

The aim of this study was to evaluate breast cancer (BC) incidence and mortality among young Latin American women and related clinico-pathology and survivorship. Incidence and mortality of BC are rising among this population. The resulting burden must be considered as a top priority of national programs in the fight against BC.
Keywords: Breast cancer, Latin America, Young women, Incidence, Mortality
Abstract
Background.
Breast cancer (BC) is the leading cause of malignancy-related deaths among women aged ≤45 years. There are unexplored and uncertain issues for BC in this particular group in Latin America. The aim of this study is to evaluate BC incidence and mortality among young women and related clinicopathological and survivorship aspects in this region.
Materials and Methods.
Data were obtained from Globocan 2008 and the International Agency for Research on Cancer's Cancer Incidence in Five Continents series plus databases. We requested collaboration from the 12 different national cancer institutes in Latin America through SLACOM, the Latin American and Caribbean Society of Medical Oncology, and conducted a systematic literature review to obtain local data regarding the prevalence of BC among young women and their characteristics, outcomes, and survivorship-related issues.
Results.
BC incidence and mortality proportions for Latin American women aged <44 years were higher when compared with those of developed countries (20% vs. 12% and 14% vs. 7%, respectively). We found only a few Latin American series addressing this topic, and prevalence varied between 8% and 14%. Stage II and III disease, high histological grade, and triple-negative and HER2 BC were features frequently observed among young Latin American BC patients.
Conclusion.
The rising incidence and mortality of BC in young Latin American women is a call to action in the region. It is necessary to monitor the epidemiological and clinical data through reliable cancer registries and to consider the implementation of protocols for education of patients and health professionals. This unmet, growing burden must be considered as a top priority of the national programs in the fight against BC, and models of specialized units should be implemented for this particular group of patients to provide better care for this emergent challenge.
Implications for Practice:
This review illustrates that breast cancer (BC) among Latin American women is a growing burden throughout the region. The increased proportion of BC cases in young women is important because their diagnoses and tumor behavior are usually more aggressive than in their older counterparts. The findings of this study reveal that there is scarce information regarding this matter in Latin American countries, especially concerning the particular effects and complications that this group of women face during and after treatment. Also, there are no specific clinical or educational programs that focus on this population. A call to action from health policy planners, medical providers, researchers, BC patients, families, and the community in general is deserved for better care of this emergent challenge.
Introduction
Worldwide, breast cancer (BC) is the most common cancer afflicting women, and its incidence and mortality are expected to increase by 50% between 2002 and 2020 [1]. These rising cancer rates will be disproportionately high in developing countries and are projected to reach 55% increased incidence and 58% greater mortality in less than 20 years [2].
For women aged ≤45 years, BC is the leading cause of malignancy-related deaths [3]. Available data suggest that BC in younger women represents a significant burden in developing countries because more than 20% of BC cases and more than 20% of deaths occur in women aged <45 years, in contrast to developed countries where these figures correspond to less than 12% and 10%, respectively [4, 5].
The definition of a “young woman” in the field of breast oncology varies, with most articles referring to women under ages 35, 40, or 45 as “young” [6]. Among women with premenopausal BC, there are reasons to believe that further subdivision into those with very early onset disease (before age 40) and relatively early onset disease (40–49 years) is meaningful [7].
This increased proportion of BC cases in young women is important because their diagnoses and tumor behavior are usually more aggressive than in their older counterparts, with a disproportionate number of life-years lost because of cancer [8]. This is because of the frequent presentation of advanced stages at diagnosis, more aggressive pathological features, a greater proportion of triple-negative and HER2-overexpressing tumors, and higher rates of systemic relapse at any clinical stage compared with older women [9, 10].
It has been reported that the particular needs of this growing population of young women with BC are not often covered [3]. The increased risk of locoregional recurrence, optimal methods for fertility preservation, precise psychosocial interventions for these women, challenges related to a longer survival period, and associated costs for the already compromised health care system remain uncertain and unexplored [11].
For Latin American countries, BC is the most common cause of cancer and the leading cause of cancer mortality among women [12]. The growing incidence may be explained partly by efforts that have translated in improvement in BC screening, whereas the high mortality rate is largely the result of late disease stage at presentation, leading to particularly poor outcomes when coupled with limited diagnosis and treatment capacity [1]. In this region, BC mortality has increased over the past two decades, and survival, on average, is 20% lower than in the U.S. and Western Europe [13].
The aim of this study is to evaluate the distribution of BC incidence and mortality among young women and to describe related clinicopathological and survivorship aspects in this region. The recognition of this growing problem in our countries should lead the medical community, governments, and health care systems toward the implementation of specialized programs to address the particular needs of this population because BC represents a great challenge to patients, families, and health care providers.
