

Abstract
Background:
Stress fractures of the naviculum bone are uncommon injuries occurring predominantly in athletes. These fractures are usually treated nonoperatively with a nonweight bearing cast for a minimum of 6 weeks followed by rehabilitation. Further, there is a paucity of literature on the long term clinical followup of these patients. These fractures do not heal predictably with conservative management, which does not inspire great compliance and their clinical outcome is variable. We report on the outcome of these fractures following early operative intervention by minimally invasive fixation and early weight bearing and rehabilitation. We propose that this is reliable and a successful treatment regimen and its role as the definitive management of this clinical problem should be explored.
Materials and Methods:
Nine athletes with ten stress fractures of the navicular treated at our institution between April 1991 and October 2000. The mean age of the patients was 22.8 years (range 18-50 years). All patients were treated by minimally invasive screw fixation and early weight bearing mobilization without a cast. The average followup was 7 years (range 2-11 years).
Results:
Seven of the nine patients returned to their pre-fracture level of sporting activity at an average of 5 months (range 3-9 months). One patient returned to full sporting activity following a delay of 2 years due to an associated tibial stress fracture and one patient had an unsatisfactory result. Long term review at an average of 7 years showed that six of these eight patients who returned to sports remained symptom free with two patients experiencing minimal intermittent discomfort after prolonged activity.
Conclusions:
We recommend percutaneous screw fixation as a reliable, low morbidity procedure allowing early return to full sporting activity without long term complications or recurrences.
Keywords: Minimally invasive surgery, naviculum, stress fracture
INTRODUCTION
Navicular stress fractures have been identified as a cause of high morbidity especially in elite athletes for the past 20 years. Originally, this fracture was thought to be rare, but recent studies reveal an incidence of 14-35% of all stress fractures diagnosed.[1,2,3] It is particularly common in elite athletes with track athletes accounting for 59% of all naviculum stress fractures.[1] Further, a recent review showed that the majority of stress fractures are mismanaged, probably due to poor compliance, when a conservative approach is taken and the result in these cases is less than acceptable.[2]
Biomechanical analysis of motion of the naviculum bone during the gait cycle reveals that the majority of force is directed at the central third of the bone.[1,2,3] Microangiographic studies of cadaveric feet revealed that this central third of the naviculum bone is an area of relative avascularity.[4,5] These two factors predispose the central third of the proximal articular surface of the tarsal naviculum bone to be the most common site for stress fractures [Figure 1].
Figure 1.

Stress fracture of the naviculum seen on plain X-ray. (White arrow)
The literature currently indicates two schools of thought on the management of these problematic fractures. Torg et al.[6] recommended nonoperative management with 6 weeks of nonweight bearing in a cast followed by 6 weeks of graduated physical therapy and rehabilitation. This view was supported by Khan et al.[7] These are short term studies and do not identify the risk of recurrence on return to the same high demand activities that resulted in the fracture in the first place or the duration and medium term success of return to such activities or indeed whether the athletes fully returned to the same very high demand level as before. Six weeks of immobilization in a cast followed by a prolonged period of rehabilitation results in significant physical as well as psychological morbidity and delays their return to active sport. Fitch et al.[8] recommended autogenous cancellous bone grafting and non-weight bearing for 3-4 weeks with 80% (12/15) success in return to pre-injury level of sport.
We propose a management protocol involving minimally invasive percutaneous screw fixation under radiological control, followed by early mobilization including immediate weight bearing and a graduated rehabilitation program.
MATERIALS AND METHODS
Nine patients with 10 stress fractures of the naviculum were identified from the hospital records [Table 1]. Data were gathered from a computer register maintained at this hospital, of all naviculum stress fractures operated by a single surgeon between January 1991 and July 2000.
Table 1.
Patient demographics
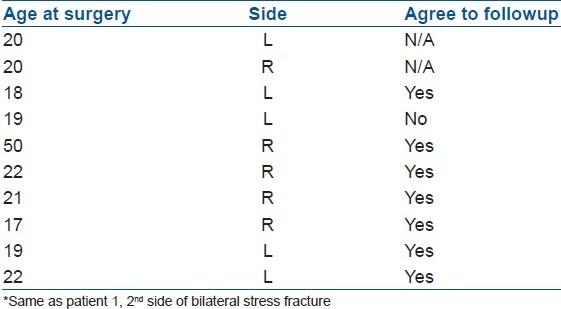
After undergoing detailed physical examination, all patients underwent X-ray examination, bone scanning and tomographic imaging (CT). Nine athletes were identified with sagittal plane naviculum stress fractures, including 4 track and field athletes, 3 Australian rules footballers, a hockey player and a basketball player. Eight were male and one was female. Four fractures were on the right, 4 on the left and one was bilateral. The average age of the patients was 22.5 years (range 17-52 years).
