

Abstract
We report the case of a patient with postoperative, hospital-acquired, quadruple-valve endocarditis caused by Enterococcus faecalis on presumed normal native valves. During a cervical laminectomy, the patient had a non-ST-elevation myocardial infarction that was treated conservatively. In the intensive care unit, the patient became febrile and developed a new 2/6 systolic murmur. Blood cultures grew E. faecalis, and the patient was given antibiotics. Postoperative transthoracic echocardiography and transesophageal echocardiography revealed vegetations on all 4 heart valves. Subsequently, the patient was moved to another facility and died. No autopsy was performed.
E. faecalis is the third-most-common cause of bacterial endocarditis overall; however, it is rarely found in multiple-valve, hospital-acquired endocarditis. Although transthoracic echocardiography is a powerful diagnostic tool, transesophageal echocardiography increases the sensitivity and specificity to about 90%. In our patient, the diagnosis of native quadruple-valve endocarditis would not have not been made without the use of transesophageal echocardiography.
Key words: Endocarditis, bacterial/complications/diagnosis; echocardiography, transesophageal; Enterococcus faecalis; heart valves/pathology; nosocomial infections; postoperative complications
An estimated 10,000 to 15,000 new cases of infective endocarditis are diagnosed each year in the United States. Infective endocarditis has increasingly become a disease of the elderly, with a predominance in men. Multiple-valve endocarditis is somewhat uncommon; however, in such cases, the overwhelming majority of etiologic microorganisms are methicillin-sensitive Staphylococcus aureus. 1 We report the case of a patient who had postoperative, hospital-acquired, quadruple-valve endocarditis caused by Enterococcus faecalis on presumed normal valves.
Case Report
In March 2001, a 64-year-old man with a history of Type II diabetes mellitus, chronic renal failure (not on hemodialysis), and hypertension was admitted to our institution with paraparesis. The patient had been in his usual state of health until the sudden onset of symptoms. There was no seizure activity, loss of consciousness, or loss of bowel or bladder continence. The initial vital signs were normal, and the patient was alert and oriented to time, place, person, and situation. The funduscopic examination revealed no abnormalities. The cardiac examination yielded normal results, with no audible murmurs, rubs, or gallops. The neurologic exam revealed lower-extremity strength of 0/5 bilateral and upper-extremity strength of 1/5 bilateral; sensation, including perianal and deep tendon reflexes, remained normal throughout. Results of cranial nerve examination were also noted to be normal. No cutaneus or mucocutaneous lesions were noted.
Admission laboratory values were as follows: white blood count, 17 × 109/L; hemoglobin, 9.2 g/dL; hematocrit, 29.1 mL/dL; and platelets 148 × 109/L. The serum values were sodium, 138 mEq/L; potassium, 5.3 mEq/L; carbon dioxide, 23 mEq/L; blood urea nitrogen, 47 mg/dL; and creatinine, 2.8 mg/dL.
The patient was admitted by the neurosurgical service. A magnetic resonance image of the cervical spine showed C4–5 cord compression with a burst disk herniation. The patient was started on dexamethasone and underwent a cervical spine laminectomy. During the procedure, the patient had a non-ST-elevation myocardial infarction that was treated conservatively. In the intensive care unit, the patient became febrile and developed a new 2/6 systolic murmur. The creatinine level rose to 3.6 mg/dL, and the white blood count increased to 18.3 × 109/L, with 84.4% neutrophils. The chest radiograph showed normal cardiac size with clear lung fields. Blood cultures grew E. faecalis in all culture bottles, in 48 hours. The patient was given gentamicin and vancomycin upon the recommendations of the infectious disease consulting service. The vancomycin was later changed to ampicillin. The patient became afebrile within 3 days.
Transthoracic echocardiography performed 2 days after surgery showed a 1- × 1-cm mass on the anterior mitral valve leaflet. Within a week, transesophageal echocardiography was performed, revealing a 2- × 1.4-cm multiple-lobed mass on the mitral valve (Figs. 1 and 2), multiple vegetations on the tricuspid valve (Fig. 3), 2 mobile strands on the pulmonic valve, a 2-mm strand on the surface of the aortic right cusp (Fig. 4), and pulmonary valve regurgitation (Fig. 5). The patient had vegetations on all 4 valves.
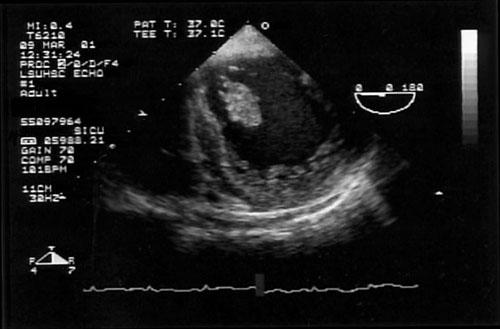
Fig. 1 Transesophageal echocardiographic image of a significant oscillating mass on the mitral valve.
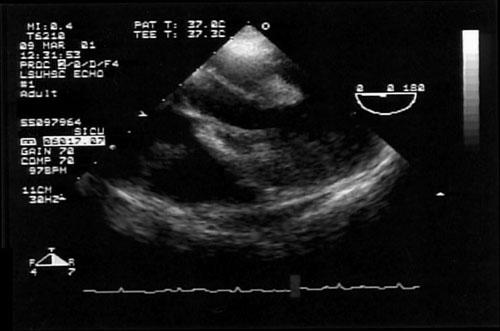
Fig. 2 Diagnostic image of a large mitral valve vegetation on transesophageal echocardiography.

Fig. 3 Transesophageal echocardiogram shows small vegetations on the tricuspid valve.