Materials and Methods
The data for the distribution analyses of incidence and mortality for women aged <39 years and <44 years with BC in Latin American countries were obtained from Globocan 2008, as well as information about other low-income and high-income elected regions for comparison [14]. All Latin American countries with reported data in Globocan were included. Data from Central American countries was reported as an entire region. U.S., Canada, European Union, U.K., Japan, India, and Sub-Saharan Africa were selected according to their gross domestic product and worldwide representation.
In the absence of country-specific national or local incidence data or when information is considered to be of insufficient quality, as is the case for many Latin American countries, Globocan uses regional models to estimate incidence and mortality rates [14]. Consequently, we obtained statistics from the International Agency for Research on Cancer (IARC) Cancer Incidence in Five Continents databases, which provide access to detailed and accurate information on cancer incidence recorded by registries (regional or national) worldwide. Registries that contain the most current information (up to 2002) from Argentina, Brazil, Colombia, Costa Rica, and Ecuador were included [14]. Data on incidence and mortality were estimated in each country and are presented as proportions for BC in women aged <39 years and <44 years.
We identified relevant BC studies written in English or Spanish through a structured literature search on Medline (Jan 1, 1995 to Aug 15, 2013) using the Medical Subject Headings “breast neoplasm,” “breast cancer,” or “breast tumors” and “young women” or “premenopausal.” In addition to these terms, searches of “breast neoplasm” and “Argentina” and “Belize” and “Bolivia” and “Brazil” and “Chile” and “Colombia” and “Costa Rica” and “Cuba” and “Ecuador” and “El Salvador” and “Guatemala” and “Guiana” and “Haiti” and “Honduras” and “Mexico” and “Nicaragua” and “Panama” and “Paraguay” and “Peru” and “Uruguay” or “Venezuela” were performed. We included 4 of 95 retrieved articles. Exclusion criteria were studies not specific to BC and young women or those who did not include patients from Latin America. References of all relevant articles were also screened for further eligible manuscripts.
We requested collaboration from the 12 different national cancer institutes in Latin America through SLACOM, the Latin American and Caribbean Society of Medical Oncology, to share either BC statistics or their own series regarding this group of patients. Through this search, we obtained a few additional published and unpublished reports from either regional cancer or hospital-based registries from Argentina, Brazil, Colombia, Mexico, Venezuela, and Peru.
Results
As shown in Figure 1, BC incidence and mortality proportions among Latin American young women from the total of BC cases and deaths were higher when compared with those of selected developed regions. The proportion of incident cases among Latin American women aged 0–44 years was higher when compared with those of developed countries in North America (20% vs. 12%; Fig. 1A, 1B). The same distribution was observed for the mortality analysis (14% vs. 7%), as presented in Figure 1C and 1D. Figures 2–4 show that the proportion of BC-incident cases and deaths was greater among young women for all Latin American countries, including Mexico and Central America, compared with high-income regions (European Union, U.S., U.K., and Japan). Other developing areas, such as India or Sub-Saharan Africa presented an even greater proportion of BC cases and deaths among young women. The observed distribution of incident cases divided by age collected from either Globocan or the IARC Cancer Incidence in Five Continents databases was similar for incidence evaluations among countries (Figs. 2 and 3).
Figure 1.

Breast cancer incidence by age group in Latin America (A) and North America (B) and breast cancer mortality by age group in Latin America (C) and North America (D).
Figure 2.

Breast cancer incidence by age group (International Agency for Research on Cancer registries): 0–39 yr versus 40–≥75 yr (A) and 0–44 yr versus 45–≥75 yr (B).
Abbreviations: IARC, International Agency for Research on Cancer; SEER, Surveillance Epidemiology and End Results.
Figure 3.

Breast cancer incidence by age group (Globocan): 0–39 yr versus 40–≥75 yr (A) and 0–44 yr versus 45–≥75 yr (B).
Figure 4.

Breast cancer mortality by age group (Globocan): 0–39 yr versus 40–≥75 yr (A) and 0–44 yr versus 45–≥75 yr (B).
The clinicopathological characteristics among young BC patients described in Latin American series are shown in Table 1 [15–25]. The proportion of women aged <40 years varies between countries from 8.2% to 14%. Stage II (66% in Mexico and 49% in Peru) and stage III (26% and 66% in Mexico and 38% in Peru) were the most common presentations at diagnosis [20, 23]. Regarding tumor subtypes, the most frequent histological BC was luminal A (55% in Brazil and 49% in Costa Rica) [17, 21], although triple-negative or basal-like tumors (18% in Brazil, 22% in Costa Rica, 26% and 32% in Mexico, and 35% in Peru) and in some series, HER2-positive BC (17% and 27% in Mexico) were also prevalent [17, 20–23]. In addition, high grade was a common feature of tumors among studied cases (86% in Costa Rica and 43.5% in Peru) [20, 21].