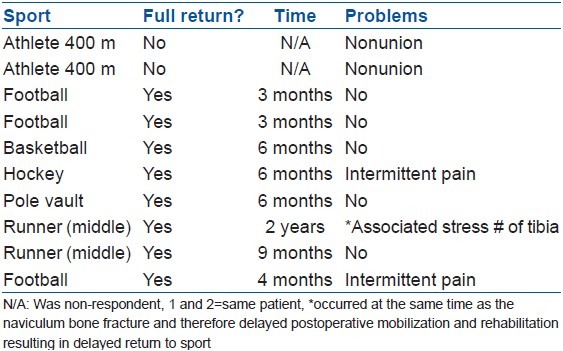
It is evident that seven of the nine athletes were able to resume active sports including competition at an average of 7.6 months after surgery [Table 2], with one outlier taking 24 months. The delay in this case was due to a co-existing tibial stress fracture. Only two out of nine patients had residual pain at followup, which was low grade and intermittent. Only one patient had a nonunion. The average time from onset of symptoms until surgical fixation was 18 weeks (range 6-41 weeks).
Table 2.
Athlete and return to function
Radiological assessment consisted of weight bearing anteroposterior, lateral and oblique views of the foot, a radionucleotide bone scan and if this showed increased activity in the naviculum, a CT scan focusing on the naviculum bone was performed. All had positive bone scans with CT confirming the diagnosis. Seven scans showed partial fractures coursing from the central third of the proximal dorsal cortex and four having propagation into the distal cortex.
All patients underwent the same procedure performed by a single surgeon. This involved minimally invasive percutaneous fixation using a single small-fragment Arbeitsgemeinschaft für osteosynthesefragen (AO) screw
AO/Synthes (Solothurn, Switzerland and West Chester, PA, USA) under image intensifier radiological control [Figure 2].
Figure 2.

Plain X-ray anteroposterior view of midfoot showing navicular stress fracture fixed percutaneously with a lag screw
Postoperative protocols were standardized and supervised. No cast was applied postoperatively. Patients were allowed immediate postoperative ambulation with weight bearing as tolerated and early return to quiet walking within limits of pain. No calf exercises, running or forefoot loading activities were allowed for the first 6 weeks. Cycling and stepper were allowed from 6 weeks to 3 months and return to running, progressing to active sports and training were allowed after 3 months, subject to good clinical progress.
Patients were contacted either by phone or mail and requested to participate in the review. Seven patients agreed, one refused (the case of bilateral fractures with failed treatment) and one was not contactable. All patients were followed up with a standardized questionnaire as well as CT scan to assess fracture union [Figure 3].
Figure 3.

Computed tomography scan at followup showing radiological evidence of union
RESULTS
This was a cohort study with baseline data extracted by chart review and followup by imaging and postal questionnaire. Followup ranged from 2 years to 11 years with a mean followup of 7 years. The average time to clinical and radiological union was 9 weeks (range 7-15 weeks). All athletes with isolated fractures achieved pre-injury levels of performance at an average of 21 weeks post-surgery (range 9-36 weeks). At followup, all the athletes, except the one with bilateral fractures had radiological union as evaluated by CT scan.
The complications that occurred were nonunion in one patient (bilaterally), which was subsequently treated with open surgery and bone grafting elsewhere with reportedly no success. Two patients had intermittent, recurrent midfoot pain that did not interfere with their activities or participation in high level sports competition [Table 2]. There were no complications of the procedure itself.
DISCUSSION
Stress fractures of the tarsal naviculum bone are being recognized with increasing frequency in physically active patients.[9] Most studies performed previously have recommended a conservative treatment strategy for these fractures[10,11,12] with varying durations of plaster cast immobilization ranging from 5 to 12 weeks.[3,10,13,14] These studies show that this form of treatment is unpredictable in respect to the time to union, with no guarantee of full union being achieved following treatment. It leaves the elite athlete with a long duration of immobilization, leading to stiffness, weakness and an extended period away from participation in sports. In addition, it surely results in frustration and psychological morbidity in these highly motivated individuals, resulting in a high risk of noncompliance.
Other studies have suggested that operative intervention should be implemented, but only if the fracture is displaced, fragmented or if conservative management has failed.[4,8,10] These studies have employed bone grafting and postoperative immobilization, the duration ranging from 4 to 8 weeks. We have not had cause to resort to bone grafting and suggest that this might generally have not been necessary had these fractures been treated initially by the method of fixation reported here. All but one of our patients united clinically and radiologically and one was lost to followup opting to have revision surgery elsewhere.
This study also shows that a minimally invasive procedure combined with immediate postoperative mobilization allows fracture healing to be achieved reliably in a predictable 3 month time frame with reduced delays in achieving pre-injury levels of performance for an athlete. In the past, studies have shown fairly good clinical results with nonoperative protocols. However even these authors concede that a large proportion of these fractures do not show radiological evidence of union at followup.[5] Surely, this would put them at increased risk of re-injury if these athletes were to return to the same level of sporting competition for any length of time.
