

Abstract
This study explored the association between area-level primary dental care performance and area-level demographics, dental treatment need, and health care service indicators. An ecological cross-sectional study was performed in Belo Horizonte, Brazil, in 2010. The 142 primary health care (PHC) units were grouped based on the following variables: access to individual dental treatment, frequency of dental emergencies, and frequency of individual preventive procedures. The independent variables analyzed were demographic variables, dental treatment need, and health care service indicators. The data were obtained from the information systems of the Brazilian Ministry of Health and the city of Belo Horizonte. We explored the associations between membership in a specific PHC cluster type and the independent variables using multinomial logistic regression with a significance level of 5%. Variables such as the high/very high vulnerability of population, rate of completed treatment, and rate of referrals of users to secondary care were independently associated with the clusters (P < 0.05). The performance of primary dental care services was associated with patient demographics, dental treatment need, and referrals. The results of this study have implications for the planning of public policies.
1. Introduction
Health care system performance is an important issue in public health research to support public policy development. The most recent Behavioral Model of Health Services Use stresses that health service use is best understood by focusing on contextual and individual determinants. A range of contextual variables, such as demographic, social, organizational, and population health indices, could be correlated with the process of medical care and use of services [1].
International studies and nationwide studies in Brazil have been conducted to identify the relationships between social and economic factors and the performance of dental services [2–10]. Despite the importance of group-level variables in epidemiological studies [11], most of these studies are conducted on an individual basis. Several ecological studies have been conducted to analyze the relationships among social and economic conditions, the use and access to dental services [2–4, 6, 7], and the prevalence of oral health conditions [6, 7, 12–14]. However, these studies did not analyze intramunicipal differences. There is a lack of ecological studies that assess the factors associated with the performance of primary oral health care in large cities, especially in Brazil. One study, conducted in London, revealed that children and adolescents living in more socially vulnerable neighborhoods had less access to dental services. Access for adults in the same city was directly proportional to the vulnerability of the area [9].
The Brazilian Health System (acronym SUS), a publicly funded health care system, provides universal access and comprehensive care, including oral health care. Although this program has ensured high levels of access to health services for most of the population, the reduction of the social exclusion of specific subgroups remains a challenge to the SUS [15]. To reduce the social inequality in Brazil, health care managers and personnel need to plan their actions based on evaluations of the health status of the population [16] at the local, municipal, state, and federal levels. The assessment of the health system could provide evidence to support the development of new policies designed to reduce social and economic inequalities in health care [17].
Thus, the purpose of this paper is to explore the association between area-level primary dental care performance and area-level demographics, dental treatment need, and health care service indicators.
2. Methods
An ecological cross-sectional study was performed in Belo Horizonte, Brazil, in 2010. The city of Belo Horizonte is the capital of the state of Minas Gerais, located in southeast Brazil. The city has a population of 2,375,151 inhabitants, and fluoridated water has been available in the city since 1975 (0.60 to 0.85 ppm). Similar to many other Brazilian cities, the city has a serious problem with social inequality; the provision of health services represents a strategy for reducing this disparity. The public health system in Belo Horizonte is composed of 146 primary health care units (PHC) designed as preferential entry points for the population to health services. The PHCs offer a range of services, seeking to provide comprehensive care to individuals and the community. The public health system of Belo Horizonte has adopted a family health strategy to serve populations. In 2010, the system included 539 family health teams (FHTs) and 237 oral health teams (OHTs), as well as other services, which were geographically distributed throughout the city [18, 19]. The FHTs and OHTs are responsible for the care of approximately 75.0% of the city's populations. Each OHT provides preventive, restorative, surgical, and emergency dental treatment to the population in the territory.
We used data from the Brazilian national health information system of the Ministry of Health [20] and from the local health system of Belo Horizonte for 142 HC units with OHTs (participation rate = 97.3%) in 2010. The inclusion criterion for each HC was the presence of an OHT. Thus, our study is a census of HCs with OHTs in a large Brazilian city. Data were extracted from health systems by a single researcher with 10 years of experience in these web environments. The data bank was evaluated for inconsistencies by a senior epidemiologist and a biostatistician for data quality control. In cases of inconsistency, the data in the local (city) database were reevaluated and modified.
The formation of clusters (dependent variable) was based on the similarity of variables of access to individual dental care, access to dental emergencies, and the frequencies of specific preventive dental procedures (Table 1).
Table 1.