Table 1.
Clinical and pathological features of breast cancer in young Latin American women

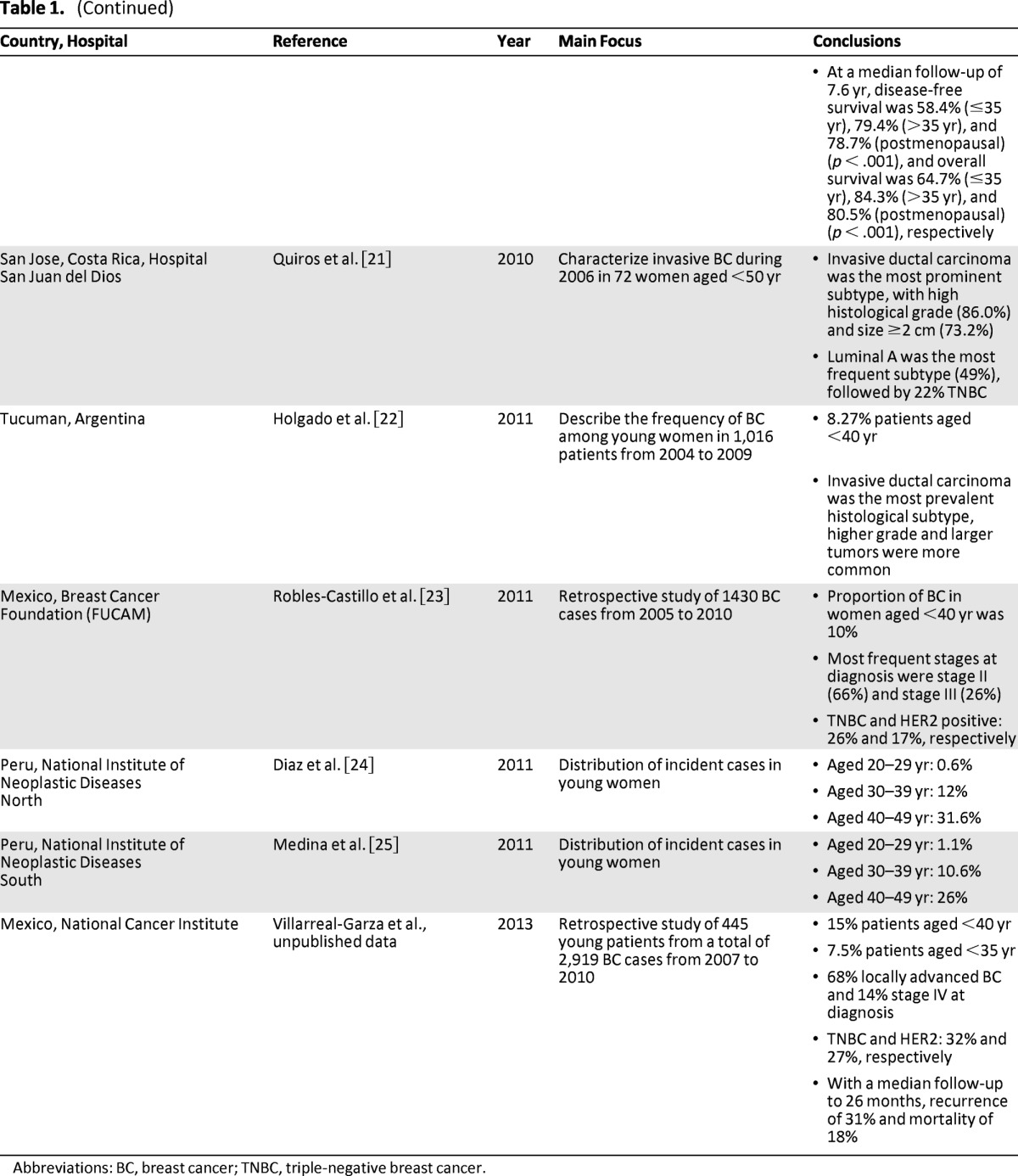
Abbreviations: BC, breast cancer; TNBC, triple-negative breast cancer.
