

Abstract
Insulin autoimmune syndrome (IAS) is characterized by spontaneous hypoglycemia caused by insulin autoantibodies in the absence of exogenous insulin administration. Some drugs containing sulfhydryl compounds are known to initiate the onset of IAS. A 67-year-old female who had diabetes for 5 years visited the outpatient clinic at our institution due to diabetic peripheral polyneuropathy. She was prescribed α-lipoic acid (ALA), which contains two sulfur atoms. Two weeks later, she complained of recurrent hypoglycemic symptoms. We detected a high level of insulin and high titers of insulin autoantibodies. Her human leukocyte antigen (HLA) genotype included the DRB1*0406 allele, which indicates a high level of susceptibility to IAS. She was treated with prednisolone. After this episode, she experienced two more hypoglycemic events after taking ALA for diabetic neuropathy in other hospitals. As ALA can be used to treat diabetic peripheral polyneuropathy, physician discretion is advised based on the possibility of IAS due to ALA in diabetic patients.
Keywords: Alpha-lipoic acid, HLA-DRB1*0406 antigen, Insulin antibodies, Insulin autoimmune syndrome
INTRODUCTION
Insulin autoimmune syndrome (IAS) was initially reported by Hirata et al. [1] in 1970 and is characterized by serious hypoglycemia and high levels of blood insulin and insulin autoantibodies in the absence of exogenous insulin administration [2]. The cause of this disease is unclear, but insulin autoantibody formation is considered to be associated with autoimmune diseases such as Graves disease, rheumatoid arthritis, or drugs containing sulfhydryl compounds, mostly penicillin, D-penicillamine, or methimazole [1]. IAS occurs frequently in East Asian countries such as Korea and Japan and is associated with a genetic predisposition. α-Lipoic acid (ALA) is a sulfhydryl-containing compound used to treat diabetic peripheral neuropathy and was first reported as the cause of IAS in 2003. Most of the cases were reported in Japan, and only one case has been reported in Korea [3]. Herein, we report a case of IAS during which hypoglycemia occurred three times after associated ALA treatments.
CASE REPORT
A 67-year-old female visited the outpatient clinic of our institution complaining of numbness and coldness in both feet. She has been diagnosed with type 2 diabetes 5 years prior and was being treated with a sulfonylurea (gliclazide 30 mg). Based on the examination results, she was diagnosed with diabetic peripheral neuropathy, and thioctacid (600 mg) was prescribed. She experienced repeated occurrences of hunger, hand tremor, cold sweat, and dizziness 3 to 4 hours after a meal since having taken the drug, but symptoms consistently improved after eating snacks. Her past history was insignificant except an appendectomy 40 years prior. On physical examination, her height was 165 cm and body weight 60 kg. Blood pressure was 130/90 mm Hg. There was no thyroid goiter or skin pigmentation.
Blood examination showed leukocyte count 4,700/mm3, hemoglobin 13.0 g/dL, platelet 202,000/mm3, blood urea nitrogen 17.0 mg/dL, Cr 0.7 mg/dL, total protein 7.1 g/dL, albumin 4.6 g/dL, aspartate aminotransferase 26 IU/L, alanine aminotransferase 36 IU/L, alkaline phosphatase 116 IU/L, total cholesterol 166 mg/dL, triglyceride 115 mg/dL, high density lipoprotein 39 mg/dL, calcium 8.8 mg/dL, phosphate 3.3 mg/dL, sodium 135 mEq/L, and potassium 4.2 mEq/L. Thyroid and adrenal cortical function tests were performed. Free T4 was 1.12 ng/dL (normal range, 0.93 to 1.7), thyroid stimulating hormone 2.25 µIU/L (normal range, 0.27 to 4.2), adrenocorticotropic hormone 16.5 pg/mL (normal range, 6 to 56.7), and cortisol 13.4 µg/dL.
On admission, hemoglobin A1c (HbA1c) was 6.6%, fasting blood glucose 208 mg/dL, and postprandial blood glucose 195 mg/dL. Serum insulin, when measured by radioimmunoassay (RIA, immunoradiometric assay, INSULIN-IRMA, Biosource Europe, Nivelles, Belgium) was normal at 15.33 and 19.41 µIU/mL on fasting and postmeal, respectively (normal range, 2 to 25). However, C-peptide (immunoradiometric assay, C-Peptide IRMA, IZOTOP, Budapest, Hungary) was increased to 13.96 ng/mL on fasting and 18.24 ng/mL after meals (normal range, 1.07 to 3.51).
