

Abstract
Background:
The available information regarding the obesity pattern of the undergraduate female students of Kolkata is inadequate, though there are several reports which indicate the complications and/or awful consequences of obesity on female health particularly, during the reproductive years.
Aim:
The present investigation has thus been carried out to report their present physiological status along with the prevalence of obesity, based on their body mass index (BMI), some direct and derived anthropometric indices, and physical fitness.
Subjects and Methods:
This small-scale cross-sectional study conducted in randomly selected 100 female students of different colleges of Kolkata with the age of 18-22 [mean age 20.4 (2.3)] years. Measurements of body composition included total 24 variables, with thirteen direct and eleven derived anthropometric variables; while physical efficiency parameters were physical fitness index, VO2max, energy expenditure and anaerobic power. The data of the experimental group were compared with those of the control group by t-test, using SPSS v.15.0 and MS-Excel v.2013.
Results:
Analysis of collected data showed majority of the students have normal range of BMI (67.95%), but, 21.95% of students found to be overweight and 3.84% are obese. They also showed higher fat mass [14.40 (4.11)], but, lower waist-to-hip ratio and conicity index. They were found to have poor to moderate physical fitness [57.60 (3.90)] and higher energy expenditure [5.61 (0.72)].
Conclusion:
The findings of the present obesity screening reports almost one of four female students (24 out of 100 participants) are overweight/obese, indicated higher body fat distribution and increased propensity of being obese with age. Thus, the overall data along with their low physical fitness points out to health risks among female undergraduates of Kolkata.
Keywords: Anthropometry, Blood pressure, Body mass index, Conicity index, Obesity, Physical fitness, Waist-to-hip ratio
Introduction
In 2009, 26% of US adult women reported a body mass index (BMI) in the obese range (≥ 30 kg/m2).[1] With rates of both adult and adolescent obesity increasing, the prevalence of obesity among women of childbearing age (aged 15-44 years) can also be expected to increase. Screening for obesity in women of reproductive age remains understudied. There are data that support the basic tenets of screening for obesity in women during reproductive years. Obesity is a disease with measurable public-health impact during the reproductive years, not just later in life.
Screening for obesity by calculating BMI is a reproducible, simple, and inexpensive technique that reliably estimates adiposity without the time and expense of less practical methods.[2] Along with BMI, anthropometric data are reliable to assess the physical status of a population.[3] Jung and Jung surveyed different dimensions and characteristics of different populations and found that age, gender, and ethnic characters were determinants of physical dimensions. It is more common in adults than in children and in females than in males.[4] There are many anthropometric indicators in use, such as mid-upper arm circumference (MUAC), BMI of Quetlet.[5] Body composition along with morphometric characters are useful measure of nutritional status of a population. Typically the composition of human body is assessed to determine percentage of body fat (PBF). However, it is now clear that in addition to the amount of fat in the body, its topography particularly the abdominal fat deposition is considered to be the most atherogenic, diabetogenic and hypertensiogenic fat deposition of the human body.[6] The three most commonly used measures of abdominal or central adiposity are waist circumference (WC), waist-to-hip ratio (WHR), and BMI. These parameters have been utilized in recent investigations to study abdominal or central adiposity.[7,8] Recent studies have also reported that central as well as subcutaneous adiposity is associated with body composition measures like PBF and fat mass (FM).[9,10]
Nutritional problems, especially obesity in women can result in reduced productivity, slow recovery from illnesses, increased susceptibility to infections, and a heightened risk of adverse pregnancy outcomes. A woman's nutritional status has important implications for her health as well as the health of her children. A woman with poor nutritional status, as indicated by a low BMI, short stature, or other micronutrient deficiencies, has also a greater risk of obstructed labour, having adverse pregnancy outcomes, producing lower quality breast milk, death due to postpartum haemorrhage. Malnutrition among women has long been recognized as a serious problem in India; but national-level data on levels and causes of malnutrition have been scarce,[11] especially, information regarding the obesity pattern among the undergraduate female students. Thus, the present investigation has been carried out to screen the obesity pattern in the female undergraduates of Kolkata.