Concerning long-term follow-up, only Peruvian data reported outcomes, which were inferior in the younger population [20]. Overall survival was 64.7% for women aged ≤35 years, 84.3% for women aged >35 years, and 80.5% for postmenopausal women (p < .001). Disease-free survival was 58.4% for women aged ≤35 years, 79.4% for women aged >35 years, and 78.7% for postmenopausal women (p < .001). At the Mexican National Cancer Institute, the reported recurrence rate was 31% and mortality was 18% at a follow-up of 26 months (unpublished data).
There were no studies in Latin America that addressed survival-related issues and the needs of young women with BC, such as quality of life, cognition, or sexuality aspects.
Discussion
A Largely Undefined, Growing Burden
Although the overall burden per 100,000 women is highest in developed countries, where incidence rates are higher, it is worth noting that the disease burden per BC case is greater in developing countries because of the higher mortality rates and the younger age of women at diagnosis [8]. Consequently, productivity losses because of younger age at death are exacerbated by the increased morbidity resulting from younger age at diagnosis in economically developing nations [8].
Table 2 shows the mean age at diagnosis and death from BC in Latin American countries [6, 8], generally 10 years younger than those reported in developed countries (which does not apply for certain countries such as Argentina and Uruguay). The reason for this earlier presentation is largely undefined. Although a plausible explanation might be the younger age distribution among the region's female population, according to data published by López-Carrillo et al. [26], only two-thirds of those early cases can be attributed to a younger age distribution in the Latin American population. The authors also revealed that although there were lower age-specific incidence rates in the Latin American registries, these grew faster in the analyzed period than those in the U.S. and Canadian cancer registries [26].
Table 2.

Data from the International Agency for Research on Cancer's database, Globocan 2008.
Data from the Pan American Health Organization's mortality database covering 2004–2006.
Another possible rationale for the high and growing proportion of this young BC population is a combination of demographic, hereditary, environmental, and lifestyle risk factors resembling the more developed countries. Changes in reproductive behaviors over the past 50 years, for example, have translated into steadily decreased fertility rates in Latin American countries, and this trend is inversely associated with BC incidence [27]. In addition, there is an emerging shift in the region toward later onset of childbearing and possibly an increasing proportion of women choosing to forgo having children [28].
It has been postulated that the set of molecular and genetic characteristics of BC arising in younger women, such as BRCA mutations, may be different from those of older women and that a greater prevalence of genetic mutations might explain the rising proportion of BC cases among young women in Latin America. Initial studies of the prevalence of deleterious mutations in BRCA1 and BRCA2 have suggested that these mutations may account for a higher proportion of BC in Hispanics than other non–Ashkenazi Jewish populations [29, 30]. Studies of mutations have been conducted in Brazil [31], Colombia [32], Chile [33], and Mexico [34–36], with variable results on the prevalence of BRCA mutations. The largest study of Hispanic breast and ovarian cancer families in the U.S. confirmed a high prevalence of BRCA mutations (25%) as well as a pattern of multiple recurrent mutations in a mostly Mexican-American population [37]. BRCA1 ex9–12del is the first reported Mexican founder mutation [30], which, along with other recurrent mutations, suggests the potential for a cost-effective panel approach for genetic testing.
Limited High-Quality Information in Latin America Concerning BC in Young Women
Unfortunately, in Latin America, there is a scarcity of high-quality cancer registries. It is estimated that only 6% of the Latin American population is included in population-based cancer registries versus 83% in North America and 32% in Europe [38]. It is recognized that the most effective approach to the cancer burden is through a cancer control plan based on evidence from reliable data. This approach helps monitor the results of strategic interventions and allows the development of specialized programs targeted to the specific needs of each population or region, according to existing resources. At this time, only Argentina, Brazil, Chile, Colombia, Cuba, Costa Rica, Ecuador, and Peru have developed cancer registries in the region. The World Health Organization, through the IARC, highlights examples of the translation of registry information into tangible results from Argentina, Colombia, and Ecuador [39]. It is imperative to stimulate their implementation in the remaining Latin American countries that lack registries, and in turn this will help researchers understand the increase of BC in Latin America. A new project of the IARC, the Global Initiative for Cancer Registry Development in Low and Middle Income Countries, includes launching a regional center in Latin America that will aid the improvement of this urgent situation [40].
There is scant information in Latin America about clinical and histological characteristics, gene expression, molecular patterns, prognosis, survivorship, and risk factors among young BC patients compared with what is known in the U.S. and other developed countries. It is important to devote more research to this topic because this population represents a growing burden for Latin America, and many aspects remain unclear.