Indicators used for cluster formation, Belo Horizonte, 2010.
| Indicators | Description |
|---|---|
| Access to individual dental care | Proportion of residents who receive a scheduled primary dental consultation with the aim of diagnosing and elaborating a preventive/therapeutic plan to address the detected needs, calculated as a percentage of the population registered by the Belo Horizonte Social Census. |
| Frequency of dental emergencies | The indicator was obtained by calculating the percentage of dental emergency consultations in primary health care (i.e., pulpal pain, acute periapical abscess, pericoronitis, periodontal abscess, dental trauma, etc.) relative to the total number of dental consultations in primary health care. |
| Proportion of individual preventive procedures | The indicator was obtained by calculating the percentage of preventive dental procedures (plaque control, fluoride treatment, sealants, dental scaling, patient counseling, and supervised individual brushing) relative to the total number of dental procedures in primary health care (preventive, restorative, and surgical procedures). |
Five different groupings (with two, three, four, five, or six clusters) were formed from the 142 HCs in the city and compared. The three-cluster model was selected to provide a better understanding of the phenomenon (performance of primary dental care). An agglomerative hierarchy technique based on the Ward method was used for the cluster analysis [21].
The explanatory variables analyzed, based on the Behavioral Model of Health Services Use [1], were demographic factors and epidemiological and health care organization indicators.
Demographic indicators were obtained by calculating the percentage of health service users registered with the city council of Belo Horizonte, Brazil, in the following age ranges [22]: younger than ten years, ten to 19 years, 20 to 59 years, and 60 years or older. The health territories that were classified as very high or high health vulnerability by the Health Vulnerability Index (HVI) were combined and defined as areas of high vulnerability. This indicator was developed to determine the degree of social vulnerability of the population of a determined area within a city and to identify priority areas for intervention and resource allocation, thus contributing to planning with the goal of reducing urban inequality. The HVI was created using sociodemographic data (sanitation, housing, education, income, and age of head of family) and health indicators [20, 21].
Based on the WHO criteria for dental caries [23], trained dentists from the OHTs performed examinations to determine dental treatment need (routinely collected data) and rated the need of each individual on a scale from zero to five. This classification is performed to allow the OHT to prioritize the treatment of users with the greatest need for treatment. On this scale, zero indicates individuals without any cavitated carious lesions; one indicates individuals with one to three teeth with cavitated carious lesions; two through four identify patient with more than three teeth with cavitated carious lesions or who require the extraction of remaining dental elements. Individuals with a score of five have controlled decay but require periodontal treatment. This classification is a modification made by council of Belo Horizonte from a previous study [24]. The overall oral health status of the patients of a given HC was determined by calculating the proportion of individuals classified with each of the codes relative to the total number of individuals examined.
The rate of completed dental treatment was calculated as the percentage of examined patients who had received final treatment for each code (according to dental treatment need) relative to the total number of finalized treatments. The indicator of referrals to secondary oral care was calculated as the percentage of referrals made relative to the number of first dental visits. The population covered by FHTs and by OHTs was calculated by dividing the population of a health territory by the total number of teams [22].
Firstly, bivariate multinomial logistic regression models were developed to identify explanatory variables (age, vulnerability, dental treatment need, rate of complete dental dental treatment, population covered by FHTs and by OHTs, and referrals to secondary care) associated with the dependent variable. Each variable with P value lower than 0.20 was included in the multivariate multinomial logistic regression. Explanatory variables with P value lower than 0.05 were maintained in the final model. Adjusted odds ratios (CI 95%) were also calculated. Probabilities predicted by the model for each one of the covariates in the final multivariate model were plotted, keeping the others fixed at their median value. The Wald test was used to assess the statistical significance of these relationships. The data were analyzed using Statistical Package for the Social Sciences (SPSS for Windows, version 18.0 SPSS Inc., Chicago, IL, USA) software.
The study was submitted to and approved by the Ethics Committee for Human Research of the Universidade Federal de Minas and the city of Belo Horizonte (protocol no. 0136.0.203.000-11).
3. Results
We evaluated 142 HCs with OHTs. No data were missing for any variable in any PHC. The primary dental care performance is described in Table 2. Cluster 1 includes PHCs with the highest average proportion of individual preventive dental procedures. PHCs in cluster 2 were associated with the lowest access to individual dental treatment and the highest average proportion of dental emergencies. PHCs from cluster 3 exhibited the lowest average proportion of preventive dental procedures.
Table 2.
Description of primary dental care performance in each cluster, Belo Horizonte, 2010.
| Cluster | Number of PHCs | Average access to individual dental treatment (minimum–maximum) | Average proportion of dental emergencies (minimum–maximum) |
Average proportion of preventive individual procedures (minimum–maximum) |
|---|---|---|---|---|
| 1 (highest preventive care) | 78 | 7.1% (1.8%–24.3%) | 9.5% (1.7%–15.8%) | 66.7% (53.7%–81.6%) |
| 2 (highest emergency care) | 43 | 5.7% (1.0%–12.6%) | 24.2% (16.9%–41.4%) | 62.8% (44.9%–81.6%) |
| 3 (lowest preventive care) | 21 | 7.1% (0.7%–13.4%) | 15.8% (3.4%–37.8%) | 43.4% (28.7%–52.1%) |
The description of median value of each explanatory variable stratified by clusters is presented in Table 3.