As cohort studies, ideal for nutritional conditioning monitoring, suffer, in third world countries, from the logistic difficulties usually associated with population studies of large magnitude, less expensive cross-sectional studies can provide relevant element for understanding the connection between health status and physical condition of life,[12] the present investigation was designed as a small-scale cross-sectional study to investigate the relationship of various physical efficiency and anthropometric measures with body composition variables among college students of Kolkata, India.
Subjects and Methods
Participants
In this cross-sectional cohort study (carried out during July, 2011-March, 2012) female (n = 100) subjects between 18 years and 22 years of age were randomly selected to participate in the present study (SPSS v.15.0 and MS-Excel v.2013). Subjects are undergraduate students of different colleges of Kolkata. The entire experimental protocol was explained to them to allay their apprehension. Consent from each participant was taken for conducting the study and the experiments were carried out following Institutional ethical permission. Subjects were instructed to take their last meal at least 2 h before conducting the test in order to avoid the specific dynamic action of food. All the experiments were carried out and measurements were taken in temperature of 20-25°C and relative humidity of about 45-50% in winter season in India, to avoid seasonal influence on fitness pattern. To minimize the experimenter bias each measurement was taken for 3 times and the mean was represented as final result. Subjects with any type of disease, specially cardiac and respiratory ailments were not taken for experiments, only healthy subjects are considered for each experiment. Each subject was given sufficient rest before each experiment to get accurate result.
Measurement of physical parameters
The BMI of Quetelet is the statistical measure, which compares a person's weight and height by the following formula: BMI = mass (kg)/height in (m2).[13] The WHO regard a BMI of less than 18.5 as underweight and may indicate malnutrition, an eating disorder, or other health problems, while a BMI greater than 25 is considered overweight and above 30 is considered obese.[14]
Body fat can be estimated from the BMI. There is a linear relationship between densitometrically-determined PBF and BMI, taking age and gender into account. Based on which following prediction formulas have been derived, which showed a valid estimate of the body fat at all ages, in males and females. However, in obese subjects the prediction formulas are slightly overestimated. The prediction error is comparable with other methods of estimating body fat percentage, such as skinfold thickness measurements or bioelectrical impedance.[15,16] The following formula to predict body fat percentage is based on current BMI, age, and gender: PBF = (1.20 × BMI) + (0.23 × Age) − 5.4 [for females].
Body surface area (BSA) is the measured or calculated surface of a body. Various calculations have been published to arrive at the BSA without direct measurement. Dubois and Dubois formula was used for estimating body surface BSA.[17]
Anthropometry
A total of 24 metric measurements were taken for each subject including direct and derived anthropometric and physiological variables. The anthropometric measurements taken for each subject were: Height, weight, eye height standing, elbow rest height standing, abdominal extension, sitting height, knee height, buttock-to-knee length, five circumferences i.e., MUAC, thigh, calf, waist, and hip (BC). However, in the present communication, thirteen directly measured variables and eleven derived variables: BSA, BMI, body adiposity index (BAI), FM, fat mass index (FMI), fat free mass (FFM), fat free mass index, waist-to-height ratio, WHR, MUAC-to-height ratio and conicity index (C-index) were included. All anthropometric measurements were made by using standard anthropometric techniques as proposed by Lohman et al.[18] All the derived variables were computed using standard equations.[19]
Resting on heart rate (HR) and blood pressure (BP)
Baseline HR was obtained after 5 min rest in the sitting position. The resting heart beat was measured at the carotid pulse. When two successive HR scores become equal then it was considered as resting HR.[20] Arterial pressures are most commonly measured by a sphygmomanometer, which historically used the height of a column of mercury to reflect the circulating pressure.[21] BP values were obtained after 5 min rest in the sitting position.[22]
Physical fitness index (PFI)
PFI was calculated by measuring HR after performing Harvard's step test (HST) developed by Brouha et al.[23] in the Harvard Fatigue Laboratories using long form PFI equation. However, following modified HST under Indian condition, using a stool of 51 cm high stepping up and down, with a rate of 30 cycles/min, for 3 min or up to exhaustion. Exhaustion is defined as when the subject cannot maintain the stepping rate for 15 s.[24] The recovery pulse was counted at 1-1.5, 2-2.5 and 3-3.5 min of recovery. Long Form Equation-Fitness index = [100 × test duration in seconds]/[2 × recovery HRs (1-1.5 min + 2-2.5 min + 3-3.5 min)]. The cut-off values of PFI are: Very poor (<50), poor (50-60), fair (60-70), and good (70-80) and excellent (>80).[23]
Anerobic power test by margaria double step method
It is a short-term anaerobic test or power test in which the subject taking two steps at a time; the heights of the stairs are measured by measuring tape. To calculate the anaerobic power; the height of ascend, the body weight, and the duration (s) is noted by the stopwatch.[25] At first the work done is calculated by the following formulae: Work done = body weight × height of ascend × 0.002342. From the calculated work done, the anaerobic power is obtained by the formulae: Anaerobic power = [work done (kg/m)/duration (s)].
