

Abstract
Background:
The expertise required for proper electroencephalography (EEG) setup can make the 10-20 array unwieldy in the hospital setting. There may be a role for an EEG array with reduced leads to improve the efficiency of inpatient practice.
Methods:
Clips from 100 EEG records, 50 ictal and 50 non-ictal, in adult inpatients from January 1, 2007, to January 1, 2012, were retrospectively reviewed and selected for digital lead reduction and blind review. Two epileptologists reviewed these tracings and documented the presence of seizures and severe disturbance of background. The reduced array included 7 leads spanning the scalp. Three different montages were available. Sensitivity and specificity of the reduced array were calculated using the formal EEG report as the comparison standard.
Results:
For the detection of any seizure, the reduced array EEG had a sensitivity of 70% and specificity of 96%. Sensitivity for identifying encephalopathic patterns was 62% and specificity was 86%. Focal seizures were more readily identified by the reduced array (20 of 25) than were generalized ictal patterns (13 of 25).
Conclusion:
The reduced electrode array was insufficiently sensitive to seizure detection. Reducing EEG leads might not be a preferred means of optimizing hospital EEG efficiency.
Keywords: EEG, montage, seizure, hospital, reduced, array
Introduction
A full electroencephalography (EEG) array, based on the internationally recognized 10-20 system of electrode placement, is the standard diagnostic test by which clinicians diagnose seizures. Moreover, rapid alteration in mentation without obvious clinical seizure is a frequent occurrence in hospitals and intensive care units, and EEG is frequently performed in that setting to identify potential epileptic abnormalities or nonspecific encephalopathic patterns.1,2 The skill and materials involved in the standard application of leads can be unwieldy in the emergency department and hospital setting, particularly in agitated patients or those with other lines and drains that might interfere with proper lead placement. Even the most skilled of technicians require tens of minutes to apply a full array of leads properly, which can seem long when a diagnosis is desired as quickly as possible. On-again-off-again leads for diagnostics in the dynamic acute care setting adds to costs for materials and skilled technician time; the increased use of materials may be partially mitigated by the use of neuroimaging-compatible EEG leads, but these are more expensive than standard leads, and thus they may not dramatically cut costs. There is reasonable interest in developing a readily available and applicable EEG array with adequate sensitivity and specificity to capture or exclude a seizure in the hospital setting. One potential means of achieving this efficiency would be to reduce the number of leads employed to capture EEG data. Potential benefits include the use of less material, the ease and speed of lead application, and the possibility of house staff or other non-EEG professionals applying the leads to reduce cost and coverage gaps.
The quest for an efficient and effective reduced array is not a new one.3–7 Most of the studies to date have chosen a 7-lead3 or 8-lead5,7 “hairline” arrays. The methodology and cohort characteristics vary between studies, but there are common features to their conclusions and criticisms. Each of these studies demonstrated unacceptably poor sensitivity for seizure detection (60%-70%) but rather good specificity (>90%). These studies were for the most part retrospective reviews of a small number of patients subject to selection bias. One study of a single-lead quantitative analysis (eg, amplitude integrated) EEG in critically ill patients was similarly too insensitive to seizures when interpreted by nonexpert intensivists.6
One small retrospective study of a 7-lead EEG array stands out from the others because of the excellent reported sensitivity.4 In this study, both resident and staff reviewers identified seizures using this array with >90% sensitivity when compared to the full electrode array. Given these discordant results in the current literature, we aimed to further study the accuracy of a reduced lead EEG in hospitalized patients. We hypothesized that a reduced electrode array can detect and exclude electrographic seizures and severe disturbance of EEG background with acceptable sensitivity and specificity for use in the hospital setting.
Methods
The authors retrospectively searched the Mayo Clinic EEG Report System database of hospitalized adults between January 1, 2007, and January 1, 2012. Search terms included “seizure,” “non-convulsive,” “non convulsive,” “nonconvulsive,” “status,” “status epilepticus,” and “severe disturbance.” Diagnostic reports were reviewed in a chronologically consecutive fashion with the goal of selecting 100 cases, 50 with seizures and 50 without. Those 100 cases were found in 99 unique patients. Of the 50 recordings with seizures, the following seizure types were captured for review: focal (n = 25), nonconvulsive status epilepticus (NCSE, n = 11), generalized (n = 10), and convulsive status epilepticus (CSE, n = 4). Of the 50 recordings without seizure, 39 had a severe disturbance of the background and 11 studies were normal or had only minor slowing. Severe disturbance of the background was defined as generalized slowing in the delta range, triphasic waves, periodic epileptiform discharges (lateralized or generalized), or suppression. Once cases were identified by review of reports, one of the investigators (O.J.) reviewed the tracings of each study for representative 5- to 10-minute clips. These clips were de-identified and assigned a random study number between 1 and 100.