Sulfonylurea administration was discontinued, but the hypoglycemic symptoms persisted. After eating carbohydrate snacks between meals, daytime frequency of hypoglycemia decreased, but hypoglycemia with a level less than 50 mg/dL persisted at dawn with prolonged fasting. A 72-hour fasting test was attempted but was ended after 6 hours because the patient complained of severe hypoglycemia with a blood sugar level of 44 mg/dL. During a 6-hour examination, the blood sugar levels were 90, 70, and 44 mg/dL at baseline, 4 and 6 hours, and the serum insulin values measured by RIA were within the normal range at 22.92, 22.16, and 27.47 µIU/mL, respectively. The C-peptide values were increased to 15.60, 20.31, and 15.65 ng/mL, respectively. The antinuclear antibody was negative, while the insulin autoantibody value (RIA, Cobra 5010, Biosource Europe) was very high at 53% (normal range, <7). The human leukocyte antigen (HLA) class II result was DRB1*0406/1454. Abdominal computed tomography revealed no abnormalities in the pancreas (Fig. 1).
Fig. 1.

Abdominal computed tomography shows no abnormal lesion in the pancreas.
Because the patient continued to suffer from fasting hypoglycemia after suspending sulfonylurea administration, and serum C-peptide and insulin autoantibody levels increased, she was diagnosed with IAS. As the sulfhydryl-containing thioctacid first administered 2 weeks before the occurrence of hypoglycemia, it was regarded as the causal factor and discontinued. The patient continued to eat complex carbohydrates between meals, but hypoglycemia persisted. Prednisolone (10 mg) administration reduced the frequency of hypoglycemia and was able to be discontinued after 2 months because recovery was observed. At 4 months after diagnosis, the insulin autoantibodies were still high at 80.4%, but no signs of hypoglycemia were evident. At the 2-year follow-up, insulin autoantibody titer was reduced to 50.9%, and hypoglycemia was no longer detected.
The patient visited the rehabilitation department of another hospital to treat diabetic peripheral neuropathy 2 years after the initial occurrence and was prescribed thioctacid. Hypoglycemia recurred 10 days later, for which she visited our hospital. At that time, the patient was treated with voglibose (0.6 mg). HbA1c was 5.7% and insulin autoantibody was 77.2%. We performed a 75 g oral glucose tolerance test. The fasting plasma glucose was 98 mg/dL and the 2-hour plasma glucose after glucose load was 135 mg/dL, but serum insulin levels measured by enzyme-linked immunosorbent assay (ELISA, Roche Elecsys insulin test, Roche Diagnostics, Mannheim, Germany) were increased to more than 1,000 µU/mL for both fasting and 2 hours posttest. Fasting and 2-hour posttest C-peptide values were 10.91 and 16.92 ng/mL, respectively. After taking prednisolone (10 mg), she recovered from hypoglycemia. The dose of prednisolone was tapered by 5 mg and was discontinued 2 months later. Before discharge, the patient was instructed to avoid thioctacid. Six months after discharge, most of the values were normalized, i.e., HbA1c 5.7%, serum insulin 267 µU/mL, and C-peptide 3.71 ng/mL, but insulin autoantibodies remained high at 78% without hypoglycemia.
The patient was again prescribed thioctacid 2 years after the second occurrence, for which she revisited our hospital due to the recurrence of hypoglycemia. At that time, she was taking voglibose (0.6 mg) as a hypoglycemic agent. Her serum insulin level based on ELISA was abnormal, measuring higher than 1,000 µU/mL, while C-peptide was 21.06 ng/mL and insulin autoantibodies were 96%. According to the test results, the patient was prescribed prednisolone (5 mg), and after 4 months, serum insulin (measured by ELISA) and C-peptide were reduced to 210 µU/mL and 2.81 ng/mL, respectively, but the insulin autoantibodies remained high (88.9%). However, there was no sign of hypoglycemia (Table 1).
Table 1.