Determination of aerobic capacity (VO2max)
Nomogram of Astrand was used to determinate the VO2max.[26] Participants maximum (peak) HR, as obtained from HST, was used to determine the aerobic capacity.
Statistical analysis
To carry out the analysis of the data statistically SPSS v.15.0 and MS-Excel v.2013 were used. Results were expressed as mean (standard deviation). If differences between groups were established, the values of the treated groups were compared with those of the control group by a modified t-test. A value of P < 0.05 was interpreted as statistically significant.[27]
Results
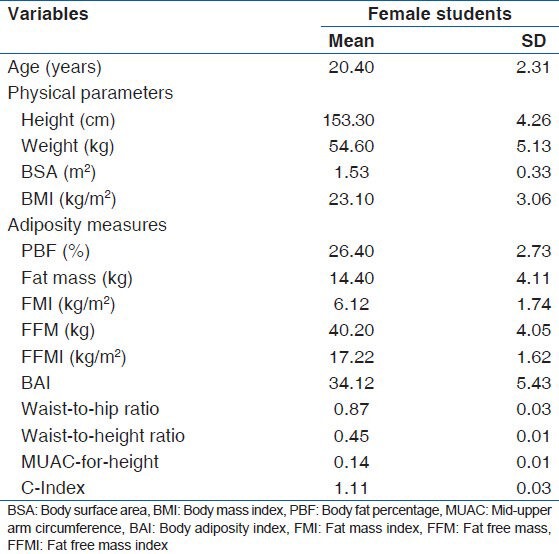
The direct and derived anthropometric parameters that indicate the prevalence of obesity of the studied population based on PBF, WC and WHR are presented in Table 1. It also represents comparative aspects of physical variables (BSA and BMI). The results though indicate moderate body weight with respect to their height in female students (according to WHO weight-to-height tables), but, the fat distribution in quite higher in females that of the cut-off values. The cut-off points of obesity were adopted as recommended by Dudeja et al.[28] of PBF (≥ 30.0%), Dasgupta and Hazra[29] for WC (≥ 72.0 cm), and Rahim et al.[30] for WHR (≥0.85). PBF (though < 30.0%), FM, FMI and BAI are higher in female students, which indicate increased inclination towards obesity.
Table 1.
Derived anthropometric variables of female (n=100) college students for screening body composition and obesity
The frequency of overweight and underweight students is presented in Table 2. The overall prevalence of obesity (BMI > 30.00) was almost absent in the studied sample, only 3.84% of the studied population showed obesity. However, the frequency of overweight (BMI 25.0-29.9) was higher in undergraduate females of Kolkata (total of 21.95%). However, most of the student populations are found to have normal range of body weight, as found on the basis of BMI. Among 100 students, 67.95% of students showed normal BMI. Here, it should be mentioned that all these estimations are based on an indirect technique, i.e., anthropometry and International Classification of BMI cut-off points.[14]
Table 2.
Prevalence of obesity based on body mass index: Undergraduate female college students of Kolkata (n=100)

Table 3 represents some common physical fitness variables of female students. They showed poor physical fitness (i.e., between the cut-off value 50 and 60). But, in all other parameters they fit in normal range.
Table 3.
