

Abstract
Patient: Male, 73
Final Diagnosis: Sacrococcygeal chordoma •
Symptoms: Coccycodynia • sacral pain
Medication: —
Clinical Procedure: —
Specialty: Surgery
Objective: Rare disease
Background:
Sacrococcygeal chordomas are rare and difficult to diagnose tumors.
Case Report:
A 73-year-old man in the last 6 months felt a pain in and around the coccyx when sitting and especially when rising from the sitting position. He consulted his family physician and was referred by him to a general surgeon with the diagnosis of pilonidal disease. During the operation, the surgeon found an unusual mass and performed a wedge biopsy of the tumor. When chordoma was returned as the diagnosis, the patient was referred to our tertiary hospital for further treatment. The sacrococcygeal chordoma was excised en bloc with the coccyx and the fifth sacral vertebra by posterior approach.
Conclusions:
Because of minimal response to chemo- and radio-therapy, resections with wide margins at initial surgery is the most important factor influencing local recurrence.
Keywords: sacrococcygeal chordoma, coccygodynia, sacral tumours
Background
Coccygodynia is defined as pain in and around the coccyx; it is a symptom, not a diagnosis. Its cause remains obscure, apart from the cases caused by local injury; rare causes include chordoma, giant cell tumour, intradural Schwannoma, perineural cyst, and intra-osseous lipoma [1–3].
Chordomas are rare, low-grade, slow-growing but locally aggressive primary bone tumors [4]. The most common location is the sacrococcygeal region (40–50%) and the base of the skull (35–40%), followed by the vertebral bodies (15–20%) [5,6]. Their incidence rate is 0.5 per million [7]. Sacrococcygeal chordomas are insidious tumors that are difficult to diagnose; many patients are treated for an assortment of unrelated diagnoses before the correct diagnosis is made [7].
Case Report
The patient was an otherwise healthy 73-year-old Caucasian man who presented himself to his family physician complaining in the last 6 months of tailbone pain felt when sitting and especially when rising from the sitting position. The physician found on examination an area of induration and tenderness along the inner gluteal fold extending into the natal cleft. The primary clinical consideration was pilonidal cyst and thus he was referred to a general surgeon. The surgeon encountered an unusual mass during the operation and decided to perform wedge biopsy. When sacrococcygeal chordoma returned as the diagnosis, the patient was referred to our tertiary cancer hospital for further treatment.
Magnetic resonance images were obtained in axial and sagittal planes using various T1- and T2-weighted sequences. A large, well-defined, lobulated mass was identified at the sacrococcygeal level. Destruction of the coccyx with insinuation into right gluteal musculature was present, along with anterior displacement of the rectum without invasion (Figures 1 and 2). The histopathological report of the wedge biopsy confirmed the diagnosis of sacrococcygeal chordoma.
Figure 1.
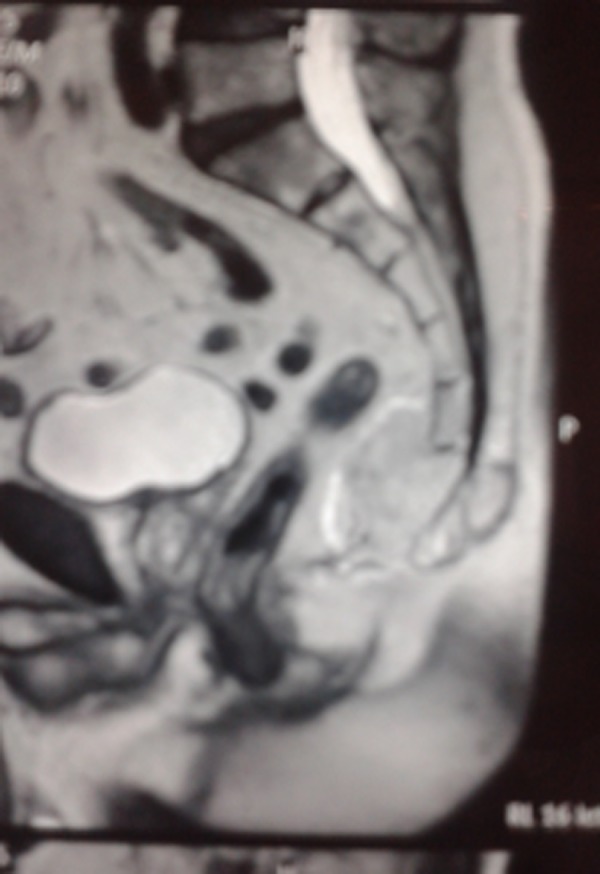
Sagittal magnetic resonance imaging revealing sacral tumour.
Figure 2.

Axial magnetic resonance imaging revealing tumour invading the gluteal muscle.
Hematological and biochemical profiles were within normal limits. Colonoscopy revealed extrinsic pressure on the rectum.
Treatment
The sacrococcygeal sarcoma was excised en bloc with the gluteal musculature, coccyx, and the fifth sacral vertebra. The whole capsule of the tumor was kept intact and at least 2 cm healthy surgical margins were achieved macroscopically. The histopathological report confirmed free surgical margins. The patient recovered uneventfully and was discharged on the 10th postoperative day. He is scheduled for follow-up visits every 4 months and is doing well 28 months after the intervention.
Although chordoma is resistant to the effects of conventional radiotherapy [6,8], our institution combined the use of post-operative high LET (linear energy transfer) radiation with surgery to attempt to increase disease-free intervals.
Discussion
Surgical resection with wide margins at the initial operation is considered the treatment of choice for sacral chordoma because it improves local control and disease-free survival [9–12].