Hypoglycemia Consistently Occurred When the Patient Took α-Lipoic Acid
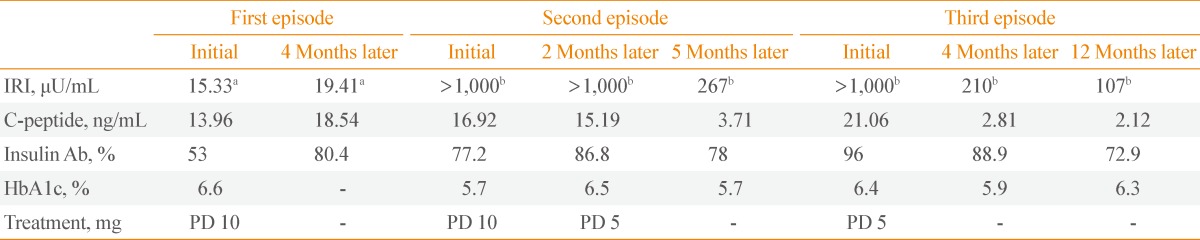
IRI, immunoreactive insulin; HbA1c, hemoglobin A1c; PD, prednisolone.
aMeasured by radioimmunoassay. Low value due to the high-dose hook effect; bMeasured by enzyme-linked immunosorbent assay.
DISCUSSION
Although the specific mechanism of IAS remains unclear, insulin autoantibodies are assumed to combine with secreted insulin as blood glucose increases after meals to inhibit insulin action and further promote the secretion of insulin. Excessive insulin combined with the autoantibody is dissociated as blood glucose is reduced and eventually induces hypoglycemia [4]. In Japan, over 200 cases of IAS-related hypoglycemia have been reported; in most cases, the patients were taking a sulfhydryl medicine 4 to 6 weeks before the occurrence of hypoglycemia. Nevertheless, several cases have been reported in which symptoms were initiated in the absence of any specific drugs or sulfhydryls such as tolbutamide, diltiazem, loxoprofen sodium, and interferone-α.
A genetic predisposition may influence the occurrence of IAS, showing a strong correlation with HLA class II and IAS is frequently observed in patients with a specific HLA allele. When considering IAS cases in Japan, 97% of patients were HLA-DR4-positive and 43% were also DRB1*0406-positive. Additionally, DQA1*0301 and DQB1*0302 alleles were frequently found in these patients [5]. The DRB1*0406 molecule has a strong affinity to the amino acid Ile-Leu-Gln motif, which is contained in the insulin α chain. Moreover, the amino acid sequence from no. 8 to no. 17 (TSICSLYQLE) of the insulin α chain has a strong affinity for DRB1*0406, and this peptide has been shown to stimulate the T cells of DRB1*040 6-positive patients. Sulfhydryl drugs promote insulin S-S bonding dissociation and expose the peptide to the antigen-presenting cell to stimulate the T cells of DRB1*0406-positive patients, resulting in the formation of insulin autoantibodies [5].
In particular, Japanese and Koreans are known to have a higher HLA-DRB1*0406-related morbidity rate than Caucasians, which is considered the main reason for the high incidence of IAS in the Japanese and Korean populations [6]. In the present case, the patient tested positive for HLA-DRB1*0406.
ALA is a relatively safe compound associated with a strong reductive reaction and thus is commonly used to treat peripheral neuropathy in diabetic patients. ALA acts as a coenzyme related to oxidative decarboxylation of pyruvic acid and α-ketoglutal acid in the mitochondria [7]. Oral ALA contains two sulfur atoms and it is reduced to dihydrolipoic acid containing sulfhydryl which decreases the oxidative stress generated in peripheral cells. The two sulfhydryls in the dihydrolipoic acid dissociate the disulfide bond of the insulin molecule to form insulin autoantibodies.
After the year 2000, ALA began gaining public attention as a dietary supplement in Japan, therefore becoming the main cause of IAS, following methimazole [7]. IAS caused by ALA has been reported a total of 20 times since first reported in Japan in 2003 [8]; 18 cases in Japan, one case in Italy [9], and one case in Korea [3] (Table 2).
Table 2.
