

Abstract
Background:
Health care in prisons is one of the neglected health areas in our country. Looking into the health problems of prisons will show us a way for the approach in providing the heath care for prisoners.
Objectives:
To assess the health status of convicted inmates of prison and to study their sociodemographic profile.
Materials and Methods:
A cross-sectional study was conducted among the inmates of central prison over a period of 1 year. Study population comprised of 300 convicted life-term prisoners. The inmates were interviewed using predesigned and pretested proforma. Sociodemographic data were analyzed by frequencies and percentages along with 95% confidence interval using statistical package SPSS18.
Results:
In health status, 29 (9.6%) inmates suffered from acute upper respiratory tract infections and 15 (5%) from acute lower respiratory tract infections. A total of 54 (18%) inmates had ascariasis. Diseases of musculoskeletal system and connective tissue contributed to 26 (8.7%) of inmates. A total of 252 (84%) prisoners had anemia. In sociodemographic profile, it was found that rural people, unmarried, illiterates, lower socioeconomic status people were more likely to have committed the crime resulting in the conviction for life.
Conclusions:
As there is an increase in number of prisoners and morbidities among them, there is an urgent need for prison health care services in developing countries like India and provide training to the health care providers to manage the commonly existing health problems among prisoners in the prisons.
Keywords: Health status, jail, prisoners, prisons
INTRODUCTION
Prison population consists of an over representation of members of the most marginalized groups in society, people with poor health and chronic untreated conditions. This population is an underserved section of the society. Often their health problems are neglected. They carry a much greater burden of illness than other members of the society; they harbour diseases that are determined both by the environment out of which they come and by the prison in which they live. “Prison” means any jail or place used permanently or temporarily under the general or special orders of the state government for the detention of prisoners and includes all lands and buildings appurtenant thereto, but does not include any place for the confinement of prisoners who are exclusively in the custody of the police or any place declared to be a subsidiary jail. It is not a place where someone would like to live. Whatever are the reasons behind incarceration? Whether it is seen as a punishment or as a mode of rehabilitation? The normal life of the inmate is restricted, freedom of movement is curtailed, and private space is limited. Many of the prisons over the globe are overburdened; the population confined behind bars in the US in 2008 was in excess of 1.6 million.[1] In India too, the situation is no better. There are about 1276 prisons in the country with an authorized accommodation of 2,77,304; however, the total number of jail inmates is nearing 4 lacs indicating severe overcrowding in prisons.[2]
There are problems of drug abuse, alcoholism, trauma, homicide, suicide, violence, neuropsychiatric diseases, epilepsy, stress manifestations, HIV infection and AIDS, sexually transmitted diseases, tuberculosis, skin infections, and so on. In the walls of the jails, the lack of adequate health facilities amounts to society inflicting punishment twice, once by incarceration and a second time by illness. The second punishment has potential to get inflicted on the family of prisoners. For example, in case a prisoner in US prison, his undetected tuberculosis got ultimately transmitted to his wife and two children one of whom died. Reforming the delivery of prison health care is one of the most important aspects of improving human rights compliance. Therefore, knowing the burden and types of morbidities among them will help policy planners and administrators in taking actions to minimize the disease burden in this group and also to help in reintegration of prisoners into main stream of society following their discharge from prison. Therefore, present study was conducted with the aim of studying the health status of persons from a section of our society, who were condemned by law and are behind the high walls of one of the largest prisons of our country that is “central prison of Gulbarga” India. Objectives of the study were (a) to study the sociodemographic characteristics of the jail inmates and (b) to estimate the prevalence of various morbidities.
MATERIALS AND METHODS
The present cross-sectional study was carried out in the central prison of Gulbarga city. The city of Gulbarga is a divisional head quarter of Hyderabad-Karnataka region of Karnataka state of the India. It was a part of Nizam state prior to the reorganization of state in 1950. Prior to the study, a written permission was obtained from the Inspector General of Prisons, Bangalore as well as Superintendent of Central Jail, Gulbarga. The study considered all the convicted life-term prisoners-“convicted lifer” was defined as the one with a sentence for imprisonment for life or equated with the definite period of 14 years as recorded in register of the prison. Under trial prisoners and prisoners convicted for “short term” or “to death” were excluded from the study. Thus, we arrived at a total of 300 convicted life-term inmates eligible for inclusion in the study. All the study subjects were personally contacted examined and interviewed using predesigned and pretested proforma. This was followed by a detailed clinical examination, anthropometric measurements, and investigations. For the purpose, a pilot study was conducted on 10 subjects and proforma was finalized after incorporating the changes based on the findings of pilot study. Proforma included the items on sociodemographic and economic characteristics of the subjects. In addition, it included the detailed general physical examination and systemic examinations of the inmates. As the convicts kept in the prison under study were mostly from rural area, BG Prasad's classification modified for the latest price index was used to arrive at the socioeconomic status of the study subjects. The collection of data was done through personal interview and detailed clinical examination with investigations which was spread over a period of 1 year.
