

Abstract
Background:
Ethical sensitivity is considered as a component of professional competency of nurses. Its effects on improvement of nurses’ ethical performance and the therapeutic relationship between nurses and patients have been reported. However, very limited studies have evaluated ethical sensitivity. Since no previous Iranian research has been conducted in this regard, the present study aimed to review nursing students’ understanding of effective factors on ethical sensitivity.
Materials and Methods:
This qualitative study was performed in Kerman, Iran, during 2009. It used semi-structured individual interviews with eight MSc nursing students to assess their viewpoints. It also included two focus groups. Purposive sampling was continued until data saturation. Data were analyzed using manifest content analysis.
Results:
The students’ understanding of factors influencing ethical sensitivity were summarized in five main themes including individual and spiritual characteristics, education, mutual understanding, internal and external controls, and experience of an immoral act.
Conclusions:
The findings of this study create a unique framework for sensitization of nurses in professional performance. The application of these factors in human resource management is reinforcement of positive aspects and decrease in negative aspects, in education can use for educational objectives setting, and in research can designing studies based on this framework and making related tools. It is noteworthy that presented classification was influenced by students themselves and mentioned to a kind of learning activity by them.
Keywords: Nursing students, professional ethics, qualitative research
INTRODUCTION
Ethical sensitivity is an ability to recognize an ethical theme. It is a process through which an individual realizes moral problems or interprets an ethical position to make an appropriate decision.[1] This interpretative awareness is the first component of moral decision-making. It is necessary for moral judgments, performing ethical behaviors, and other moral components.[2] Understanding the process of ethical sensitivity is of high importance. Being sensitive to ethical criteria is considered as a professional competence for nurses.[3] That is why nursing educational organizations pay attention to this objective in their planning.[4]
Various studies have indicated the effects of ethical sensitivity on improving ethical performance of nurses[5] and enhancing nurse–patient relationships.[6] Previous research has shown that nurses, who are more sensitive to ethical issues, have greater ability to solve moral problems with less moral distress.[7] On the other hand, individuals with no ethical sensitivity are more willing to learn issues related to their job.[8]
According to the available literature, various factors influence the level of moral sensitivity. Weaver and Morse believed that working and being in clinical environment affects the level of moral sensitivity.[9] Kim et al. reported the level of moral sensitivity of nurses as 70%. They suggested that the level of moral sensitivity was related with age and individuals’ attitude toward their profession.[10] A Finnish study found a significant difference between moral judgment of nursing freshmen and seniors. It, therefore, concluded that education level can affect the level of moral sensitivity and accordingly moral judgment of nursing students.[11] Some other studies have been indicative of the effects of educational methods on moral sensitivity. In fact, education with more concrete facts, examples, case studies, and teaching aids will better enhance ethical sensitivity.[12] Using a combination of several teaching methods, instead of one method alone, will also increase the ethical sensitivity of students.[13] Clinical work experience and direct presence at patients’ bedside have also been found to result in higher levels of ethical sensitivity.[13] Contrary to nursing students, medical students have been reported to have high ethical sensitivity during the first year of their presence in hospitals. However, this sensitivity tapers off over time.[14]
Various studies have reported several, and sometimes contrasting, factors to affect the level of ethical sensitivity. Since sociocultural backgrounds of the workplace are known to have certain impacts on ethical sensitivity,[15] greater numbers of studies in different communities will better determine the effective factors on this concept.[9] Despite the importance of ethical sensitivity in clinical practice, very limited, mostly quantitative, studies have evaluated its dimensions and effective factors. Kim et al. considered the findings of previous studies about ethical sensitivity to be limited, superficial, and mostly based on quantitative and objective analyses.[10]
As ethical sensitivity is apparently affected by different cultural conditions and working backgrounds, and its assessment requires a comprehensive and holistic approach which can be obtained by naturalistic methods. On the other hand, the period of education can have an important role in developing ethical sensitivity. Since no previous Iranian studies have reviewed ethical sensitivity and its determinants, this study evaluated nursing students’ understanding of factors influencing ethical sensitivity. We considered Master's students due to their wide spectrum of clinical experiences.