The authors developed a reduced electrode array as depicted in Figure 1. This array was designed within the XLTEK (Oakville, Ontario, Canada) software system to simulate the circumstance of having acquired the electroencephalographic data with only those 7 leads. The following montages were created to work within this digital array: referential (to Cz), transverse (F3-F4, T7-Cz, Cz-T8, O1-O2), and bipolar (“double banana,” F3-T7, T7-O1, F3-Cz, F4-Cz, Cz-O1, Cz-O2, F4-T8, T8-O2). All 3 montages were displayed on the screen simultaneously to further expedite the review process. The reviewers were allowed to review any video data accompanying the EEG.
Figure 1.
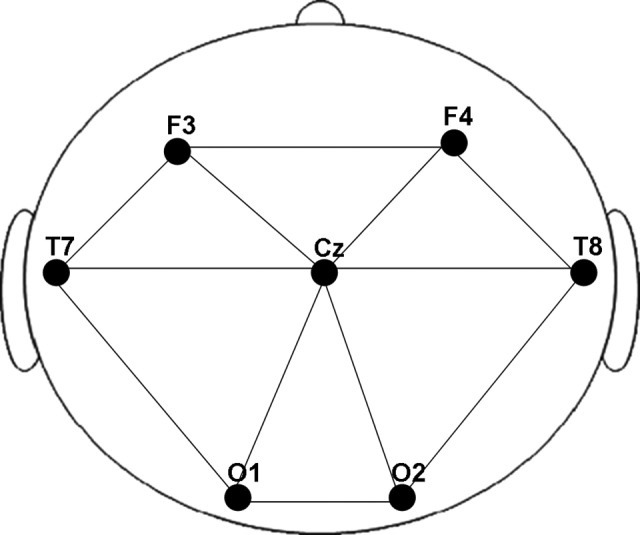
The reduced electroencephalography (EEG) array.
The review process was undertaken independently by two experienced epileptologists (J.B. and G.D.C.) who were blinded to the clinical data and the formal EEG diagnosis of each patient. For each of the 100 cases analyzed with the reduced array, the reviewers designated presence or absence of seizure and severe disturbance of the background. This diagnosis was compared to that in the EEG report in the medical record, which was considered the “gold standard.” Sensitivity and specificity data were calculated for overall seizure detection and for overall detection of severe disturbance of the background. These were calculated for each reviewer individually and their combined findings. Rate of detection by seizure type was also calculated for each reviewer and their combined detection. This study was approved by the Institutional Review Board of Mayo Clinic.
Results
Test performance characteristics for detection of seizure are shown in Table 1 and for detection of severe disturbance of background in Table 2. The combined sensitivity and specificity seizure detection was 70% and 96%, respectively. The combined sensitivity and specificity for detecting severe disturbance of background was 62% and 86%, respectively. The fraction of seizures detected was ascertained by seizure type for each reviewer and their combined results (Table 3). Focal seizures (n = 25) were detected in 80% of the cases, generalized seizures (n = 10) were detected in 50% to 60% of the cases, NCSE (n = 11) in 55% of the cases, and CSE (n = 4) in 50% to 100% of the cases.
Table 1.
Test Performance for Detection of Seizures.
| Reviewer 1 | Reviewer 2 | Combined | |
|---|---|---|---|
| Sensitivity, % | 72 | 68 | 70 |
| Specificity, % | 92 | 100 | 96 |
Table 2.
Test Performance for Detection of Severe Disturbance of Background.
| Reviewer 1 | Reviewer 2 | Combined | |
|---|---|---|---|
| Sensitivity, % | 63 | 59 | 62 |
| Specificity, % | 91 | 82 | 86 |
Table 3.
Detection of Seizure With Reduced EEG Array by Seizure Type.
| Reviewer 1 | Reviewer 2 | Combined % | |
|---|---|---|---|
| Focal (n = 25) | 20/25 | 20/25 | 80 |
| Generalized (n = 10) | 6/10 | 5/10 | 55 |
| NCSE (n = 11) | 6/11 | 6/11 | 55 |
| CSE (n = 4) | 4/4 | 2/4 | 75 |
Abbreviations: CSE, convulsive status epilepticus; EEG, electroencephalography; NCSE, nonconvulsive status epilepticus.
