

An 87-year-old woman presented with subacute onset of headache, fever, and episodes of aphasia, eventually progressing to coma. Magnetic resonance imaging (MRI) revealed a newly identified enhancing left sphenoid wing meningioma with peritumoral edema in the underlying brain (Figure 1). MRI also demonstrated expansile fluid-attenuated inversion recovery (FLAIR) signal, restricted diffusion, and elevated plasma volume in the medial temporal lobe more suggestive of superimposed infection. Electroencephalogram (EEG) showed left periodic lateralized epileptiform discharges (PLEDS). Cerebrospinal fluid (CSF) analysis showed herpes simplex virus 1 (HSV1) by polymerase chain reaction (PCR). Despite treatment with intravenous acyclovir, the patient remained comatose and comfort measures were pursued. Herpes encephalitis has been described in the setting of cancer and brain metastases but not concurrently with meningioma.1,2 Postmortem examination confirmed HSV1 and meningioma (Figure 2).
Figure 1.

MRI showing an enhancing left sphenoid wing meningioma with edema in the underlying temporal lobe (white arrowheads in A, B), expansile FLAIR signal, restricted diffusion (red arrowheads in C, D), and elevated plasma volume in the medial temporal lobe (blue arrowheads in E) suggestive of superimposed infection rather than peritumoral edema alone. Abbreviations: MRI, magnetic resonance imaging; FLAIR, fluid-attenuated inversion recovery.
Figure 2.
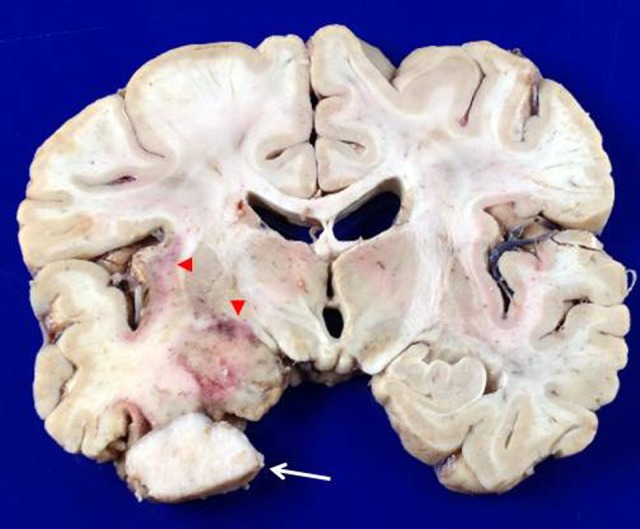
Postmortem examination demonstrating herpes encephalitis and meningioma in situ (white arrow), as well as hemorrhagic necrosis of the left insula and medial temporal lobe (red arrowheads).
References
- 1. Graber JJ, Rosenblum MK, DeAngelis LM. Herpes simplex encephalitis in patients with cancer. J Neurooncol. 2011;105(2):415–421 [DOI] [PubMed] [Google Scholar]
- 2. Manz HJ, Phillips TM, McCullough DC. Herpes simplex type 2 encephalitis concurrent with known cerebral metastases. Acta Neuropathol. 1979;47(3):237–240 [DOI] [PubMed] [Google Scholar]