MATERIALS AND METHODS
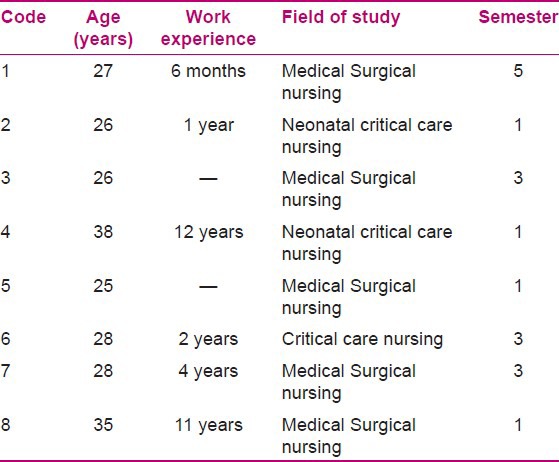
In a qualitative study during 2009 in Kerman (Iran), 8 female MSc nursing students were included [Table 1]. Data were collected through semi-structured interviews with open-ended questions. Polit and Beck believed that this method is a valid method to obtain information from the participants in qualitative studies.[16] Open-ended questions were asked during individual interviews to let the subjects freely express their feelings and thoughts. In order to obtain better understanding and thorough information, follow-up questions were also asked whenever necessary.[17] The interviews were conducted at the Department of Nursing (School of Nursing and Midwifery, Kerman University of Medical Sciences) or the dormitory based on the participants’ preferences. Data collection and data analysis were performed simultaneously.[16]
Table 1.
Characteristics of individual interviewees
In order to collect complementary information, two focus groups were also formed and a number of meetings were held to allow the participants to better describe their experiences and perceptions. The first focus group consisted of three female and five male students (mean age: 27 years). They had a mean work experience of 3 years (range: 0-10 years) and were studying nursing education (n = 2), critical care nursing (n = 3), and neonatal critical care nursing (n = 3). The second focus group included two male critical care nursing students (age: 28 and 30 years, work experience: 5 and 8 years). The subjects discussed the questions that the researchers had prepared in the focus groups. During discussions, the researchers tried to retain the participants’ attention on the main subject and to avoid distractions.
Manifest content analysis was used to analyze the collected data. This method of analysis focuses on human communications and allows the researcher to understand superficial and overt elements of the participants’ words.[18] To perform manifest content analysis according to Bernard's theory,[19] the interviews were immediately transcribed. Afterward, two research team members reviewed the texts separately to better understand their contents. They extracted the units of meaning and wrote them as comments on the original versions of texts. The units of meaning were then summarized and classified based on their similarities. Each category was named considering its manifest content. Naming clarified the subject for the researchers. The next step was to create broader categories and classifications. Finally, five categories were obtained[19] which indicated the students’ understanding of factors influencing ethical sensitivity. During this process, the researchers referred to the data and original texts several times. The categories were also reviewed repeatedly to make sure that the results show the manifest content of the data. Microsoft One Note 2007 was used to organize the categories and classes.
At the beginning of the study, the participants were explained about the confidentiality of data and their right to withdraw at any time. They were then asked to provide written informed consents. The study protocol was approved by the relevant authorities. The participants were allowed to know about the results. In addition, since the participants were nursing students and the interviews could interfere with their academic activities, the time and location of interviews were set according to their preferences.
In order to increase the credibility of the study, the participants were asked to confirm the final data and the emerged themes. Long exposure to the data and maximum variation sampling were also beneficial to the credibility of the study. Moreover, two faculty members who were familiar with qualitative research coded a number of interviews separately. The agreement between their codes was calculated as above 90%. Better auditing of data was ensured by recording all stages of the study, e.g. interviews and methods of analysis, in detail.
RESULTS
After all analyses, five main themes were found to indicate the students’ understanding of factors influencing ethical sensitivity. These themes included individual and spiritual characteristics, education, mutual understanding, internal and external controls, and experience of immoral acts.
Individual and spiritual characteristics
The participants believed that nurses are different from the whole society in terms of some individual characteristics such as morality. According to them, nurses are more sensitive to ethical issues than other people. Individual characteristics such as personality types (law-oriented, decisive, reliable, accurate, able to say “no”), the relevance of individuals’ personality with their profession, emotions, empathy with patients, and interest in profession were mentioned as factors influencing ethical sensitivity. On the other hand, since all participants were Muslim, religious beliefs were also reported to be effective.