Presently, the accepted standard of conservative treatment for stress fractures of the naviculum bone involves 6-8 weeks of non-weight-bearing with cast immobilization.[5] The compliance level with this prolonged immobilization especially among athletes is poor. We propose an alternative whereby, following minimally invasive surgery, the patient is able to bear weight immediately and does not require cast immobilization. This technique produces a high level of compliance and a high success rate in terms of union, pain relief and early return to the same level of sporting activities. Atleast these results should prompt further study, perhaps including a randomized controlled trial of a larger number of patients.
The strength of our study derives from the fact that all procedures were performed by a single surgeon at a single institution with a uniform postoperative management protocol and therefore the variables in management are reduced. The drawback is the limited number of patients studied and this could be overcome in future by standardizing the management protocol over a larger number of patients.
Minimally, invasive surgery and early mobilization have several advantages over any other method of treatment. Minimally, invasive fixation results in very low operative site morbidity. Early mobilization avoids fracture disease, local osteoporosis, calf muscle and generalized muscle wasting and loss of muscle tone. By avoiding cast immobilization and permitting early weight bearing ambulation, we believe that the patient is more independent, mobile and optimistic about their recovery, significantly reducing the psychological morbidity associated with prolonged immobilization. Long term followup of these patients showed that six out of eight patients were asymptomatic at followup and the other two had only intermittent mild pain, without restriction of sporting activity and therefore there is no significant long term morbidity associated with this line of management. This treatment regimen should therefore at least be offered as an option as part of properly informed consent in the standard of management of these fractures. Not only are they pain free sooner, but they return to sports faster and stay pain free long term, with no recurrence of the fracture.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Bennell KL, Malcolm SA, Thomas SA, Wark JD, Brukner PD. The incidence and distribution of stress fractures in competitive track and field athletes. A twelve-month prospective study. Am J Sports Med. 1996;24:211–7. doi: 10.1177/036354659602400217. [DOI] [PubMed] [Google Scholar]
- 2.Brukner P, Bradshaw C, Khan KM, White S, Crossley K. Stress fractures: A review of 180 cases. Clin J Sport Med. 1996;6:85–9. [PubMed] [Google Scholar]
- 3.Khan KM, Brukner PD, Kearney C, Fuller PJ, Bradshaw CJ, Kiss ZS. Tarsal navicular stress fracture in athletes. Sports Med. 1994;17:65–76. doi: 10.2165/00007256-199417010-00006. [DOI] [PubMed] [Google Scholar]
- 4.Bojanic I, Pecina MM. Conservative treatment of stress fractures of the tarsal naviculam in athletes. Rev Chir Orthop Reparatrice Appar Mot. 1997;83:133–8. [PubMed] [Google Scholar]
- 5.Burne SG, Mahoney CM, Forster BB, Koehle MS, Taunton JE, Khan KM. Tarsal naviculum stress injury: Long term outcome and clinicoradiological correlation using both computed tomography and magnetic resonance imaging. Am J Sports Med. 2005;33:1875–81. doi: 10.1177/0363546505278253. [DOI] [PubMed] [Google Scholar]
- 6.Torg JS, Pavlov H, Cooley LH, Bryant MH, Arnoczky SP, Bergfeld J, et al. Stress fractures of the tarsal naviculum. A retrospective review of twenty one cases. J Bone Joint Surg Am. 1982;64:700–12. [PubMed] [Google Scholar]
- 7.Khan KM, Fuller PJ, Brukner PD, Kearney C, Burry HC. Outcome of conservative and surgical management of navicular stress fracture in athletes. Eighty six cases proven with computerized tomography. Am J Sports Med. 1992;20:657–66. doi: 10.1177/036354659202000606. [DOI] [PubMed] [Google Scholar]
- 8.Fitch KD, Blackwell JB, Gilmour WN. Operation for nonunion of stress fracture of the tarsal navicular. J Bone Joint Surg Br. 1989;71:105–10. doi: 10.1302/0301-620X.71B1.2644288. [DOI] [PubMed] [Google Scholar]
- 9.Coris EE, Lombardo JA. Tarsal navicular stress fractures. Am Fam Physician. 2003;67:85–90. [PubMed] [Google Scholar]
- 10.Kapandji IA. The Physiology of Joints. Edinburgh Scotland: Churchill Livingstone; 1970. The Physiology of Joints. [Google Scholar]
- 11.Orava S, Karpakka J, Hulkko A, Takala T. Stress avulsion fracture of the tarsal navicular. An uncommon sports-related overuse injury. Am J Sports Med. 1991;19:392–5. doi: 10.1177/036354659101900413. [DOI] [PubMed] [Google Scholar]
- 12.Ostlie DK, Simons SM. Tarsal navicular stress fracture in a young athlete: Case report with clinical, radiologic and pathophysiologic correlations. J Am Board Fam Pract. 2001;14:381–5. [PubMed] [Google Scholar]
- 13.Torg JS, Pavlov H, Torg E. Overuse injuries in sport: The foot. Clin Sports Med. 1987;6:291–320. [PubMed] [Google Scholar]
- 14.van Langelaan EJ. A kinematical analysis of the tarsal joints. An X-ray photogrammetric study. Acta Orthop Scand Suppl. 1983;204:1–269. [PubMed] [Google Scholar]