Discussion
This study of a reduced electrode EEG array for the detection of seizures and severe disturbance of background represents the largest and most clinically diverse of its kind. The focus on clinically relevant data, including performance of the array based on several seizure types, was employed to maximize generalizability of the results. The authors constructed the digitally reduced electrode array with a specific aim to cover as much of the scalp as possible while using no more than 7 electrodes and maintaining 10-20 system-based location of those electrodes. These principles came from the consideration of “hairline” arrays being insensitive to posteriorly generated seizures and the relative success of Karakis et al4 who also employed an electrode array with greater scalp coverage. Despite our use of an array designed to maximize scalp coverage, the reduced array demonstrated less than optimal sensitivity for seizures in our study.
The main objective of EEG in the hospital is to detect seizures. Although it was slightly more sensitive for focal seizures compared to generalized patterns, our reduced array has an unacceptably poor sensitivity for seizure detection. Specificity, on the other hand, was excellent as was interrater consistency. It is worthwhile to note that our results neatly mirror the sensitivity and specificity of previous reduced array studies outside of those reported by Karakis et al.4 The sensitivity and specificity for encephalopathic patterns were also less than optimal.
Our study has limitations. The authors sought to design a safe model (eg, not relying on untested diagnostics in an emergency setting) to test the hypothesis that a reduced electrode EEG array might be useful in the hospital setting. The authors decided that a retrospective design with digital lead reduction in previously acquired data was the best means of achieving that goal, acknowledging the potential for selection bias inherent in such design. In an attempt to mitigate this, consecutive studies with the desired diagnosis in the report were selected and only then were representative clips identified, rather than selecting cases for their clear EEG abnormalities. The reviewers interpreting the reduced array tracings did not have access to clinical data which differs from clinical practice. The use of short clips and the study report as the gold standard, rather than the original full array EEG data, is also a limitation of this study.
Although the use of a reduced array might seem like a reasonable option to improve efficiency, our results suggest that the sensitivity of a reduced electrode array is too low for hospital practice where missing electrographic seizures might have particularly dangerous consequences. It is worth noting that very dissimilar reduced electrode arrays have produced similar results in performance, including our study, so the idea that a more rational electrode arrangement was all that was missing from previous reduced arrays seems untenable. Thus, our findings indicate that investigators should seek facets of EEG practice other than the use of fewer electrodes to improve the efficiency of EEG practice in the hospital.
Footnotes
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Jordan KG. Continuous EEG and evoked potential monitoring in the neuroscience intensive care unit. J Clin Neurophysiol. 1993;10(4):445–475 [DOI] [PubMed] [Google Scholar]
- 2. Jordan KG. Continuous EEG monitoring in the neuroscience intensive care unit and emergency department. J Clin Neurophysiol. 1999;16(1):14–39 [DOI] [PubMed] [Google Scholar]
- 3. Bridgers SL, Ebersole JS. EEG outside the hairline: detection of epileptiform abnormalities. Neurology. 1988;38(1):146–149 [DOI] [PubMed] [Google Scholar]
- 4. Karakis I, Montouris GD, Otis JA, et al. A quick and reliable EEG montage for the detection of seizures in the critical care setting. J Clin Neurophysiol. 2010;27(2):100–105 [DOI] [PubMed] [Google Scholar]
- 5. Kolls BJ, Husain AM. Assessment of hairline EEG as a screening tool for nonconvulsive status epilepticus. Epilepsia. 2007;48(5):959–965 [DOI] [PubMed] [Google Scholar]
- 6. Nitzschke R, Muller J, Engelhardt R, Schmidt GN. Single-channel amplitude integrated EEG recording for the identification of epileptic seizures by nonexpert physicians in the adult acute care setting. J Clin Monit Comput. 2011;25(5):329–337 [DOI] [PubMed] [Google Scholar]
- 7. Young GB, Sharpe MD, Savard M, Al Thenayan E, Norton L, Davies-Schinkel C. Seizure detection with a commercially available bedside EEG monitor and the subhairline montage. Neurocrit Care. 2009;11(3):411–416 [DOI] [PubMed] [Google Scholar]