BC in Young Women: Special Considerations
The principles of care and treatment for invasive BC in young women are the same as those for older women, although there are several particularly challenging age-related issues in this group, such as fertility impairment after cancer treatment, impaired cognition, and effects on bone mineral density [41–44]. Furthermore, these women are recognized to be more vulnerable to emotional distress and psychosocial problems needing special supportive interventions [11]. Known causes that diminish quality of life for these women include premature menopause induced by treatment, body image disturbance caused by surgery, compromised sexual function, and the constant threat of disease recurrence and death [45]. Moreover, this population represents an important economically active population that often serves as primary moral and financial support to their families. It is also the age at which the professional phases, social lives, and family projects of these women are consolidated. Other particular issues that young BC patients might face in developing countries are marital problems, violence and abuse, child-care issues, economic loss, stigma, and a perception of discrimination [46].
There are scant data related to the treatment impact on these young women; for instance, despite the use of more aggressive treatment based on the use of radiation, anthracyclines, and taxanes, little is known regarding long-term cardiac toxicity or other long-term side effects. In addition, few data are reported related to cognitive impairment associated with the use of hormonal and chemotherapy treatment, which can be particularly problematic for the continuation of professional and family-related plans of young women. A European Organization for Research and Treatment of Cancer study about fertility attitudes in young BC women, which included 12% of patients from South America (Peru and Chile), showed that Latin American patients required an increase in the chance of being cured to accept chemotherapy with potential fertility loss and were less likely to accept higher infertility rates than women from the Middle East and Western and Eastern Europe [47].
For a more comprehensive and positive impact on this group of women, the implementation of interdisciplinary management through program models for recognition and attention to their multifaceted care needs has been recommended. Because of the relatively rare incidence of BC in women aged ≤40 years in developed nations, there is little experience in this matter, and few centers are equipped to address the medical and psychological difficulties that these women could present.
Special programs are required for young women with BC in Latin America. The models of specialized clinics for the care of these patients at the Sunnybrook Odette Cancer Centre in Toronto, Canada, and at the Dana-Farber Cancer Institute and Brigham and Women's Hospital in Boston, Massachusetts, under the leadership of Dr. Ellen Warner [48] and Dr. Ann Partridge [3], respectively, offer an innovative strategy for more appropriate care. Similarly, both models offer an interdisciplinary approach, including psychosocial support and body image, early referral to genetic and fertility counseling, and support for sexual health and rehabilitation. The programs also feature seminars and educational activities for patients and cancer survivors.
We adopt the model of a specialized clinic for the care of young women with BC, the first in Latin America, at the National Cancer Institute in Mexico. The goals of our clinic include optimizing complex clinical care and supporting needs for young women with BC and their families; promoting medical, biomedical, and social research focused on the needs of these young women; and educating this group of women and health professionals regarding their specific requirements to promote early cancer detection and better multidisciplinary management for this subgroup of patients. Similar initiatives can be replicated or extended to other cancer centers and to primary care in Mexico. In this way, it is intended that the program organization and structure can reach national and eventually international interactions and serve as a model for other Latin American countries.
Conclusion
The rising incidence and mortality of BC among young Latin American women is a call to action in the region. Further research is necessary in order to understand and characterize the real scenario of this particular group of patients in our countries. These efforts should be focused on understanding the clinical, molecular, sociocultural, and educational traits and issues related to survival. Moreover, the data presented urge all Latin American countries to consider the implementation of protocols for patient education and for health professionals who treat and follow these women. This unmet, growing burden must be considered a top priority for the national programs in the fight against BC. Models of specialized units should be implemented for this particular group of patients to provide better care for this emergent challenge.
Author Contributions
Conception/Design: Cynthia Villarreal-Garza, Christian Aguila
Provision of study material or patients: Cynthia Villarreal-Garza, Christian Aguila, Maria C. Magallanes-Hoyos, Enrique Bargalló, Abelardo Meneses, Eduardo Cazap, Henry Gomez, Raúl Murillo, Carlos Barrios
Collection and/or assembly of data: Cynthia Villarreal-Garza, Christian Aguila, Maria C. Magallanes-Hoyos, Henry Gomez, Raúl Murillo, Carlos Barrios
Data analysis and interpretation: Cynthia Villarreal-Garza, Alejandro Mohar, Eduardo Cazap, Lizbeth López-Carrillo, Yanin Chávarri-Guerra
Manuscript writing: Cynthia Villarreal-Garza, Christian Aguila, Maria C. Magallanes-Hoyos, Alejandro Mohar, Enrique Bargalló, Abelardo Meneses, Eduardo Cazap, Henry Gomez, Lizbeth López-Carrillo, Yanin Chávarri-Guerra
Final approval of manuscript: Cynthia Villarreal-Garza, Christian Aguila, Maria C. Magallanes-Hoyos, Alejandro Mohar, Enrique Bargalló, Abelardo Meneses, Eduardo Cazap, Henry Gomez, Lizbeth López-Carrillo, Yanin Chávarri-Guerra, Raúl Murillo, Carlos Barrios
Disclosures
Eduardo Cazap: Sociedad Latinoamericana y del Caribe de Oncología Médica, Union for International Cancer Control, Breast Health Global Initiative, and the National Cancer Institute of Argentina (E); Bayer, Schering Pharma (C/A); Bayer, Bristol-Myers Squibb, Fresenius, Roche (H); Poniard Pharmaceuticals, Daiichi Sankyo Pharma, Breast Cancer Research Foundation (RF). The other authors indicated no financial relationships.