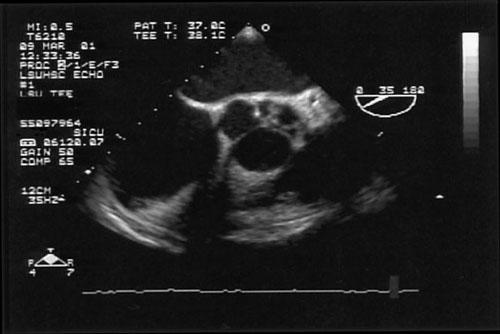
Fig. 4 Transesophageal echocardiographic image of masses on the aortic valve.
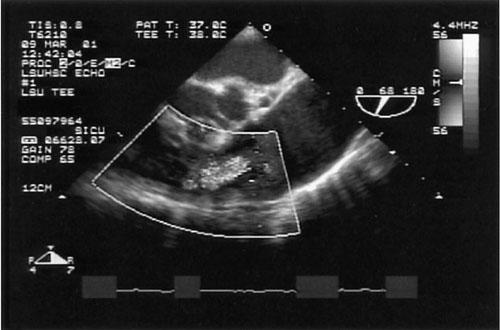
Fig. 5 Transesophageal echocardiographic image shows pulmonary valve regurgitation.
The patient died after he was transferred to another facility; an autopsy was not performed.
Discussion
Hospital-acquired or hospital-associated native valve endocarditis is nearly always caused by staphylococci, usually S. aureus or coagulase-negative staphylococcus. 2 In a case review series, the most common organisms found in multiple-valve endocarditis were S. aureus and Streptococcus viridans. 1 Although E. faecalis is the third-most-common cause of bacterial endocarditis overall, it is rarely found in multiple-valve, hospital-acquired endocarditis.
In a recent case series of multiple-valve endocarditis, only one of 39 patients had enterococcus. This infection occurred during the postoperative period. 1 Another case series found surgery to be a risk factor for enterococcal endocarditis. However, the types of surgery noted were dental, cardiovascular, and abdominal—not neurological, as in our patient. 3
Although uncommon, cases of quadruple-valve endocarditis have been reported. 4,5 To our knowledge, these cases have not involved E. faecalis in a post-neurosurgical patient. It is important to note that small vegetations referred to as nonbacterial thrombotic endocarditis occur when there is turbulent flow across a valve or a high-flow septal defect. It is likely, but not proved, that the 4 valves were infected in this patient.
Although clinical diagnosis with a complete history, physical examination, appropriate laboratory tests, and transthoracic echocardiography (TTE) are mandatory, the use of transesophageal echocardiography (TEE) is extremely helpful when the TTE images are not optimal. The Duke criteria do not specifically mandate TEE for the clinical diagnosis of endocarditis. 6 A finding of multiple-valve lesions by any means enables the identification of patients who are at higher risk of complications, which, in turn, increases the ability to optimally manage the patient. One complication of endocarditis is heart failure, which is more common in patients who have multiple-valve endocarditis. 1 Identification of multiple valve involvement adds to the ability to optimally manage the patient.
Although TTE is a powerful tool that enables risk stratification, vegetation identification, valvular function evaluation, and close examination of prosthetic valves, TEE has a greater sensitivity due to superior image quality. 7 The use of TEE increases sensitivity and specificity to about 90%. 8 In our patient, the diagnosis of native 4-valve endocarditis would not have been made without TEE.
Summary
We have presented herein the case of a patient who had hospital-acquired, quadruple-valve endocarditis caused by E. faecalis. Of interest is not only the rarity of the microbiologic origin but also the method of diagnosis: the quadruple-valve endocarditis would not have been found without TEE. Knowledge of the causative infectious agent and the location of the vegetations allowed optimal clinical management. Nonetheless, multiple-valve endocarditis adversely affects the prognosis of the patient. In this case, the patient died after leaving our institution.
To our knowledge, this is the 1st reported case of quadruple-valve endocarditis due to E. faecalis. Transesophageal echocardiography is an indispensable tool for diagnosing the extent of valvular involvement in patients with endocarditis and for determining the optimal clinical management.
Footnotes
Address for reprints: Patrick R. Krake, MD, Department of Cardiology, LSUHSC-Shreveport, 1501 Kings Highway, Shreveport, LA 71130
E-mail: pkrake@hotmail.com
References
- 1.Kim N, Lazar JM, Cunha BA, Laio W, Minnaganti V. Multi-valvular endocarditis. Clin Microbiol Infect 2000;6:207–12. [DOI] [PubMed]
- 2.Eykyn SJ. Endocarditis: basics. Heart 2001;86:476–80. [DOI] [PMC free article] [PubMed]
- 3.Hricak V Jr, Kovacik, J, Marx P, Fischer V, Krcmery V Jr. Endocarditis due to Enterococcus faecalis: risk factors and outcome in twenty-one cases from a five year national survey. Scand J Infect Dis 1998;30:540–1. [DOI] [PubMed]
- 4.Farrer W. Four-valve endocarditis caused by corynebacterium CDC group I1. South Med J 1987;80:923–5. [DOI] [PubMed]
- 5.Hobbs RD, Downing SE, Andriole VT. Four-valve polymicrobial endocarditis caused by Pseudomonas aeruginosa and Serratia marcescens. Am J Med 1982;72:164–8. [DOI] [PubMed]
- 6.Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med 1994;96:200–9. [DOI] [PubMed]
- 7.Kemp WE Jr, Citrin B, Byrd BF 3rd. Echocardiography in infective endocarditis. South Med J 1999:92:744–54. [PubMed]
- 8.Flachskampf F, Daniel WG. Role of transesophageal echocardiography in infective endocarditis. Heart 2000;84:3–4. [DOI] [PMC free article] [PubMed]