α-Lipoic Acid-Induced Insulin Autoimmune Syndrome Reported from 2003 to August 2012
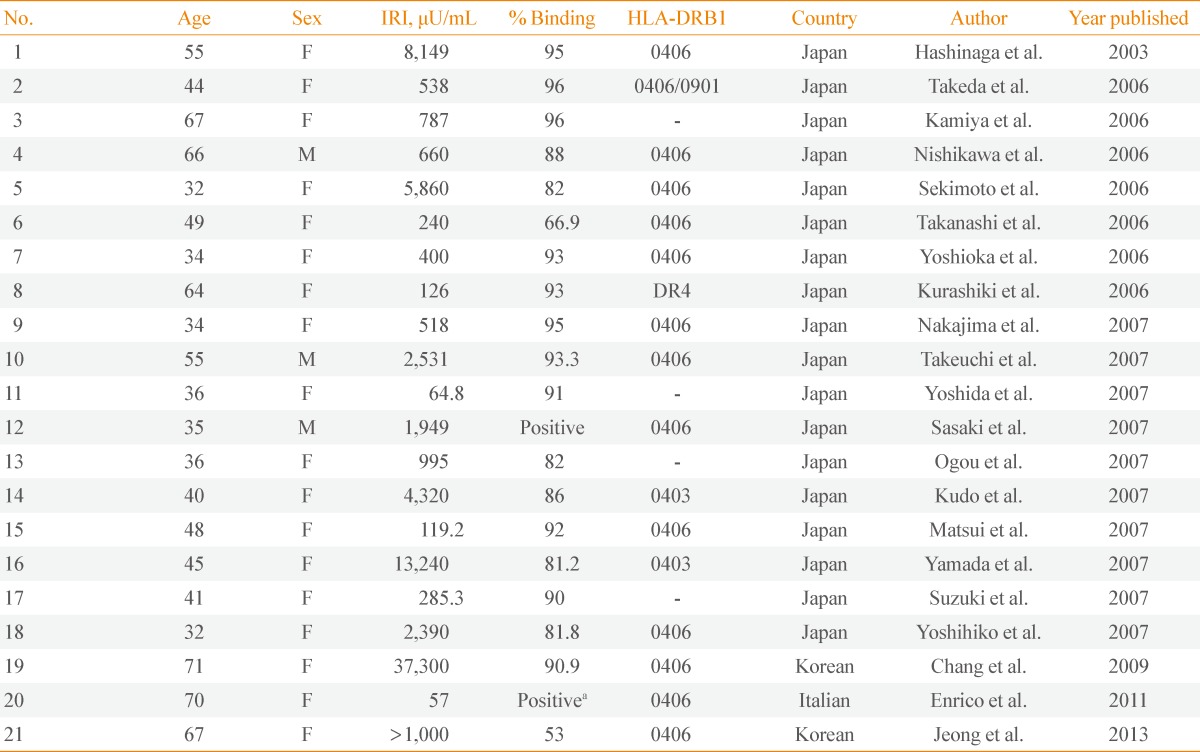
IRI, immunoreactive insulin; HLA, human leukocyte antigen; F, female; M, male.
a210,000 Arbitrary units.
Previously, hypoglycemia due to IAS was mostly observed in patients without diabetes and was easily detected. However, ALA is a compound frequently used for the treatment of peripheral neuropathy in diabetic patients. If a diabetic patient is determined to have hypoglycemia, oral hypoglycemic agent, or exogenous insulin administration is first suspected to be the cause. Therefore, when a diabetic patient presents with IAS following ALA intake, the possibility of ALA-induced hypoglycemia must be considered, otherwise the diagnosis may be delayed or the causative drug may be readministered. In the present case, the patient was instructed to stop taking ALA after being diagnosed with ALA-induced IAS. However, this patient was twice more prescribed ALA and experienced hypoglycemia that continued for several weeks after intake. Among the 21 cases of IAS caused by ALA, this is the only case in which IAS recurred due to repeated administration of ALA. Because Koreans and Japanese individuals significantly express the HLA DR4 allele relevant to IAS [6], if a Korean diabetic patient taking ALA has spontaneous hypoglycemia without any specific cause and has high levels of blood insulin and insulin antibodies, the physician should consider ALA-induced IAS.
In the present case, the serum insulin value when the patient was initially hospitalized was 15.33 µIU/mL before meals and 19.41 µIU/mL after meals, both of which were within the normal range. However, after the second and third occurrences, the serum insulin measured over 1,000 µIU/mL, well above the normal range. The initial serum insulin value was low, possibly because the insulin was measured using RIA. In this method, the antibodies fixed to the test tube may be saturated with insulin when the serum insulin is too dense, and unbound insulin and signal antibodies may be combined, leaving only a small amount of signal antibodies after washing, thus causing an underestimation of the insulin level, referred to as the high-dose hook effect. Namely, the highly concentrated insulin in the blood was assumed to be underestimated due to the hook effect when using RIA during the patient's first hospitalization. This possibility was overlooked at her first presentation, and we could not re-examine diluted sample or measure by other method like ELISA. On the other hand, we used ELISA to measure the insulin level on the second and third examination and confirmed a high insulin concentration in the blood.