(C/A) Consulting/advisory relationship; (RF) Research funding; (E) Employment; (H) Honoraria received; (OI) Ownership interests; (IP) Intellectual property rights/inventor/patent holder; (SAB) Scientific advisory board
References
- 1.Anderson BO, Yip CH, Smith RA, et al. Guideline implementation for breast healthcare in low-income and middle-income countries: Overview of the Breast Health Global Initiative Global Summit 2007. Cancer. 2008;113(suppl):2221–2243. doi: 10.1002/cncr.23844. [DOI] [PubMed] [Google Scholar]
- 2.Anderson BO, Cazap E, El Saghir NS, et al. Optimisation of breast cancer management in low-resource and middle-resource countries: Executive summary of the Breast Health Global Initiative consensus, 2010. Lancet Oncol. 2011;12:387–398. doi: 10.1016/S1470-2045(11)70031-6. [DOI] [PubMed] [Google Scholar]
- 3.Partridge AH, Ruddy KJ, Kennedy J, et al. Model program to improve care for a unique cancer population: Young women with breast cancer. J Oncol Pract. 2012;8:e105–e110. doi: 10.1200/JOP.2011.000501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Knaul F, Bustreo F, Ha E, et al. Breast cancer: Why link early detection to reproductive health interventions in developing countries? Salud Publica Mex. 2009;51(suppl 2):220–227. doi: 10.1590/s0036-36342009000800012. [DOI] [PubMed] [Google Scholar]
- 5.Knaul F, Arreola-Ornelas H, Méndez O. Distribución por edad del CaMa en países en vías de desarrollo: Introducción a los datos de GLOBOCAN 2008. [Accessed November 1, 2013]. Available at: http://www.scribd.com/doc/91316254/Breast-cancer-onset-age-distribution-in-developing-countries-Global-and-regional-patterns-of-age-at-onset-and-mortality-180811.
- 6.Gabriel CA, Domchek SM. Breast cancer in young women. Breast Cancer Res. 2010;12:212. doi: 10.1186/bcr2647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Narod SA. Breast cancer in young women. Nat Rev Clin Oncol. 2012;9:460–470. doi: 10.1038/nrclinonc.2012.102. [DOI] [PubMed] [Google Scholar]
- 8.A review of breast cancer and outcomes in Latin America, 2012. [Accessed November 1, 2013]. Available at: http://www.paho.org/hq/index.php?option=com_docman&task=doc_download&gid=17994&Itemid=
- 9.Han W, Kim SW, Park IA, et al. Young age: An independent risk factor for disease-free survival in women with operable breast cancer. BMC Cancer. 2004;4:82. doi: 10.1186/1471-2407-4-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bleyer A, Barr R, Hayes-Lattin B, et al. The distinctive biology of cancer in adolescents and young adults. Nat Rev Cancer. 2008;8:288–298. doi: 10.1038/nrc2349. [DOI] [PubMed] [Google Scholar]
- 11.Shannon C, Smith IE. Breast cancer in adolescents and young women. Eur J Cancer. 2003;39:2632–2642. doi: 10.1016/s0959-8049(03)00669-5. [DOI] [PubMed] [Google Scholar]
- 12.Goss PE, Lee BL, Badovinac-Crnjevic T, et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol. 2013;14:391–436. doi: 10.1016/S1470-2045(13)70048-2. [DOI] [PubMed] [Google Scholar]
- 13.Schwartsmann G. Breast cancer in South America: Challenges to improve early detection and medical management of a public health problem. J Clin Oncol. 2001;19(suppl):118S–124S. [PubMed] [Google Scholar]
- 14.Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 15.Rodriguez-Cuevas S, Macias Martinez CG, Labastida Almendaro S. Breast cancer in Mexico. Is it a young women disease? Ginecol Obstet Mex. 2000;68:185–190. [PubMed] [Google Scholar]
- 16.Freitas R, Jr, Freitas NM, Curado MP, et al. Incidence trend for breast cancer among young women in Goiania, Brazil. Sao Paulo Med J. 2010;128(2):81–84. doi: 10.1590/S1516-31802010000200007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Carvalho LV, Pereira EM, Frappart L, et al. Molecular characterization of breast cancer in young Brazilian women. Rev Assoc Med Bras. 2010;56(3):278–287. doi: 10.1590/s0104-42302010000300010. [DOI] [PubMed] [Google Scholar]