“Faith in God is very important,” stated a participant. “Unfortunately, we will not go to patients’ bedside anymore when we are in charge of the shift. In such situations, I wonder if my salary is halal. A lot of other nurses may think about the same things. I always think that even if I do not give a vitamin pill to the patient, I’ll owe him/her.”
Talking about personality, another participant commented, “I am not sure! Maybe it is just my personality. I sometimes think about and feel really sad for people in some parts of Africa. I wish I were a volunteer nurse and helped them. God has fulfilled all my wishes by letting me be a nurse. I have always wanted to help others. It is in my make-up and that is probably why I have learned these aspects of nursing better.”
Education
Most participants considered education as a major factor in ethical sensitivity. They stated that education has the greatest effects at the beginning of each task. Personal characteristics are, therefore, of high importance since they result from primary educations in an individual's life. Repeated education with reminders and warnings will reinforce individuals’ underlying characteristics and increase their awareness. As nursing profession and treatment methods are progressing, constant and updated education on ethics seems indispensable. Awareness needs to be improved in two aspects of professional ethics and professional tasks.
Participant 7 mentioned the effects of increased professional knowledge. “Professional information is really effective. Sometimes, someone really likes to do something but he/she has no information. An outsider would see the person as unscrupulous, but they do not know!” she said.
The participants emphasized that despite the absence of courses on ethics, they had received covert education from the behaviors of their instructors. They thought of these accidental, intangible educations as very influential.
“There was a professor who used to take care of patients’ eyes and stroke them while we were suctioning them. We all liked and learned that,” stated a participant.
On the other hand, patients should be educated about their own rights. Increased knowledge of patients may act as an external control to sensitize the community, and hence the nurses, to ethics. However, education to enhance nurses’ ethical sensitivity is not necessarily formal. In other words, any learning opportunity, like discussing everyday events, can be absolutely beneficial.
Mutual understanding
According to the experiences of nursing students, ethical sensitivity requires relationships with at least one other person. They actually believed that ethical sensitivity results from direct mutual understanding. Nurses will be obliged to follow ethics if they understand the physical and emotional needs of patients through putting themselves in their situation. On the other hand, patients’ understanding of nurses’ situation and trusting how they prioritize the needs of all patients will lead to a calmer environment in which the nurse has enough time to think about more important issues such as ethics.
“Now think they do not possess adequate knowledge and they had not been trained. But would we like such behaviors if we were patients? If we were admitted in another hospital where no one knew us?” stated a participant.
The participants regarded receiving feedback as an effective factor in developing ethical sensitivity. The feedback can be received from patients or their relatives, or even from other nurses and nursing managers. With a more holistic view, it can be given by all members of the society.
A participant stated, “I have no idea! Maybe, again others’ feedback or things such as a mother's gratitude have a positive effect which keeps us from feeling disappointed with everything we do.”
According to the participants, the whole society should also provide such an understanding. To be precise, as mutual understanding can positively affect ethical sensitivity, its absence will result in decreased ethical sensitivity. The subjects believed that in order to establish an appropriate mutual understanding, the society needs to accept nursing as a valuable profession. In their opinion, nurses should not be expected to be sensitive to important communicational aspects such as ethics unless the community has a correct understanding of nursing profession and transfers it to nursing volunteers and students.
“In such a situation, ethics and morality are no longer important. Will someone who does not respect him/herself and whose job is not honored care about morality?” commented a participant.
Internal and external controls
Although rules and regulations cannot entirely control the implementation of ethics, individuals will be more sensitive as long as measures of control exist. The first participant said, “Laws! Firm laws will make us be more sensitive. An example is the patients’ bill of rights which helps people know what is happening to them. It also makes us more sensitive.”
The participants considered rules as a temporary solution to any problem. They believed it can provide authorities with the required opportunity to permanently solve a problem. In addition, while laws should be enforced, individuals have to have law-oriented personalities as well. As the subjects in this study mentioned, external controls are only helpful in combination with internal controls which are more effective, stable, and valid.