Local recurrence rates of 43% to 85% and metastases rates of 5% to 40% at 1 to 10 years have been reported for sacral chordomas [10–13]. When gluteal invasion is present, the risk of recurrence is reportedly higher and wider margins are important [14]. To obtain wide margins, a combined anteroposterior approach is usually required for proximal tumors, whereas wide resections of distal sacrum chordomas can be performed through a single posterior approach [5,10,15].
Intraoperative contamination is another major issue in sarcoma surgery [16–18]. One study reported a local recurrence of 28% after en bloc resection of chordoma compared with a 64% local recurrence rate when the tumor spilled intraoperatively [17]. Another study suggested intraoperative contamination of muscle and/or sacroiliac joint increased the probability of local recurrence [16].
Considering the above situation, we conclude that effective management of sacrococcygeal chordoma requires early diagnosis, accurate preoperative staging, definitive and adequate surgical resection with proven tumor-free cut margins, and close follow-up.
Conclusions
The most common underlying cause of coccygodynia and mass formation in the natal cleft is pilonidal disease. The 3 characteristic findings that confirm the diagnosis are: 1) abscess or sinus, 2) drainage of fluid (usually purulent), and 3) midline skin pits. In case one or more of them are absent, we should think about the rare causes of the coccygodynia such as chordoma, giant cell tumour, intradural Schwannoma, perineural cyst, and intra-osseous lipoma [19].
Footnotes
Conflict of interest
There is no conflict of interest between the authors.
References:
- 1.Hanelin LG, Sclamberg EL, Bardsley JL. Intra-osseous lipoma of the coccyx. Radiology. 1975;114:343–44. doi: 10.1148/114.2.343. [DOI] [PubMed] [Google Scholar]
- 2.Kinnet JG, Root L. An obscure cause of Coccygodynia. J Bone Joint Surg. 1979;61:299–302. [PubMed] [Google Scholar]
- 3.Ziegler DK, Batnitzky S. Coccygodynia caused by perineural cyst. Neurology. 1984;34:829–30. doi: 10.1212/wnl.34.6.829. [DOI] [PubMed] [Google Scholar]
- 4.Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. doi: 10.3322/canjclin.57.1.43. [DOI] [PubMed] [Google Scholar]
- 5.Dahlin DC, MacCarthy CS. Chordoma: a study of 59 cases. Cancer. 1952;5:1170–78. doi: 10.1002/1097-0142(195211)5:6<1170::aid-cncr2820050613>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 6.Dahlin DC. Bone tumours. 4th ed. Springfield, IL: Charles C Thomas; 1986. pp. 379–93. [Google Scholar]
- 7.Bethke KP, Neifeld JP, Lawrence W., Jr Diagnosis and management of sacrococcygeal chordoma. J Surg Oncol. 1991;48:232–38. doi: 10.1002/jso.2930480405. [DOI] [PubMed] [Google Scholar]
- 8.Dorfman HD, Czerniak B. Bone tumours. 1st ed. St Louis, MO: CV Mosby; 1998. pp. 974–10008. [Google Scholar]
- 9.Ahmed AR. Safety margins in resection of sacral chordoma: analysis of 18 patients. Arch Orthop Trauma Surg. 2009;129:483–87. doi: 10.1007/s00402-008-0674-y. [DOI] [PubMed] [Google Scholar]
- 10.Atalar H, Selek H, Yildiz Y, Saglik Y. Management of sacrococcygeal chordomas. Int Orthop. 2006;30:514–18. doi: 10.1007/s00264-006-0095-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barrati D, Gronchi A, Pennacchioli E, et al. Chordoma: natural history and results in 28 patients treated at a single institution. Ann Surg Oncol. 2003;10:291–96. doi: 10.1245/aso.2003.06.002. [DOI] [PubMed] [Google Scholar]
- 12.Bergh P, Kindblom LG, Gunterberg B, et al. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer, 200. 88:2122–34. doi: 10.1002/(sici)1097-0142(20000501)88:9<2122::aid-cncr19>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- 13.Azzareli A, Quagliuolo V, Cerasoli S, et al. Chordoma; natural history and treatment results in 33 cases. J Surg Oncol. 1988;37:185–91. doi: 10.1002/jso.2930370311. [DOI] [PubMed] [Google Scholar]
- 14.Yonemoto T, Tazezaki S, Takenouchi T, et al. The surgical management of sacrococcygeal chordoma. Cancer. 1999;85:878–83. [PubMed] [Google Scholar]
- 15.Devin C, Chong PY, Holt GE, et al. Level-adjusted perioperative risk of sacral amputations. J Surg Oncol. 2006;94:203–11. doi: 10.1002/jso.20477. [DOI] [PubMed] [Google Scholar]
- 16.Hanna SA, Aston WJ, Bringgs TW, et al. Sacral chordoma: can local recurrence after sacrectomy be predicted? Clin Orthop Relat Res. 2008;466:2217–23. doi: 10.1007/s11999-008-0356-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kaiser T, Pritchard D, Unni KK. Clinicopathologic study of sacrococcygeal chordoma. Cancer. 1984;53:2574–75. doi: 10.1002/1097-0142(19840601)53:11<2574::aid-cncr2820531136>3.0.co;2-5. [DOI] [PubMed] [Google Scholar]
- 18.Virkus WW, Marshall D, Enneking WF, Scarborough MT. The effect of contaminated surgical margins revisited. Clin Orthop Relat Res. 2002;397:89–94. doi: 10.1097/00003086-200204000-00013. [DOI] [PubMed] [Google Scholar]
- 19.Humphries AE, Duncan JE. Evaluation and management of pilonidal disease. Surg Clin North Am. 2010;90:113–24. doi: 10.1016/j.suc.2009.09.006. [DOI] [PubMed] [Google Scholar]