

Abstract
Osteochondromas arising from the interosseous border of the distal tibia and involving distal fibula are uncommon. Considering its proximity to the ankle joint, early excision of this deforming distal tibial osteochondroma is done to avoid the future risk of pathological fracture of the distal fibula, ankle deformities and syndesmotic complications. We present a 16-year-old young girl with thinning and deformed distal fibula, secondary to an osteochondroma arising from the distal tibia which was managed with transfibular excision of mass and reconstruction of distal fibula using square nail by shoefields technique.
Keywords: Interosseous osteochondromas, Transfibular excision, Reconstruction, Sofields technique
1. Introduction
Osteochondroma is the most common benign bone tumour commonly arising from the metaphyseal ends of long bones and composed of spongy bone covered by a cartilaginous cap.1 Osteochondromas arising from the interosseous border of distal tibia are rare though reported in literature. Neglected these tumour can cause “mass effect” with plastic deformation of lower end of tibia and fibula, mechanical blocking of joint motion, syndesmotic problems (synostosis or diastasis), varus/valgus deformities of the ankle and subsequent degenerative changes in the ankle.2,3 Thorough removal of the tumour with proper reconstruction of the lower end of fibula is of paramount importance to provide stability and mobility of ankle joint. We present such a case where the distal fibula was reconstructed using Sofield's technique described for osteogenesis imperfecta.4
2. Case presentation
A 16-year-old girl student of average built presented to us with progressively increasing swelling in the outer aspect of right ankle for last two years. Patient also gave history of pain off and on. There was no history of difficulty in walking or restriction of movements at ankle.
There was a globular swelling measuring 6 cm × 5 cm over lateral aspect of right ankle on examination (Fig. 1a,b), bony hard in consistency, smooth with ill defined margins and nontender on palpation. There was no distal neurovascular deficit.
Fig. 1.

a: Clinical photograph of the mass (AP profile). b: Clinical photograph of the mass (lateral profile).
Patient was subjected to anteroposterior and lateral radiography of leg with ankle. Radiography revealed a well defined bony exostosis, arising from the interosseous border of distal tibial metaphysis with thinning, deformity of distal fibula with impending fracture (Fig. 2). The same X-ray also shows a similar dormant lesion involving the fibular head. The patient was initially put in an ankle foot orthosis.
Fig. 2.

AP and lateral X-ray showing the interosseous osteochondroma with thinning, deformed fibula.
The nature and prognosis of the condition was discussed at length with the patient and his family and operative intervention was planned once an informed and written consent was obtained. The patient underwent excision of the osteochondroma through a transfibular approach. Intra-operatively, the fibula was found to be thinned out, lengthened but its cortical shell was intact. The inferior tibio–fibular joint was stable. About 8 cm of this curved fibula was excised followed by complete removal of the tumour mass. Removed fibula was then sectioned and partly excised; the marrow cavity was created using 3 mm K wire. Finally distal reconstruction was done using radius square nail by Sofield's method (Figs. 3 and 4). Stability was checked and would was closed. Histology confirmed the clinical diagnosis of osteochondroma with no malignant transformation.
Fig. 3.
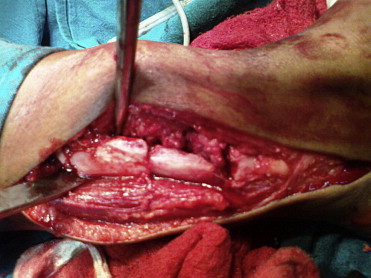
Intraoperative picture after reconstruction of fibula.
Fig. 4.

Post-operative X-ray.
Post-operatively, the patient was mobilised, non-weight bearing in a below knee plaster, for 4weeks. Further mobilisation was undertaken with a gradual transition from partial to full weight bearing. At 1 year follow-up, she had made a complete recovery with full return of ankle functions. The nail had migrated and was thus removed. The fibular osteotomy site had united (Fig. 5a,b). There was no evidence of recurrence and she is still under follow-up.
Fig. 5.