Statistical analysis
Sociodemographic characteristics of the study subjects were assessed by working out appropriate frequencies and percentages along with 95% confidence interval. The morbidities prevalent among the study subjects were classified according to “International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10).[3] Subsequently, prevalence of morbidities according to different categories of ICD-10 was estimated by working out the percentages and 95% confidence intervals for the same. Data were entered into the computer using Microsoft Excel and analyzed using statistical package SPSS 18.
RESULTS AND DISCUSSION
The present cross-sectional study was undertaken by selecting all the life-term inmates in the central prison of Gulbarga, to assess the health status of the convicted life-term inmates of central prison.
Sociodemographic characteristics
Our study found that most of the prisoners were men and the crime was more prevalent in younger age groups, although differences by age were not statistically significant. It was consistent with a study done by Bellad et al.,[4] among the inmates of central jail, Belgaum. This may be because our population is a male-dominated society; men have greater involvement in the matters outside the household. They move about in society more freely than women and therefore higher risk to commit crime in all communities and all age groups. Regarding age group, a younger person could have greater vulnerability to take deviant ways as well as greater ability to perform a crime. At this age, there may be problems like family feuds and unemployment which might have led to an increase in crime [Table 1].
Table 1.
Number (#) and proportion (%) of subjects (n=300) according to different sociodemographic characteristics and reasons for crime along with 95% confidence interval
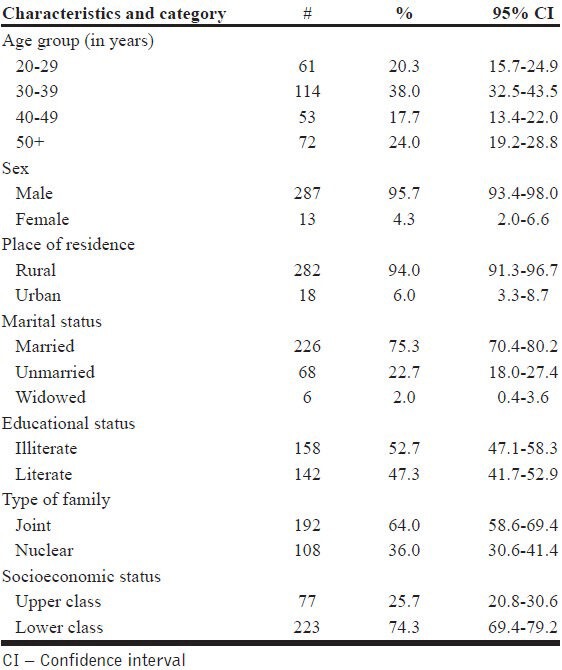
Regarding place of residence, our finding of preponderance of rural persons in jail was consistent with the study done by Aggarwal et al.,[5] in Amritsar jail. This may be attributed to more number of conflicts occurring in rural places owing to illiteracy, unemployment, and social mixing as compared to urban where people relatively confined in their own.
The study showed majority of the study subjects were married. This was comparable to the study done by Sundar et al.,[6] in central prison, Bangalore. Marriage is a crucial factor in the understanding of a person's most intimate and important interaction with life. Any sense of failure, frustration, or victimization on this front may provoke unusual behavior.
In the education of the study subjects, the majority of the inmates were illiterates followed by primary schooling and least were the graduates which are consistent with the study done by Aggarwal et al.,[5] in Amritsar jail. This may be due backwardness of the Hyderabad-Karnataka region in India. Three fourth of them were doing unskilled work. Lack of job satisfaction and low income in unskilled work might have provoked them to commit crime.
Coming to the socioeconomic status majority of the study subjects belonged to lower socioeconomic status which was consistent with a study done by Bellad et al.,[4] among the inmates of central jail, Belgaum and Sundar et al.,[6] in central prison, Bangalore. This may be due to majority of the prisoners are from rural background. Socioeconomic status reveals the functional efficacy of an individual and the presence or absence of the sense of gratification, one may derive from it. Poverty and lack of satisfaction of wants generally serve as stimulants to crime. And, majority of them belonged to joint family. This may be due to the head of the family might not have supervised the internal and external affairs of the family and also has failed to provide the economic and social security.
