

Abstract
Nora lesion is a rare benign parosteal osteochondromatous proliferation involving feet and hand. Aggressive features on imaging and confusing results on histopathological studies make its diagnosis difficult. Since the time of its discovery, only few cases have been reported in the literature. Authors report a case of Nora's lesion on the planto-medial aspect of metatarsal head of great toe of left foot. The diagnosis was suspected by imaging characteristic features and was confirmed by histopathology. Treatment was surgical, with complete excision. There are no clinical or radiological signs of recurrence on further review 1 year post-operatively.
Keywords: Nora's lesion, Bizarre osteochondromatous proliferation, Histopathology
1. Introduction
Nora lesion is a rare benign parosteal osteochondromatous proliferation involving feet and hand. It was first described by Nora et al1 in 1983. It grows rapidly and is reported to recur in 50% of the cases following resection.2,3 Aggressive features on imaging and confusing results on histopathological studies make its diagnosis difficult. So, it must be distinguished from malignant lesion like chondrosacroma,2,3 parosteal osteosarcoma1,3 and conventional osteosarcoma1,3 and benign lesions like florid reactive periostitis, myositis ossificans, periosteal chondroma and osteochondroma.4,5 Since the time of its discovery, few cases have been reported in the literature. We report an additional case of Nora's lesion on the planto-medial aspect of metatarsal head of great toe of left foot.
2. Case report
A 37-year-old female presented with a 1 year history of a progressive growing tumor at her left foot; there was no history of trauma.
Clinical examination revealed a non-tender, non-mobile and remarkably hard mass measuring approximately 5 cm × 3 cm, located on the planto-medial aspect of great toe of left foot (Fig. 1). The overlying skin was intact and not adherent; the mobility, sensibility and vascularity of the involved toe were normal.
Fig. 1.

Swelling on the planto-medial aspect of great toe.
Radiographs (Fig. 2a) and computed tomography scan (Fig. 2b) of the left foot showed soft-tissue swelling with calcifications in the planto-medial region on the medial aspect of head of the first metatarsal without cortical irregularity. A diagnosis of ectopic calcification or tumorous lesion was made.
Fig. 2.
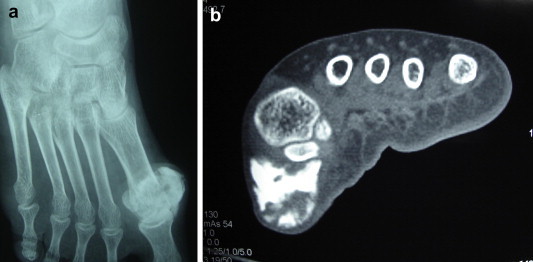
Radiograph (a) and computerized tomography (b) demonstrate the soft tissue swelling with calcification in the plantar-medial aspect of head of first metatarsal.
Routine laboratory determinations were normal. A wide open excision biopsy was performed, through a longitudinal incision on the medial side of the left foot over the first metatarsal bone; the mass was found to be multilobulated with additional portions extending planto-medially to the head of first metatarsal; it was easily removed with the pseudocapsule, as there were no adherence to any of the surrounding bony or soft tissue structures (Fig. 3).
Fig. 3.

Intra-operative showed the multilobulated mass with the pseudocapsule on the planto-medial aspect of first metatarsal.
Histopathological analysis confirmed a disorganized proliferation of fibrous tissue, cartilage and bone, with the cartilaginous component showing irregular groups of enlarged binucleated and ’bizarre’ chondrocytes (Fig. 4).
Fig. 4.