a: Follow-up lateral X-ray showing union of osteotomy. b: Follow-up AP X-ray showing union of osteotomy.
3. Discussion
Osteochondromas are the most common benign bone tumours.1 They probably are developmental malformations rather than true neoplasm and are thought to originate within the periosteum as small cartilaginous nodules.5 They present most often in the second decade of life during the period of rapid skeletal growth. The metaphyses of proximal tibia, distal femur, distal tibia, distal fibula, proximal femur and proximal humerus are the most commonly affected sites, though they can occur at all bony sites.2,3 About 90% of patients have only a single lesion but are multiple in some inherited as autosomal dominance trait with variable penetrance.5 Osteochondromas may be asymptomatic when they are discovered incidentally or present as a mass or bony lump. Progressive enlargement may cause pressure symptoms like nerve compression or skeletal deformity and sometimes may fracture. Malignant transformation to chondrosarcoma is rare (less than 1% in solitary and higher in multiple) and should be suspected in the presence of increasing pain and sudden increase in the size of lesion in patients presenting after skeletal maturity.6
It is shown that fibula shares 10–16% of total load transmission across the ankle joint.7 Whenever tumour excision is contemplated with lower one fourth fibular resections, there is creation of a “void” which adversely affects the stability and functional outcome of the ankle joint. Thus simple resection of the distal fibula without reconstruction of the lateral side of the ankle is obsolete.8 Carrell described the fibular rotational osteotomy where proximal fibula has been sacrificed for reconstruction of ankle joint.9 Many surgeons have successfully used this technique for reconstructing distal fibula and distal radius. Our case was unique where the proximal fibula was also involved. Eger used a long bone graft from the iliac crest for distal fibula reconstruction where the syndesmosis was reconstructed with a periosteal flap in second stage after en bloc excision.10 Johnston et al have lengthened the fibula using the Ilizarov method.11 An allograft construction12 has also been described but such complex surgeries are usually described for malignant cases. An alternative method is an arthrodesis of the tibiotalar joint.13 The disadvantage of this technique is the limited range of motion and the development of a nonunion.
4. Conclusion
This case highlights the need for early excision of the osteochondromas arising from distal aspect of tibia before subsequent fibular and hind-foot deformities arise. We suggest this method worthwhile for treatment of such uncommon lesion.
Conflicts of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1.Schramm G. Pathogenesis of cartilaginous exostoses and enchondromas. Arch Orthop. 1929;27:421. [Google Scholar]
- 2.Chin K.R., Kharazzi F.D., Miller B.S., Mankin H.J., Gebhardt M.C. Osteochondromas of distal aspect of tibia and fibula. Natural history and treatment. J Bone Jt Surg Am. 2000;82(9):1269–1278. doi: 10.2106/00004623-200009000-00007. [DOI] [PubMed] [Google Scholar]
- 3.Spatz D.K., Guille J.T., Kumar S.J. Distal tibiofibular diastasis secondary to osteochondroma in a child. Clin Orthop. 1997;345:195–197. [PubMed] [Google Scholar]
- 4.Sofield H.A., Millar E.A. Fragmentation, realignment, and intramedullary rod fixation of deformities of the long bones in children. J Bone Jt Surg Am. 1959;41:1371–1391. [Google Scholar]
- 5.Canale S.T., Beaty J.H. 11th ed. Mosby; USA: 2007. Campbell's Operative Orthopaedics. [Google Scholar]
- 6.Krieg J.C., Buckwalter J.A., Peterson K.K., El-Khoury G.Y., Robinson R.A. Extensive growth of an osteochondroma in a skeletally mature patient. A case report. J Bone Jt Surg Am. 1995;77(2):269–273. doi: 10.2106/00004623-199502000-00015. [DOI] [PubMed] [Google Scholar]
- 7.Goh J.C., Mech A.M., Lee E.H. Biomechanical study on load bearing characterstics of the fibula and effects of fibular resection. Clin Orthop. 1992;279:223–228. [PubMed] [Google Scholar]
- 8.Mohler D.G., Cunningham D.C. Adamantinoma arising in the distal fibula treated with distal fibulectomy: a case report and review of the literature. Foot Ankle Int. 1997;18:746–751. doi: 10.1177/107110079701801112. [DOI] [PubMed] [Google Scholar]
- 9.Carrell W. Transplantation of fibula in the same leg. J Bone Jt Surg Am. 1938;20:627–634. [Google Scholar]
- 10.Eger W., Schorle C., Zeiler G. Giant cell tumor of the distal fibula: fifteen-year result after en bloc resection and fibula reconstruction. Arch Orthop Trauma Surg. 2004;124:56–59. doi: 10.1007/s00402-003-0562-4. [DOI] [PubMed] [Google Scholar]
- 11.Johnston A.J., Andrews T. Fibular lengthening by Ilizarov method secondary to shortening by osteochondroma of distal tibia. Strategies Trauma Limb Reconstr. 2008 April;3(1):45–48. doi: 10.1007/s11751-007-0028-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lubliner J.A., Robbins H., Lewis M.M., Present D. Aneurysmal bone cyst of the fibula: en bloc resection with allograft reconstruction. Bull Hosp Jt Dis Orthop Inst. 1985;45:80–86. [PubMed] [Google Scholar]
- 13.Pickering R. Arthrodesis of ankle, knee, and hip. In: Pickering R.M., editor. Campbells's Operative Orthopaedics. 10th ed. Mosby; St. Louis: 2003. [Google Scholar]