Health status and study population
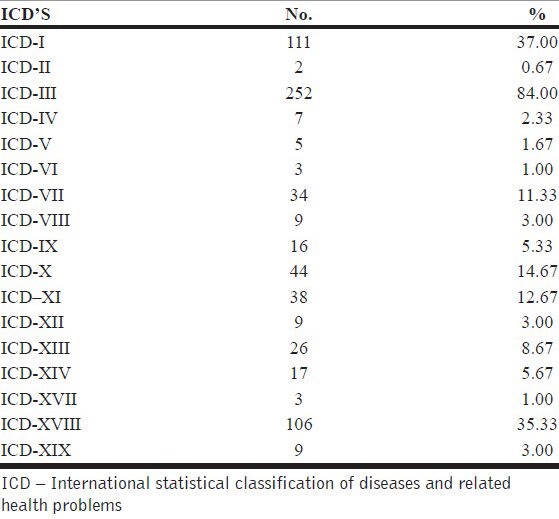
In the health status of inmates, one third were having normal health status but majority of them 191 (63.67%) were morbid. These results were comparable to a study done by Kale et al.,[7] in India showed that 90% inmates had one or more morbid conditions. The reasons for major morbidity in the present study may be prolonged contact between prisoners, inadequate chlorination of water, inadequate water supply, taking bath occasionally because of nonavailability of hot water, and so on [Table 2].
Table 2.
Distribution of the study subjects according to ICD-10 classification
ICD-I
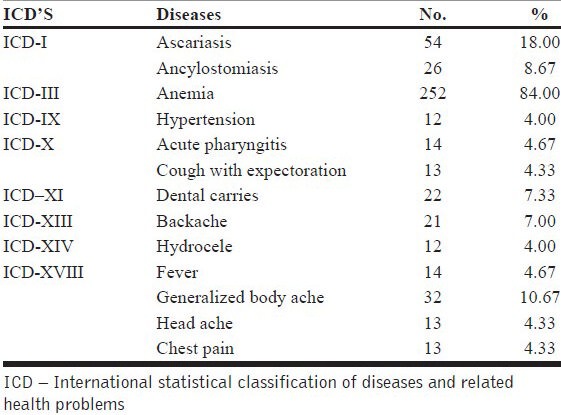
Among parasitic diseases [Table 3], majority of them suffered from ascariasis 54 (18%) and least were from teniasis 8 (2.67%). In infectious diseases, 10 (3.33%) inmates were suffered from diarrhea and pulmonary tuberculosis (TB) and 1 (0.33%) from HIV/AIDS. These results were consistent with the study done by Gupta et al.,[8] among the inmates of central prison, Yervada, Pune showed that stool of 61 inmates (26.8%) was found to be positive for ova/cyst of intestinal helminths. 36 inmates (15.8%) had ascariasis, followed by 19 (8.4%) who had ancylostomiasis and 6 (2.6%) had teniasis and TB contributed to 17 cases (7.5%). And other studies done by Bellad et al.,[4] among the inmates of central jail; Belgaum showed that 13% of the inmates suffered from diarrhea, followed by pulmonary TB and HIV contributed 2% and 1.5% respectively. Andrea et al.,[9] in San Francisco country jail has showed HIV prevalence was 1.8%. Baillargeon et al.,[10] in Texas prison showed that infectious diseases (29.6%) constituted the most prevalent major disease category among inmates. Reichard et al.,[11] in US prison showed that 14% inmates have tuberculosis and Aggarwal et al.,[5] in Amritsar jail showed HIV-1 antibodies were detected in 2.4%. The prevalence of infectious and parasitic diseases is may be due to inadequate chlorination of water, lack of sanitation, and poor personal hygiene. The prevalence of tuberculosis in the present study is high when compared with that of general population in India; this could be because of overcrowding, poor living conditions, and close contact with one another.
Table 3.