A majority of IAS patients (80%) recover from hypoglycemia in 1 to 3 months. However, several patients have reported experiencing hypoglycemia for more than a year. To treat hypoglycemia, increasing the frequency of meals is helpful, but a steroid or α-glucosidase inhibitor may be necessary. Reportedly, azathioprine, 6-mercaptopurine, or plasmapheresis has also used in some cases [10]. In the present case, snack intake between meals and oral steroid administration improved hypoglycemia.
In summary, a 67-year-old female patient with diabetes visited our hospital for diabetic peripheral neuropathy and began taking ALA but experienced hypoglycemia after 2 weeks. Because there was no history of exogenous insulin administration and the serum insulin and insulin autoantibody levels were found to be high, the patient was diagnosed with IAS. The HLA test result was positive for DRB1*0406. She recovered by taking steroids. We advised her to not take ALA; however, she was twice more prescribed ALA at other hospitals to treat her diabetic peripheral neuropathy, which again provoked hypoglycemia. Thus, she revisited our hospital to receive the same treatment as before and recovered both times. Since Koreans have a high incidence of HLA-DRB1*0406-related morbidity, and ALA is a commonly used medicine to treat diabetic peripheral neuropathy, physicians should consider IAS when a diabetic patient taking ALA has hypoglycemia without any specific cause.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Hirata Y, Ishizu H, Ouchi N, Motomura S, Abe M, Hara Y, Wakasugi H, Takahashi I, Sakano H, Tanaka M, Kawano H, Kanesaki T. Insulin autoimmunity in a case of spontaneous hypoglycemia. J Jpn Diabetes Soc. 1970;13:312–320. [Google Scholar]
- 2.Uchigata Y, Hirata Y, Iwamoto Y. Drug-induced insulin autoimmune syndrome. Diabetes Res Clin Pract. 2009;83:e19–e20. doi: 10.1016/j.diabres.2008.10.015. [DOI] [PubMed] [Google Scholar]
- 3.Chang HJ, Choi HS, Park MY, Leem SM, Jang YS, Park KS, Lee JM. A case of insulin autoimmune syndrome related to alpha-lipoic acid. Korean J Med. 2009;76:600–604. [Google Scholar]
- 4.Kim MJ, Shin MS, Kim MK, Lee Y, Kim YU, Shin YG, Chung CH. A case of autoimmune hypoglycemia induced by insulin autoantibody and insulin receptor autoantibody. Diabetes Monit. 2002;3:177–184. [Google Scholar]
- 5.Takeuchi Y, Miyamoto T, Kakizawa T, Shigematsu S, Hashizume K. Insulin autoimmune syndrome possibly caused by alpha lipoic acid. Intern Med. 2007;46:237–239. doi: 10.2169/internalmedicine.46.1893. [DOI] [PubMed] [Google Scholar]
- 6.Uchigata Y, Kuwata S, Tokunaga K, Eguchi Y, Takayama-Hasumi S, Miyamoto M, Omori Y, Juji T, Hirata Y. Strong association of insulin autoimmune syndrome with HLA-DR4. Lancet. 1992;339:393–394. doi: 10.1016/0140-6736(92)90080-m. [DOI] [PubMed] [Google Scholar]
- 7.Uchigata Y. The novel agent, alpha lipoic acid, can cause the development of insulin autoimmune syndrome. Intern Med. 2007;46:1321–1322. doi: 10.2169/internalmedicine.46.0221. [DOI] [PubMed] [Google Scholar]
- 8.Uchigata Y, Hirata Y, Iwamoto Y. Insulin autoimmune syndrome (Hirata disease): epidemiology in Asia, including Japan. Diabetol Int. 2010;1:21–25. [Google Scholar]
- 9.Bresciani E, Bussi A, Bazzigaluppi E, Balestrieri G. Insulin autoimmune syndrome induced by alpha-lipoic acid in a Caucasian woman: case report. Diabetes Care. 2011;34:e146. doi: 10.2337/dc11-0600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dozio N, Scavini M, Beretta A, Sarugeri E, Sartori S, Belloni C, Dosio F, Savi A, Fazio F, Sodoyez JC, Pozza G. Imaging of the buffering effect of insulin antibodies in the autoimmune hypoglycemic syndrome. J Clin Endocrinol Metab. 1998;83:643–648. doi: 10.1210/jcem.83.2.4599. [DOI] [PubMed] [Google Scholar]