Physiological parameters indicating physical fitness and endurance of female students
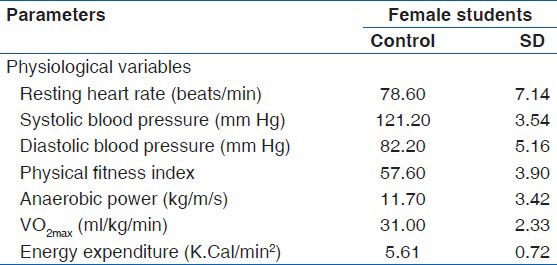
Figure 1 describes some common anthropometric measures of female college students; of these parameters also indicate the tendency towards obesity. Results show that female students have lower stature, eye height, acromial height, elbow rest height, abdominal extension, and mean upper arm, thigh and WCs than the Indian standard values.[31] Lower WC and abdominal extension reflects lower abdominal fat distribution in females, which has again reflected in WHR.
Figure 1.
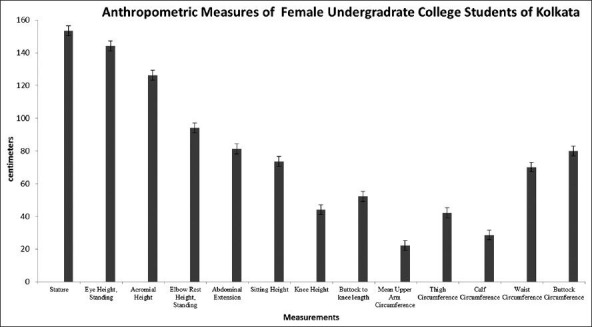
Direct anthropometric indices of female (n = 100) college students
Discussion
BMI is considered as a better index for assessing obesity, because it does away with the need of height-weight tables and is independent of type of obesity frame and it can be used to estimate the prevalence of obesity within a population.[32] Therefore, in the present study, the body composition of undergraduate college students was calculated according to critical limits of BMI as recommended by WHO.[32] Table 1 shows various physical parameters and obesity indicators, among which female students have showed lower BSA due to their lower stature. They also showed higher PBF, FM, FMI and BAI, than the cut-off values, which are indicators of their overall higher fat distribution. Conversely, they showed significantly lower FFM and C-index, which showed lower abdominal fat and muscle mass distribution. These results indicate higher overall fat distribution in females, but, they have lower fat distribution in their abdominal regions.
Table 2 presents the distribution of all subjects according to BMI classification. Only 4% of the participants are reported to be underweight. Though, it was observed that most of the subjects have normal BMI (total of 67.95%), but, the results indicated higher propensity of being obese was observed in females. Among undergraduate female students, 21.95% were overweight (24.9-29.9). The results of female students also indicated an important aspect, that when they are getting aged, they are getting more weight than their young age, which has been reflected in age wise BMI distribution of students [Table 2]. In this present study it has been found that the females in the age group of 20-22 years have higher frequency of overweight students (69.23%) than those in the 18-20 years age group (66.67%). It has already been found in earlier studies that when the Bengali/Hindu females of Kolkata, getting aged, they gain more weight and becomes obese. They rank third in the prevalence of obesity in India, after Uttar Pradesh and Jammu and Kashmir.[33] While comparing the present data with the other populations of India, it is apparent that the prevalence rate of overweight/obesity in the present study is in line with other Indian studies which have also shown a high prevalence of overweight and obesity. Gopinath et al.[34] studied urban women of Delhi and reported the prevalence rate of obesity as 33.4%. Visweswara Rao et al.[35] studied females belonging to high socio-economic status of Hyderabad and reported the prevalence rate of obesity as 36.3%. The nutrition Foundation of India has just completed a study on the prevalence of obesity in urban Delhi, and has reported the prevalence rate of overweight (BMI 25+) and obesity (BMI > 30) as 50% and 14% respectively.[36]
Overweight and obesity has been found to be associated with many disease particularly heart disease, type-2 diabetes and osteoarthritis.[37] The prevention and control of this problem must, therefore, claim priority attention.