- 18.Hernandez Aten DE, Borgas R, Betancourt L. Cáncer de mama en mujeres jóvenes evaluación de los factores de riesgo. Rev Venez Oncol. 2010;22(4):216–221. [Google Scholar]
- 19.Uribe Perez CJ, Alvarez Serrano M, Montañoz Rizo G. Incidencia de cáncer de mama en mujeres menores de 40 años en el Área Metropolitana de Bucaramanga, 2000–2004. MedUNAM 2010. 2010;13(2):81–84. [Google Scholar]
- 20.Vallejos Sologuren C, Gomez HL, Abugattas JE, et al. Clinicopathologic, molecular subtype, and survival prognostic features in premenopausal breast cancer patients by age at diagnosis. ASCO Meeting Abstracts. 2010;28(suppl 15):653. [Google Scholar]
- 21.Quirós Alpízar JL, Arce Jiménez IS, Ramírez Cisneros B. Cáncer de mama en mujeres jóvenes características clínicas y patológicas. Rev Med Univ Costa Rica. 2006;4(2):54–64. [Google Scholar]
- 22.Holgado S, Sanchez Segura M, Vinuales A, et al. Breast cancer in young women in a northern province of Tucuman, Argentina. ASCO Meeting Abstracts. 2011;29(suppl 15):e12022. [Google Scholar]
- 23.Robles-Castillo J, Ruvalcaba-Limon E, Maffuz A, Rodriguez-Cuevas S. Breast cancer in Mexican women under 40. Ginecol Obstet Mex. 2011;79(8):482–488. [PubMed] [Google Scholar]
- 24.Díaz Plasencia JA, Hernández Morón PM, Burga Vega AM. Registro Hospitalario de Cáncer Informe 2010–2011. Instituto Regional de Enfermedades Neoplásicas “Dr. Luis Pinillos Ganona”. [Accessed November 1, 2013]. Available at: http://www.irennorte.gob.pe/pdf/epidemiologia/informe5.pdf.
- 25.Medina Fernández LE, Rodríguez Zea B. Registro de Cáncer Poblacional de Aréquipa, Perú 2004–2007. Instituto Regional de Enfermedades Neoplásicas del Sur. [Accessed November 1, 2013]. Available at: http://www.irensur.gob.pe/rcc/pdf/c6.pdf.
- 26.López-Carrillo L, Franco-Marina F, Keating N, et al. Breast cancer: Age at diagnosis patterns in Latin America and Caribbean. [Accessed November 1, 2013]. Available at: http://www.saludpublica.uchile.cl/saludglobal_2013/es/Simposios_simultaneos/La_lucha_global_contra_el_cancer/Lizbeth_Lopez.pdf.
- 27.Robles SC, Galanis E. Breast cancer in Latin America and the Caribbean. Rev Panam Salud Publica. 2002;11:178–185. doi: 10.1590/s1020-49892002000300007. [DOI] [PubMed] [Google Scholar]
- 28.Rosero-Bixby L, Castro-Martín T, Martín-García T. Is Latin America starting to retreat from early and universal childbearing? Demographic Research. 2009;20:169–194. [Google Scholar]
- 29.Weitzel JN, Lagos V, Blazer KR, et al. Prevalence of BRCA mutations and founder effect in high-risk Hispanic families. Cancer Epidemiol Biomarkers Prev. 2005;14:1666–1671. doi: 10.1158/1055-9965.EPI-05-0072. [DOI] [PubMed] [Google Scholar]
- 30.Weitzel JN, Lagos VI, Herzog JS, et al. Evidence for common ancestral origin of a recurring BRCA1 genomic rearrangement identified in high-risk Hispanic families. Cancer Epidemiol Biomarkers Prev. 2007;16:1615–1620. doi: 10.1158/1055-9965.EPI-07-0198. [DOI] [PubMed] [Google Scholar]
- 31.Gomes MC, Costa MM, Borojevic R, et al. Prevalence of BRCA1 and BRCA2 mutations in breast cancer patients from Brazil. Breast Cancer Res Treat. 2007;103:349–353. doi: 10.1007/s10549-006-9378-6. [DOI] [PubMed] [Google Scholar]
- 32.Torres D, Rashid MU, Gil F, et al. High proportion of BRCA1/2 founder mutations in Hispanic breast/ovarian cancer families from Colombia. Breast Cancer Res Treat. 2007;103:225–232. doi: 10.1007/s10549-006-9370-1. [DOI] [PubMed] [Google Scholar]