“Internal commitment is the first! Ethics can be implemented by the force of rules, but that does not make a moral person. He/she will follow ethics in only one aspect. The tasks can be moral. You may be able to make someone who sits all his/her shift stand, but you cannot wake their conscience. I mean as soon as you remove the law, they would sit again!” said a participant.
EXPERIENCE OF IMMORAL ACTS OR IMMORAL ACTS EXPERIENCE
As the participants highlighted, nursing aims to help vulnerable people. Caring is thus an entirely moral action. An immoral act will impose additional harm on a vulnerable person. Since immoral acts put nurses in turmoil, they try to avoid such actions. Therefore, not only education but also the experience of an immoral act will elevate nurses’ level of knowledge. These experiences are expected to have stable impacts due to their high costs.
“Well, previous experience is so important! For example you might have been in a similar situation in the past. If you had made a wrong decision which caused a bad experience, you will try to decide more wisely this time,” mentioned a participant.
DISCUSSION
This study classified factors affecting ethical sensitivity. It not only paved the way for further studies, but also provided a list for planning measures to educate, promote, facilitate, and develop ethical sensitivity and ultimately develop moral performance of nurses.
Our findings indicated personal and spiritual characteristics, education, mutual understanding, internal and external controls, and experience of immoral acts as the factors affecting ethical sensitivity of nurses. Some personal and spiritual aspects have also been reported by previous research. The effects of religion,[10] personal characteristics, communicational skills,[10,20] and spirituality[21] have been emphasized. Some individuals are more sensitive to ethics due to their attitude toward morality. Such attitude may be formed as a result of various experiences throughout the life. Since ethics have greater effects on spiritual aspects of life rather than its material dimensions, students who believe in spirituality are more sensitive to ethics. In other words, ethical sensitivity leads to moral acts which in turn facilitate moral development.
Kim et al. suggested that ethical sensitivity is influenced by upbringing, culture, religion, education, and life experiences.[10] Weaver and Morse believed that personal characteristics and interpersonal relations are effective on ethical sensitivity.[9] Abbaszadeh et al. reported individual characteristics to be important in nursing students’ viewpoints about their profession.[21] Similarly, our participants considered the same factor as a determinant of ethical sensitivity.
The subjects in the present study considered education, both on various aspects of professional skills and on ethics itself, as an important factor in enhancing ethical qualities and increasing individuals’ knowledge. Likewise, Kim et al. showed that students who had passed training courses in ethics had higher ethical sensitivity.[10] Weaver and Morse announced that professional advancement and higher levels of knowledge and skills will increase ethical sensitivity.[9] Auvinen et al. reported that moral judgment in senior students of nursing was significantly more than in freshmen.[11] Inadequate awareness about ethics can lead to wrong interpretation of respecting other individuals’ rights. Rahmani et al. found misunderstandings about patient rights, i.e. while nurses stated that they respected patients’ right to be independent and thus provided them with enough information to make decisions, patients thought the opposite.[22] The importance of education in ethical sensitivity indicates the necessity of including this subject in nursing curriculum. Apparently, education on ethics is a major prerequisite of ethical sensitivity. Students will only be sensitive to an ethical issue if they have an appropriate understanding of it. Such an understanding is commonly acquired through education. Therefore, a direct relation between ethical awareness of students and their ethical sensitivity is expected.
Mutual understanding was another finding of this study which resulted in different codes. In nursing profession, mutual understanding can be attributed to the socialization process. According our participants, an efficient ethical relation between nurses and patients requires both sides to understand each other. Weaver and Morse emphasized the importance of mutual respect in formation and continuity of ethical sensitivity.[9] Schluter et al. indicated feedback about individuals’ performance to affect their ethical sensitivity. They, however, reported this perception to receive little attention from the organizations. On the other hand, family, coworkers, friends, and physicians had greater shares in supporting nurses.[20]
Kim et al. suggested the impacts of individuals’ attitude toward their job on their ethical sensitivity.[10] Likewise, our participants considered attitude as incredibly important. They stated that the public's viewpoint on different majors will form a person's point of view on his/her profession. Having a positive viewpoint on one's major will in turn increase their ethical sensitivity. The subjects in the present study did not classify this mutual support and understanding. However, each of them had a special experience of inadequate understanding on the part of different people of the community such as patients and their relatives. They greatly emphasized on such experiences. Abbaszadeh et al. found the effects of personal characteristics on the attitudes of individuals toward their field of study.[21] A mutual understanding between nurses and patients will ensure nurses that their decisions and actions are appreciated by the society. They will, therefore, be more sensitive to ethics. After the establishment of a mutual understanding, the nurse will no longer care for the patient as a duty. She/he will instead fully attend to various physical, mental, and spiritual needs of the patient. On the other hand, when the patients and their relatives value the care provided by nurses and understand their problems and concerns, nurses will feel satisfied.