Cardiorespiratory fitness is a measure of how well a physiological system is capable of transport oxygen to muscles during prolonged exercise. Resting HR and aerobic capacity (VO2max) has been extensively considered to be a reliable and valid measure of cardiopulmonary or aerobic fitness.[38] Energy required by muscle for physical movement normally is originated through aerobic metabolism. Therefore, workload could be measured through calculation of VO2max. Undergraduate students of Kolkata showed normal range of VO2max. However, Bailey et al.[39] have reported that lower VO2max levels are associated with an increased probability of being overweight/obese. Strength exercise increases ventricular muscle mass,[5] which results in increased force of contraction and hence cardiac output, but, in this study, a normal range of systolic BP was observed among female college students. While measuring physical fitness, their pulse rate recovered quite slowly; this is an indicator of poor fitness, and thus, reflected in PFI. They showed normal range of energy expenditure and anaerobic power [Table 3]. PFI scores are useful measures of fitness for strenuous exercises. Physical fitness has three main aspects: Static fitness (absence of disease), dynamic fitness (ability to perform strenuous work) and motor skills fitness. Of this three, dynamic fitness is very important and can be measured by HST.[40]
Morphometric analysis of the body is virtually the investigation of the process of life which reflects the general health status of an individual.[41] In this present study, lower stature, eye height, acromial height, elbow rest height, abdominal extension, and mean upper arm, thigh and WCs were found in female students than Indian standard values.[31] MUAC, which is an estimate of energy store and protein mass of the body and an indirect estimate of strength,[42] is found to be lower in female students. Lower WC and abdominal extension reflects lower abdominal fat distribution in females, which has again reflected in WHR. Among WC and WHR, WC is considered to be a better index for fat location than WHR for predicting lipid profile in adult women.[40] However, it is a well-known fact that BMI also has a negative correlation with WHR, as reflected in our study, which is very much important in case of women, because, this interrelation is a cue to the female physical attractiveness and beauty of women.[43,44,45,46]
Conclusion
Overall findings of the present obesity screening report describes that almost one of four female students (24 out of 100 participants) are overweight/obese, and indicated higher body fat distribution and increased propensity of being obese with age. Therefore, appropriate precautionary measures to be taken to prevent further progression of the problem into the young population. Because if the present trends of overweight/obesity continues, the situation can get worse even single most important public health problem in adults.
Acknowledgments
We are sincerely thankful to the Principal, Vidyasagar College for Women, University of Calcutta for providing support to the authors for this work. They also gratified to other Teachers and Staffs of Department of Physiology, Vidyasagar College for Women and obvious credit goes to B.Sc. Final Year Physiology Honors students (2011-2012).
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Centers for Disease Control and Prevention (CDC). Vital signs: State-specific obesity prevalence among adults – United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59:951–5. [PubMed] [Google Scholar]
- 2.Oken E, Gillman MW. Fetal origins of obesity. Obes Res. 2003;11:496–506. doi: 10.1038/oby.2003.69. [DOI] [PubMed] [Google Scholar]
- 3.Chandra AK, Sengupta P, Goswami H, Sarkar M. Excessive dietary calcium in the disruption of structural and functional status of adult male reproductive system in rat with possible mechanism. Mol Cell Biochem. 2012;364:181–91. doi: 10.1007/s11010-011-1217-3. [DOI] [PubMed] [Google Scholar]
- 4.Jung SH, Jung SH. Surveying dimensions and characteristics of Korean ears for the ergonomic design of ear-related products. Int J Indus Erg. 2003;31:361–73. [Google Scholar]
- 5.Sengupta P. Assessment of physical fitness status of young sikkimese residing in high-hill temperate regions of Eastern Sikkim. Asian J Med Sci. 2011;2:169–74. [Google Scholar]
- 6.Kopelman PG. Obesity as a medical problem. Nature. 2000;404:635–43. doi: 10.1038/35007508. [DOI] [PubMed] [Google Scholar]
- 7.Ghosh A, Chatterjee D, Bandyopadhyay AR, Das Chaudhuri AB. Age and sex variation of body mass index and waist circumference among the Santal children of Jharkhand, India. Anthropol Anz. 2006;64:83–89. [PubMed] [Google Scholar]
- 8.Sengupta P, Chaudhuri P, Bhattacharya K. A small-scale cross-sectional study for the assessment of cardiorespiratory fitness in relation to body composition and morphometric characters in fishermen of Araku valley, Andhra Pradesh, India. Int J Prev Med. [In Press] [PMC free article] [PubMed] [Google Scholar]
- 9.Sengupta P. Environmental and occupational exposure of metals and their role in male reproductive functions. Drug Chem Toxicol. 2013;36:353–68. doi: 10.3109/01480545.2012.710631. [DOI] [PubMed] [Google Scholar]
- 10.Bose K, Ghosh A, Das Chaudhuri AB. Relationship between anthropometric measures and body composition among Bengalee female university students of Kolkata. J Ind Anthrop Soc. 2003;38:89–94. [Google Scholar]
- 11.Behrman RE, Kliegman RM, Jenson HB. Nelson's Textbook of Paediatrics. 16th ed. Philadelphia: Saunders; 2000. The field of Pediatrics; pp. 32–50. [Google Scholar]
- 12.Das S, Chowdhury T, Bose K. Age variations in anthropometric and body composition characteristics among adult Bauri females of Paschim Medinipur, West Bengal, India. Scholarly J Sci Res Essay. 2012;1:16–24. [Google Scholar]
- 13.Eknoyan G. Adolphe Quetelet (1796-1874) – The average man and indices of obesity. Nephrol Dial Transplant. 2008;23:47–51. doi: 10.1093/ndt/gfm517. [DOI] [PubMed] [Google Scholar]
- 14.World Health Organization. Global Database on Body Mass Index. BMI Classification. World Health Organization website. 2000. [Last cited 2011 Apr 26]. Available from: http://www.apps.who.int/bmi/index.jsp?introPage=intro_3.html .