- 33.Gallardo M, Silva A, Rubio L, et al. Incidence of BRCA1 and BRCA2 mutations in 54 Chilean families with breast/ovarian cancer, genotype-phenotype correlations. Breast Cancer Res Treat. 2006;95:81–87. doi: 10.1007/s10549-005-9047-1. [DOI] [PubMed] [Google Scholar]
- 34.Ruiz-Flores P, Sinilnikova OM, Badzioch M, et al. BRCA1 and BRCA2 mutation analysis of early-onset and familial breast cancer cases in Mexico. Hum Mutat. 2002;20:474–475. doi: 10.1002/humu.9084. [DOI] [PubMed] [Google Scholar]
- 35.Calderon-Garciduenas AL, Ruiz-Flores P, Cerda-Flores RM, et al. Clinical follow up of Mexican women with early onset of breast cancer and mutations in the BRCA1 and BRCA2 genes. Salud Publica Mex. 2005;47:110–115. doi: 10.1590/s0036-36342005000200004. [DOI] [PubMed] [Google Scholar]
- 36.Villarreal-Garza C, Herrera LA, Herzog J, et al. Significant clinical impact of recurrent BRCA1 and BRCA2 (BRCA) mutations in Mexico. Cancer Res. 2012;72(suppl):PD08–06. doi: 10.1002/cncr.29058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Weitzel JN, Clague J, Martir-Negron A, et al. Prevalence and type of BRCA mutations in Hispanics undergoing genetic cancer risk assessment in the southwestern United States: A report from the Clinical Cancer Genetics Community Research Network. J Clin Oncol. 2013;31:210–216. doi: 10.1200/JCO.2011.41.0027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Curado M. P., Edwards B., Shin H. R., et al., editors. Cancer Incidence in Five Continents. Vol. IX. Lyon, France: International Agency for Cancer Research; 2007. [Google Scholar]
- 39.Jensen MB, Parkin DM, MacLennan R, et al. Cancer Registration: Principles and Methods (IARC Scientific Publications) New York, NY: Oxford University Press; 1991. [Google Scholar]
- 40.Global Initiative for Cancer Registry Development in Low- and Middle-Income Countries. International Agency for Research on Cancer. [Accessed Aug 15, 2013]. Available at: http://gicr.iarc.fr/
- 41.Partridge AH, Gelber S, Peppercorn J, et al. Web-based survey of fertility issues in young women with breast cancer. J Clin Oncol. 2004;22:4174–4183. doi: 10.1200/JCO.2004.01.159. [DOI] [PubMed] [Google Scholar]
- 42.Fobair P, Stewart SL, Chang S, et al. Body image and sexual problems in young women with breast cancer. Psychooncology. 2006;15:579–594. doi: 10.1002/pon.991. [DOI] [PubMed] [Google Scholar]
- 43.Burwell SR, Case LD, Kaelin C, et al. Sexual problems in younger women after breast cancer surgery. J Clin Oncol. 2006;24:2815–2821. doi: 10.1200/JCO.2005.04.2499. [DOI] [PubMed] [Google Scholar]
- 44.Armes J, Crowe M, Colbourne L, et al. Patients' supportive care needs beyond the end of cancer treatment: A prospective, longitudinal survey. J Clin Oncol. 2009;27:6172–6179. doi: 10.1200/JCO.2009.22.5151. [DOI] [PubMed] [Google Scholar]
- 45.Avis NE, Crawford S, Manuel J. Quality of life among younger women with breast cancer. J Clin Oncol. 2005;23:3322–3330. doi: 10.1200/JCO.2005.05.130. [DOI] [PubMed] [Google Scholar]
- 46.Modesitt SC, Gambrell AC, Cottrill HM, et al. Adverse impact of a history of violence for women with breast, cervical, endometrial, or ovarian cancer. Obstet Gynecol. 2006;107:1330–1336. doi: 10.1097/01.AOG.0000217694.18062.91. [DOI] [PubMed] [Google Scholar]
- 47.Senkus E, Gomez H, Dirix L, et al. Attitudes of young patients with breast cancer toward fertility loss related to adjuvant systemic therapies. EORTC study 10002 BIG 3–98. Psychooncology. 2013 doi: 10.1002/pon.3384. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 48.Ali A, Warner E. pynk: Breast cancer program for young women. Curr Oncol. 2013;20:e34–e39. doi: 10.3747/co.20.1131. [DOI] [PMC free article] [PubMed] [Google Scholar]