Scholar]
- 14.Marsh HW, Martin AJ, Jackson S. Introducing a short version of the physical self description questionnaire: new strategies, short-form evaluative criteria, and applications of factor analyses. J Sport Exerc Psychol. 2010;32:438–82. doi: 10.1123/jsep.32.4.438. [DOI] [PubMed] [Google Scholar]
- 15.Marsh HW, Hau KT, Sung RY, Yu CW. Childhood obesity, gender, actual- ideal body image discrepancies, and physical self-concept in Hong Kong children: Cultural differences in the value of moderation. Dev Psychol. 2007;43:647–62. doi: 10.1037/0012-1649.43.3.647. [DOI] [PubMed] [Google Scholar]
- 16.Qureshi N, Babbar R. Effect of ramipril therapy on cognitive functions in cases of mild to moderate essential hypertension. Indian J Physiol Pharmacol. 2007;51:40–8. [PubMed] [Google Scholar]
- 17.Nuwer MR, Lehmann D, Silva FLD, Matsuoka S, Sutherling W. IFCN guidelines for topographic and frequency analysis of EEGs and EPs. Report of an IFCN committee. International Federation of Clinical Neurophysiology. Electroencephalogr Clin Neurophysiol. 1994;91:1–5. doi: 10.1016/0013-4694(94)90011-6. [DOI] [PubMed] [Google Scholar]
- 18.Stivelman JC. Benefits of anaemia treatment on cognitive function. Nephrol Dial Transplant. 2000;15(Suppl 3):29–35. doi: 10.1093/oxfordjournals.ndt.a027973. [DOI] [PubMed] [Google Scholar]
- 19.Marsh HW. Age and sex effects in multiple dimensions of self-concept: Preadolescence to adulthood. J Educ Psychol. 1989;81:417–30. [Google Scholar]
- 20.Pierce JW, Wardle J. Cause and effect beliefs and self- esteem of overweight children. J Child Psychol Psychiatr. 1997;38:645–50. doi: 10.1111/j.1469-7610.1997.tb01691.x. [DOI] [PubMed] [Google Scholar]
- 21.French SA, Story M, Perry CL. Self esteem and obesity in children and adolescents: a literature review. Obes Res. 1995;3:479–90. doi: 10.1002/j.1550-8528.1995.tb00179.x. [DOI] [PubMed] [Google Scholar]
- 22.Michelle RH, Julie MT. The stigma of obesity: What about Men? Basic Applied Soc Psychol. 2005;27:267–75. [Google Scholar]
- 23.Lee S, Lee AM. Disordered eating in three communities of China: a comparative study of female high school students in hong kong, Shenzhen, and rural hunan. Int J Eat Disord. 2000;27:317–27. doi: 10.1002/(sici)1098-108x(200004)27:3<317::aid-eat9>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 24.Marsh HW, Hau KT, Kong CK. Multilevel causal ordering of academic self-concept and achievement: Influence of language of instruction (English Vs Chinese) for Hongkong students. Am Educ Res J. 2002;39:727–63. [Google Scholar]
- 25.Wylie R. Lincola: University of Nebraska; 1979. The self-concept, vol. II: Theory and research on selected topics. [Google Scholar]
- 26.Cournot M, Marquie JC, Ansiou D, Martinaud C, Fonds H, Ferrieres J, et al. Relation between Body Mass Index and cognitive function in healthy middle-aged men and women. Neurology. 2006;67:1208–14. doi: 10.1212/01.wnl.0000238082.13860.50. [DOI] [PubMed] [Google Scholar]
- 27.Raji CA, Ho AJ, Parikshak NN, Becker JT, Lopez OL, Kuller LH, et al. Brain structure and obesity. Hum Brain Mapp. 2010;31:353–64. doi: 10.1002/hbm.20870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gustafson D. Adiposity indices and dementia. Lancet Neurol. 2006;5:713–20. doi: 10.1016/S1474-4422(06)70526-9. [DOI] [PubMed] [Google Scholar]
- 29.Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart; exercise effects on brain and cognition. Nat Rev Neurosci. 2008;9:58–65. doi: 10.1038/nrn2298. [DOI] [PubMed] [Google Scholar]
- 30.Alexander S. Cleveland State University; 1997. The relationship of self-concept, IQ, academic performance, and stressors to coping abilities for Urban African-American gifted students. [Google Scholar]
- 31.Castor SE. Ball State University; 1996. Locus of control and self-concept in achieving and under achieving gifted students. [Google Scholar]
- 32.Datar A, Strum R. Childhood overweight and elementary school outcomes. Int J Obes. 2006;30:1449–60. doi: 10.1038/sj.ijo.0803311. [DOI] [PubMed] [Google Scholar]