- 15.Deurenberg P, Weststrate JA, Seidell JC. Body mass index as a measure of body fatness: Age- and sex-specific prediction formulas. Br J Nutr. 1991;65:105–14. doi: 10.1079/bjn19910073. [DOI] [PubMed] [Google Scholar]
- 16.Sengupta P, Chaudhuri P, Bhattacharya K. Male reproductive health and yoga. Int J Yoga. 2013;6:87–95. doi: 10.4103/0973-6131.113391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.DuBois D, DuBois EF. A formula to estimate the approximate surface area if height and weight be known. Arch Int Med. 1916;17:863. [Google Scholar]
- 18.Lohman TG, Roche AF, Martorell R. Chicago: Human Kinetics Books; 1988. Anthropometric standardization reference manual; pp. 55–69. [Google Scholar]
- 19.Geneva: World Health Organization; 1995. World Health Organization. Physical status: The use and interpretation of anthropometry. Report of the WHO Expert Committee, Technical Report Series, No. 854; p. 460. [PubMed] [Google Scholar]
- 20.Krajewska-Kulak E, Sengupta P. Thyroid function in male infertility. Front Endocrinol. 2013;4:1–2. doi: 10.3389/fendo.2013.00174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Booth J. A short history of blood pressure measurement. Proc R Soc Med. 1977;70:793–9. [PMC free article] [PubMed] [Google Scholar]
- 22.Chatterjee CC. Kolkata, India: Medical Allied Agency; 1985. Measurement of blood pressure. Human Physiology; pp. 299–312. [Google Scholar]
- 23.Brouha I, Health CW, Gray B. A step test simple method of measuring physical fitness for hard muscular work in adult men. Rev Can Biol. 1943;2:86. [Google Scholar]
- 24.Ryhming I. A modified Harvard step test for the evaluation of physical fitness. Arbeitsphysiologie. 1953;15:235–50. doi: 10.1007/BF00933320. [DOI] [PubMed] [Google Scholar]
- 25.Margaria R, Aghemo P, Rovelli E. Measurement of muscular power (anaerobic) in man. J Appl Physiol. 1966;21:1662–4. doi: 10.1152/jappl.1966.21.5.1662. [DOI] [PubMed] [Google Scholar]
- 26.Astrand PO, Rodahl K, Dahl H, Stromme S. Test Book of Work Physiology. 4th ed. McGraw Hill: United States; 1960. Evaluation of physical performance on the basis of tests; p. 281. [Google Scholar]
- 27.Das D, Das A. Statistics in Biology and Psychology. 4th ed. Calcutta: Academic Publishers; 2005. Testing of Hypothesis; pp. 123–42. [Google Scholar]
- 28.Dudeja V, Misra A, Pandey RM, Devina G, Kumar G, Vikram NK. BMI does not accurately predict overweight in Asian Indians in northern India. Br J Nutr. 2001;86:105–12. doi: 10.1079/bjn2001382. [DOI] [PubMed] [Google Scholar]
- 29.Dasgupta S, Hazra SC. The utility of waist circumference in assessment of obesity. Indian J Public Health. 1999;43:132–5. [PubMed] [Google Scholar]
- 30.Rahim AHF, Abu-Rmeileh NM, Husseini A, Ottensen GO, Jervell J, Bjertness E. Obesity and selected co-morbidities in an urban Palestine population. Int J Obs Rel Met Dis. 2001;25:1736–40. doi: 10.1038/sj.ijo.0801799. [DOI] [PubMed] [Google Scholar]
- 31.Roy JS. Cambridge Studies in Biological and Evolutionary Anthropology. Cambridge: University Press; 1991. Epidemiological indices, anthropometric and cadaver estimates of body composition. Body Composition In Biological Anthropology; pp. 24–5. [Google Scholar]