Histopathological analysis confirmed a disorganized proliferation of fibrous tissue, cartilage and bone.
The clinical and histopathological features of the tumor were consistent with a bizarre parosteal osteochondromatous proliferation.
3. Discussion
Bizarre parosteal osteochondroma of bone (first described by Nora et al in 19831 and called Nora's lesion) are rare lesions. The commonest presentation is that of a bony swelling arising from the small bones of the hands and feet mostly occur on the proximal and middle phalanges, metacarpals, and metatarsals. Long bones (commonly of the upper extremity), skull, jaw are the other sites which are rarely involved.2
Nora's lesion occurs in adults in second and third decade of life (average age 30–33 years, range, 2–73). Males and females are equally affected.2,4 There is a history of a mildly painful mass that seems to increase in size over many weeks or a few months. There is usually no history of trauma. There may be stiffness of a nearby joint, or other mechanical symptoms.1,2 Our patient presented with painless swelling.
The cause of Nora's lesions is unknown. It may be related to a reparative process following trauma to the periosteum, as was noted in 30% of cases in the series of Meneses et al.2,6 But there was no history of trauma in our patient.
On plain radiographs these lesions appear to arise from the cortex without affecting it. The lesion is usually located in the metaphysis, and may exhibit a spiculated or irregular surface. Computed tomography scan helps to distinguish it from osteochondromas by showing the absence of continuity between the cortex and medullary cavity of the bone and the lesion.1,2,4
Grossly, the lesion has a nodular surface covered with glistening cartilage with an underlying bony core. Histologically they consist of atypical cartilage with marked proliferative activity resembling Grade I or II chondrosarcoma, disorganized ossification in the cartilage, plenty of irregularly calcified osteoid with benign osteocytes, and actively proliferating but benign fibrous tissue.1,7 The histological feature of our patient is consistent with literature.
It is often confused with malignant lesion like chondrosacroma,2,3 parosteal osteosarcoma1,3 and conventional osteosarcoma1,3 and benign lesions like florid reactive periostitis, myositis ossificans, periosteal chondroma and osteochondroma.4,5 So, good suspicion is always required when benign parosteal osteosarcoma is considered.
The treatment is a simple excision. The recurrence rate is very high. Nora et al1 reported a 51% rate of initial recurrence and a 22% of second recurrence. The majority of the recurrences occurred within 2 years of excision. A wide excision is probably curative. However, there was no recurrence in our case 1 year post-operatively.
Conflicts of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Contributor Information
Sumit Mahajan, Email: mahajan.sumit20@gmail.com.
Rajesh Chandra, Email: rajeshchandra_@hotmail.com.
Yash Mohan Lal, Email: yashorth@yahoo.co.in.
References
- 1.Nora F., Dahlin D., Beabout J. Bizarre parosteal osteochondromatous proliferation of the hands and feet. Am J Surg Pathol. 1983;7:245–250. doi: 10.1097/00000478-198304000-00003. [DOI] [PubMed] [Google Scholar]
- 2.Meneses M.F., Unni K.K., Swee R.G. Bizarre parosteal osteochondromatous proliferation of bone (Nora s lesion) Am J Surg Pathol. 1993;17(7):691–697. doi: 10.1097/00000478-199307000-00006. [DOI] [PubMed] [Google Scholar]
- 3.Smith N.C., Ellis A.M., McCarthy S., McNaught P. Bizarre parosteal osteochondromatous proliferation: a review of 7 cases. Aust N Z J Surg. Oct 1996;66(10):694–697. doi: 10.1111/j.1445-2197.1996.tb00720.x. [DOI] [PubMed] [Google Scholar]
- 4.Resnick D., Kyriakos M., Greenway G.D. Tumors and tumor – like lesions of bone: imaging and pathology of specific lesions. In: Resnick D., editor. Diagnosis of Bone and Joint Disorders. 3rd ed. WB Saunders, Co; Philadelphia: 1995. pp. 3725–3766. 3978, 3979. [Google Scholar]
- 5.Soejima O., Isamaya T., Ogata K. Extensor pollicis longus tendon rupture caused by a bizarre parosteal osteoc hond romatous proliferation of the wrist. J Hand Surg. Dec 1998;3(2):277–281. [Google Scholar]
- 6.Yuen M., Friedman L., Orr W., Cockshott W.P. Proliferative periosteal processes of phalanges: a unitary hypothesis. Skeletal Radiol. 1992;21:301–303. doi: 10.1007/BF00241768. [DOI] [PubMed] [Google Scholar]
- 7.Horiguchi H., Sakane M., Matsui M., Wadano Y. Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) of the foot. Pathol Int. 2001;51:816–823. doi: 10.1046/j.1440-1827.2001.01271.x. [DOI] [PubMed] [Google Scholar]