The nursing students in this study believed that internal and external controls were effective on enhancing ethical sensitivity. They mentioned rules as external controls and conscience as the internal control. The majority of participants in a previous research believed that standard policies will cause increased ethical sensitivity.[10] Weaver and Morse emphasized that hospital criteria should not be in conflict with personal moral standards.[9] However, the greater significance of internal controls over external controls was accentuated by our participants. While humans have both individual and collective dimensions, internal controls mostly affect the individual aspect of a person. Since successful nursing requires the cooperation of a large number of individuals, external controls are also of high importance. However, a person's conscience (or internal control) can compensate for the shortcomings of external controls. For instance, in situations when it is impossible to supervise a nurse (such as times caring for a patient with reduced consciousness or working alone), the internal control will force the nurse follow ethics. Despite the higher emphasis on internal controls in the present study, the two types of control are complementary to each other in forming ethical sensitivity.
Among the themes suggested by our participants were experiences of performing or witnessing immoral acts. Kim et al. considered ethical sensitivity to be influenced by life experiences and clinical experience.[10] According to Ersoy and Gündogmus, in the absence of education and adequate information, experience will play a major role in the establishment of ethical sensitivity.[1] Not only experience, but also direct or indirect confrontation with everyday situations (holding positive or negative moral messages) is effective on shaping a nurse's cognitive organization. Since experience is obtained through high costs for patients, nurses, and health systems, it should undoubtedly be considered as a chief factor in developing ethical sensitivity. Therefore, all its aspects should be further examined.
A limitation of this study was evaluating nursing students’ experiences of the theoretical aspect of perception. Obviously, experience of ethical sensitivity can affect other aspects of the students’ professional life which were not included in the present research. Considering the specific geographic and cultural characteristics of the studied population, further research in other nursing education centers is recommended. Moreover, as we only selected postgraduate students, future studies on perceptions of undergraduate and PhD students are necessary.
CONCLUSION
We found a combination of individual and spiritual characteristics, education, socialization, control, and experience to influence ethical sensitivity of nurses. This combination shapes a unique application to sensitize nurses in professional situations. In nursing human resource management, application of this combination in positive and negative reinforcement, education, educational objectives, and research can reveal the practicality of our findings. It is noteworthy that we did not introduce the above-mentioned factors in an isolated list. We actually provided an integrated and correlated collection. Analyzing the systemic relationships of this collection will, therefore, better clarify this issue.
These findings can be used not only in education and sensitization of nursing students, but also in increasing ethical sensitivity of clinical nurses. The latter, however, will require introducing favorable individual and spiritual characteristics, efforts in professional socialization, application of external controls, and reviewing the immoral experiences of nurses.
Footnotes
Source of Support: Shahid Beheshti University of Medical Scienses, Tehran, Iran
Conflict of Interest: None declared.