- 32.Geneva: World Health Organization; 1998. World Health Organization. Obesity: Preventing and managing the global epidemic. Report of the WHO Consultation on Obesity, Technical Report Series, No. 894; pp. 1–3. [PubMed] [Google Scholar]
- 33.Zargar AH, Masoodi SR, Laway BA, Khan AK, Wani AI, Bashir MI, et al. Prevalence of obesity in adults: An epidemiological study from Kashmir Valley of Indian Subcontinent. J Assoc Physicians India. 2000;48:1170–4. [PubMed] [Google Scholar]
- 34.Gopinath N, Chadha SL, Sood AK, Shekhawat S, Bindra SP, Tandon R. Epidemiological study of hypertension in young (15-24 yr) Delhi urban population. Indian J Med Res. 1994;99:32–7. [PubMed] [Google Scholar]
- 35.Visweswara Rao K, Balakriskhna N, Shatrugna V. Variations if forms of malnutrition in well-to-do adults and the associated factors. Man in India. 1995;75:241–9. [Google Scholar]
- 36.Gopalan C. Obesity in the Indian urban middle class. NFI Bulletin. 1998;19:19. [Google Scholar]
- 37.Haslam DW, James WP. Obesity. Lancet. 2005;366:1197–209. doi: 10.1016/S0140-6736(05)67483-1. [DOI] [PubMed] [Google Scholar]
- 38.Sengupta P, Chaudhuri P, Biswas S, Haldar RP. An evaluation of the effect of emerging trend of gym-going over physical and physiological fitness. Intern Conference Molecules Systems Physiol. 2011;1:113–4. [Google Scholar]
- 39.Bailey DM, Davies B, Young IS, Jackson MJ, Davison GW, Isaacson R, et al. EPR spectroscopic detection of free radical outflow from an isolated muscle bed in exercising humans. J Appl Physiol. 2003;94:1714–8. doi: 10.1152/japplphysiol.01024.2002. [DOI] [PubMed] [Google Scholar]
- 40.Sengupta P. The laboratory rat: Relating its age with humans. Int J Prev Med. 2013;4:624–30. [PMC free article] [PubMed] [Google Scholar]
- 41.Chandra A, Sengupta P, Goswami H, Sarkar M. Effects of dietary magnesium on testicular histology, steroidogenesis, spermatogenesis and oxidative stress markers in adult rats. Ind J Exp Biol. 2013;51:37–47. [PubMed] [Google Scholar]
- 42.Chandra AK, Goswami H, Sengupta P. Dietary calcium induced cytological and biochemical changes in thyroid. Environ Toxicol Pharmacol. 2012;34:454–65. doi: 10.1016/j.etap.2012.06.003. [DOI] [PubMed] [Google Scholar]
- 43.Sengupta P. Potential health impacts of hard water. Int J Prev Med. 2013;4:866–75. [PMC free article] [PubMed] [Google Scholar]
- 44.Dutta S, Joshi KR, Sengupta P, Bhattacharya K. Unilateral and bilateral cryptorchidism and its effect on the testicular morphology, histology, accessory sex organs and sperm count in laboratory mice. J Hum Repro Sci. 2013;6:106–10. doi: 10.4103/0974-1208.117172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sengupta P, Sahoo S. A cross sectional study to evaluate the fitness pattern among the young fishermen of coastal Orissa. Indian J Pub Health Res Dev. 2013;4:171–5. [Google Scholar]
- 46.Sengupta P. Challenge of infertility: How protective the yoga therapy is? Ancient Sci Life. 2012;32:61–2. doi: 10.4103/0257-7941.113796. [DOI] [PMC free article] [PubMed] [Google Scholar]