Prevalence of important sub categories of ICD-10
ICD-II, ICD-III, and ICD-IV
Our present study showed that among neoplasm 2 (0.67%) inmates showed lipoma. Among diseases of blood [Table 3], 252 (84%) inmates showed anemia and from endocrine and metabolic diseases 7 (2.33%) inmates are suffering from diabetes mellitus. These results were comparable to a study done by Bellad et al.,[4] which showed that 3.6% inmates were suffering from diabetes. And other studies done by Braatvedt et al.,[12] in Mt. Eden prison, Auckland showed that eight inmates were suffering from diabetes mellitus.
ICD-V and ICD-VI
Among mental and behavioral disorders, two (0.67%) inmates suffered from schizophrenia and three (1%) from depression, coming to the diseases of nervous system, three (1%) inmates suffering from epilepsy. These results were comparable to a study done by Alemagno et al.,[13] in Ohio jail showed that 10% reported a mental health service history in that 19% reported symptoms of schizophrenia. And other studies done by Falissard et al.,[14] in French prison showed 3.8% for schizophrenia and 17.9% major depressive disorder. Compared to Western countries, here the prevalence of mental disorders was low in our developing country like India.
ICD-VII
Our study showed that 11 (3.67%) suffered from presbyopia followed by 8 (2.67%) senile cataract and myopia, and 2 (0.67) from acute conjunctivitis. These results were comparable to a study done by Bellad et al.,[4] showed that 7% inmates had senile cataract.
ICD-VIII and ICD-IX
Among the diseases of ear and mastoid process 5 (1.67%) inmates suffered from conductive deafness and 2 (0.67%) from acute and chronic suppurative otitis media. Amongst the diseases of circulatory system [Table 3] 12 (4%) inmates had hypertension and 2 (0.67%) had varicose veins. But literature showed that Baillargeon et al.,[10] in Texas prison has showed prevalence of circulatory system diseases contributed to 14% and 9.8% cases of hypertension. And study done by Colsher et al.,[15] showed that prevalence of hypertension was 40% and myocardial infarction was 19% in elderly inmates which was very high compared to our results.
ICD-X
Among the diseases of respiratory system [Table 3] 29 (9.66%) of study population suffered from acute upper respiratory tract infection and 15 (5%) suffered from acute lower respiratory tract infection. These results were comparable to a study done by Baillargeon et al.,[10] in Texas prison has showed prevalence of diseases of respiratory system was 6.3% and 5.2% inmates suffered from asthma. Other studies done by Gupta et al.,[8] showed that 28.6% of inmates suffered from respiratory diseases among them 19 (8.4%) cases of chronic bronchitis and 22 (9.7%) cases were from acute upper respiratory tract infections. Bellad et al.,[4] showed that 21.75% inmates were suffered from acute upper respiratory tract infections revealed that respiratory infection are still a major problem in our country.
ICD-XI
Our study revealed that 22 (7.33%) of the study population suffered from dental carries [Table 3]. In the diseases of gastrointestinal system, eight (2.67%) suffered from gastritis. These results were comparable to a study done by Bellad et al.,[4] which revealed 0.93% diarrhea and 0.35% gastritis.
ICD-XII and ICD-XIII
In the diseases of skin and subcutaneous tissue, four (1.33%) suffered from pruritis ani, followed by three (1%) from tenia infection. Among the diseases of musculoskeletal system and connective tissue, 21 (7.00%) suffered from backache [Table 3] and 5 (1.67%) from rheumatoid arthritis. These results were comparable to a study done by Kuruvila et al.,[16] among the inmates of district prison, Mangalore showed that among the infectious dermatoses (63.3%) majority were fungal infections (51.3%) and pigmentary changes in 21% inmates. And other studies done by Bellad et al.,[4] showed that pyoderma was in 12% inmates. Gupta et al.,[8] showed 34.9% inmates suffered from fungal infections. Here, in our study, the skin infections are less may be due to good hygiene among inmates, less humidity, and dry weather. Baillargeon et al.,[10] in Texas prison has showed that musculoskeletal system and connective tissue diseases contributed to 15.3%, and low back pain in 5.1% inmates. Murray et al.,[17] in New South Wales prison revealed chronic health conditions like backache and arthritis. This shows lack of physical exercise and restriction of activity will lead to chronic diseases.
ICD-XIV
Our present study showed that 12 (4.00%) suffered from hydrocele [Table 3], followed by urinary tract infection and urinary calculus 2 (0.67%) and one female prisoner with fibroid uterus (0.33%). These results were comparable to the study done by Gupta et al.,[8] which revealed seven inmates were suffering from acute urethritis with overall prevalence of 3%. Here, urinary calculus cases are more because of more calcium content in water of local area and use of more dhal for food.