REFERENCES
- 1.Ersoy N, Gündogmus UN. A study of the ethical sensitivity of physicians in turkey. Nursing Ethics. 2003;10:472–84. doi: 10.1191/0969733003ne6290a. [DOI] [PubMed] [Google Scholar]
- 2.Robertson D, Snarey J, Ousley O, Harenski K, Bowman FD, Gilkey R, et al. The neural processing of moral sensitivity to issues of justice and care. Neuropsychologia. 2007;45:755–66. doi: 10.1016/j.neuropsychologia.2006.08.014. [DOI] [PubMed] [Google Scholar]
- 3.London: RCN; 2002. Royal College of Nursing. Competencies in nursing: A framework for nurses working in specialist palliative care. [Google Scholar]
- 4.Parsons S, Barker PJ, Armstrong AE. The teaching of health care ethics to students of nursing in the UK: A pilot study. Nurse Ethics. 2001;8:45–56. doi: 10.1177/096973300100800106. [DOI] [PubMed] [Google Scholar]
- 5.Lützén K, Dahlquist V, Eriksson S, Norberg A. Developing the concept of moral sensitivity in health care practice. Nurs Ethics. 2006;12:187–96. doi: 10.1191/0969733006ne837oa. [DOI] [PubMed] [Google Scholar]
- 6.Bischko D. The art of nursing: The client-nurse relationship as a therapeutic tool. Nurse Case Manage. 1998;3:148–50. [PubMed] [Google Scholar]
- 7.Corley M. Moral distress of critical care nurses. Am J Crit Care. 1995;4:280–5. [PubMed] [Google Scholar]
- 8.Sayers LS, de Vries K. A concept development of “being sensitive in nursing”. Nurs Ethics. 2008;15:289–303. doi: 10.1177/0969733007088355. [DOI] [PubMed] [Google Scholar]
- 9.Weaver K, Morse AM. Pragmatic utility: Using analytical questions to explore the concept of ethical sensitivity. Res Theory Nurs Pract. 2006;20:191–214. doi: 10.1891/rtnp.20.3.191. [DOI] [PubMed] [Google Scholar]
- 10.Kim YS, Park JW, You MA, Sea YS, Han SS. Sensitivity to ethical issues confronted by Korean hospital staff nurses. Nurs Ethics. 2005;12:595–605. doi: 10.1191/0969733005ne829oa. [DOI] [PubMed] [Google Scholar]
- 11.Auvinen J, Suominen T, Leino-Kilpi H, Helkama K. The development of moral judgment during nursing education in Finland. Nurse Educ Today. 2004;24:538–46. doi: 10.1016/j.nedt.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 12.McPhail K. The other objective of ethics education: Re-humanising the accounting profession:a study of ethics education in law, engineering, medicine and accountancy. J Bus Ethics. 2001;34:279–98. [Google Scholar]
- 13.Weaver K. Ethical sensitivity: State of knowledge and need for future research. Nurs Ethics. 2007;14:141–55. doi: 10.1177/0969733007073694. [DOI] [PubMed] [Google Scholar]
- 14.Patenaude J, Niyonsenga T, Fafard D. Changes in students’ moral development during medical school: A cohort study. CMAJ. 2003;168:840–4. [PMC free article] [PubMed] [Google Scholar]
- 15.Claussen AH, Crittenden PM. Maternal sensitivity. In: Crillenden PM, editor. The organization of attachment relationships: Maturation, culture and context. New York: Cambridge University Press; 2000. pp. 115–22. [Google Scholar]
- 16.Polit DF, Beck CT. 6th ed. Philadelphia: Lippincott Williamsand Wilkins; 2006. Essentials of nursing research, methods, appraisal and utilization. [Google Scholar]
- 17.Salsali M, Parvizi S, Adib Hajbagheri M. Tehran: Boshra LTD; 2003. Qualitative research methods. [Google Scholar]
- 18.Downe-Warm Boldt B. Content analysis method, applications and issues. Health Care Women Int. 1992;13:313–21. doi: 10.1080/07399339209516006. [DOI] [PubMed] [Google Scholar]
- 19.Burnard P. A method of analysis interview transcripts in qualitative research. Nurse Educ Today. 1991;89:461–6. doi: 10.1016/0260-6917(91)90009-y. [DOI] [PubMed] [Google Scholar]
- 20.Schluter J, Winch S, Holzhauser K, Henderson A. nurses’ moral sensitivity and hospital ethical climate: A literature review. Nurs Ethics. 2008;15:304–21. doi: 10.1177/0969733007088357. [DOI] [PubMed] [Google Scholar]
- 21.Abbaszadeh A, Borhani F, Mohsenpour M. Compatibility of personality and major among freshman undergraduate nursing students of the Kerman University of Medical Sciences. Iranian J Nursing Midwifery Res. 2010;15:85–90. [PMC free article] [PubMed] [Google Scholar]
- 22.Rahmani A, Ghahramanian A, Alahbakhshian A. Respecting to patients’ autonomy in viewpoint of nurses and patients in medical-surgical wards. Iranian J Nursing Midwifery Res. 2010;15:14–9. [PMC free article] [PubMed] [Google Scholar]