CONCLUSION
The population of the prisoners harbours diseases that are determined both by the environment from which they come and in prison in which they live. If the inmates are not treated adequately in jails they will return to the community further burdening the existing health care facilities of the country.
ACKNOWLEDGMENT
We thank Sri. Dharampal Negi, IPS, Additional Director General of Police (Prisons), Sri. V. S. Raja, Deputy Inspector General of Prisons, Bangalore and Sri. Sangappa, Sri. Krishna Kumar, former and current superintendents of central prison, Gulbarga and other officials of prison department for their kind support to carry out the present study in the central jail of Gulbarga. We are also thankful to the prisoners of central jail for their cooperation throughout the study.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.United States department of justice: Bureau of justice statistics. 2008. [Last accessed on july 2012]. Available from: http://www.ojp.usdoj.gov/bjs .
- 2.Prison statistics India, National Crime Records Bureau. [Last accessed on july 2012]. Available from: http://ncrb.nic.in/PSI2007/prison2007.htm .
- 3.International classification of diseases and related health problems 10th revision. [Last accessed on july 2012]. Available from: http://apps.who.int/classifications/icd10/browse/2010/en .
- 4.Bellad A, Naik V, Mallapur A. Morbidity pattern among prisoners of central jail, Hindalga, Belgaum, Karnataka. Indian J Community Med. 2007;32:307. [Google Scholar]
- 5.Aggarwal A, Arora U, Nagpal N. Seroprevalence of HIV in central jail inmates of Amritsar. Indian J Community Med. 2005;30:151. [Google Scholar]
- 6.Sundar M, Ravikumar KK, Sudarshan MK. A cross sectional seroprevalence survey for HIV 1 and high risk sexual behavior of seropositives in a prison in India. Indian J Public Health. 1995;39:116–8. [PubMed] [Google Scholar]
- 7.Kale KM, Jogdand GS, Aswar NR. Sociomedical problems of institutionalised women. Indian J Med Sci. 1999;53:162–6. [PubMed] [Google Scholar]
- 8.Gupta RK, Singh GPI, Gupta RR. Health status of inmates of a prison. Indian J Community Med. 2001;26:86–9. [Google Scholar]
- 9.Kim AA, Martinez AN, Klausner JD, Goldenson J, Kent C, Liska S, et al. Use of sentinel surveillance and geographic information systems to monitor trends in HIV prevalence, incidence, and related risk behavior among women undergoing syphilis screening in a jail setting. J Urban Health. 2008;86:79–92. doi: 10.1007/s11524-008-9307-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Baillargeon J, Black SA, Pulvino J, Dunn K. The disease profile of Texas prison inmates. Ann Epidemiol. 2000;10:74–80. doi: 10.1016/s1047-2797(99)00033-2. [DOI] [PubMed] [Google Scholar]
- 11.Reichard AA, Lobato MN, Roberts CA, Bazerman LB, Hammett TM. Assessment of tuberculosis screening and management practices of large jail systems. Public Health Rep. 2003;118:500–7. doi: 10.1016/S0033-3549(04)50286-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Braatvedt G, Rowan J, Atherfold C. A cross-sectional study of diabetes in Mt Eden Prison, Auckland. N Z Med J. 1994;107:292–3. [PubMed] [Google Scholar]
- 13.Alemagno SA, Wolfe SA, Pace RB, Shobert RL, Butts JM. Managed public health in a county jail. Am J Public Health. 1998;88:1265. doi: 10.2105/ajph.88.8.1265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Falissard B, Loze JY, Gasquet I, Duburc A, de Beaurepaire C, Fagnani F, et al. Prevalence of mental disorders in French prisons for men. BMC Psychiatry. 2006;6:33. doi: 10.1186/1471-244X-6-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Colsher PL, Wallace RB, Loeffelholz PL, Sales M. Health status of older male prisoners: A comprehensive survey. Am J Public Health. 1992;82:881–4. doi: 10.2105/ajph.82.6.881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kuruvila M, Ismail SM, Pramod K. Pattern of dermatoses among inmates of district prison-Mangalore. Indian J Dermatol. 2002;68:16–8. [PubMed] [Google Scholar]
- 17.Murray N, LePage E, Butler T. Hearing health of New South Wales prison inmates. Aust N Z J Public Health. 2004;28:537–41. doi: 10.1111/j.1467-842x.2004.tb00043.x. [DOI] [PubMed] [Google Scholar]