Table 3.
Median values of demographic and dental treatment need indicators and health care services indicators in each cluster, Belo Horizonte, 2010.
| Explanatory variables (median values) | Cluster 1 | Cluster 2 | Cluster 3 |
|---|---|---|---|
| High/very high vulnerability | 31.5 | 32.3 | 74.6 |
| <10 years | 9.5 | 9.0 | 10.2 |
| 10 to 19 years | 15.7 | 16.2 | 17.1 |
| 20 to 59 years | 60.5 | 60.3 | 59.9 |
| 60 years and above | 14.2 | 14.1 | 11.2 |
| No teeth with cavities | 16.8 | 12.5 | 17.4 |
| Up to 3 teeth with cavities | 43.5 | 41.9 | 46.2 |
| More than 3 teeth with cavities and/or requiring extraction | 28.6 | 33.6 | 34.5 |
| Necessity of periodontal treatment | 7.2 | 5.9 | 3.5 |
| Completed treatment (no teeth with cavities) |
24.1 | 21.5 | 27.3 |
| Completed treatment (up to 3 teeth with cavities) |
46.9 | 43.7 | 45.1 |
| Completed treatment (more than 3 teeth with cavities and/or requiring extraction) |
18.5 | 24.4 | 27.0 |
| Completed treatment (periodontal treatment) |
5.8 | 4.8 | 3.5 |
| Referral to secondary oral care | 32.5 | 33.7 | 16.0 |
| Population coverage per family health team | 2930.3 | 2936.8 | 2855.7 |
| Population coverage per oral health team | 8075.0 | 8972.5 | 6813.5 |
The final multivariate multinomial logistic regression model is shown in Table 4. The increase of one point in the rate of completed treatment (more than 3 teeth with cavities and/or requiring extraction) increased in 6.1% (CI 95% 2.1–10.2) the odds of pertaining to cluster 2 compared to 1. The increase of one point in the rate of completed treatment (more than 3 teeth with cavities and/or requiring extraction) increased in 5% (CI 95% 0.3–10.0) the odds of pertaining to cluster 3 compared to 1.
Table 4.
Multivariate multinomial logistic regression, Belo Horizonte, 2010.
| Variables | Cluster 2 × Cluster 1 | Cluster 3 × Cluster 1 | ||
|---|---|---|---|---|
| OR (95% CI) | P value | OR (95% CI) | P value | |
| Vulnerability | 1.001 (0.988–1.014) | 0.872 | 1.025 (1.008–1.041) | 0.003 |
| Referrals to secondary care | 1.008 (0.992–1.023) | 0.333 | 0.971 (0.943–0.999) | 0.045 |
| Completed treatment (more than 3 teeth with cavities and/or requiring extraction) | 1.061 (1.021–1.102) | 0.003 | 1.050 (1.003–1.100) | 0.039 |
The increase of one point in the rate of vulnerability increased in 2.5% (CI 95% 0.8–4.1) the odds of pertaining to cluster 3 compared to 1. Finally, the increase of one point in the rate of referrals to secondary care increased in 0.971 (CI 95% 0.943–0.999) the odds of pertaining to cluster 3 compared to 1; that is, the decrease of one point in the rate of referrals to secondary care increased in 3% the odds of pertaining to cluster 3 compared to 1. No other explanatory variable was associated with the dependent variable. Figures 1, 2, and 3 showed the association between the probabilities of belonging to each cluster according to the rate of vulnerability, referrals to secondary care, and completed treatment.
Figure 1.
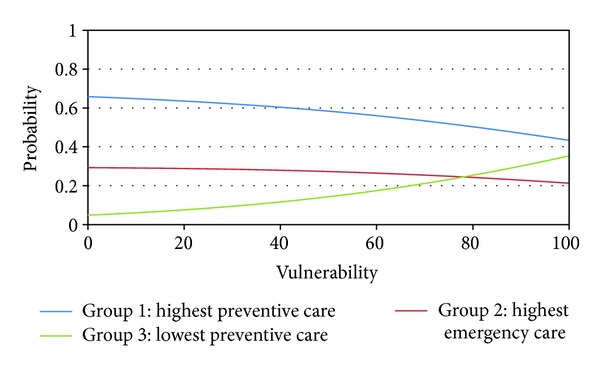
Probability of pertaining to each cluster according to vulnerability in Belo Horizonte, Brazil, 2010.
Figure 2.
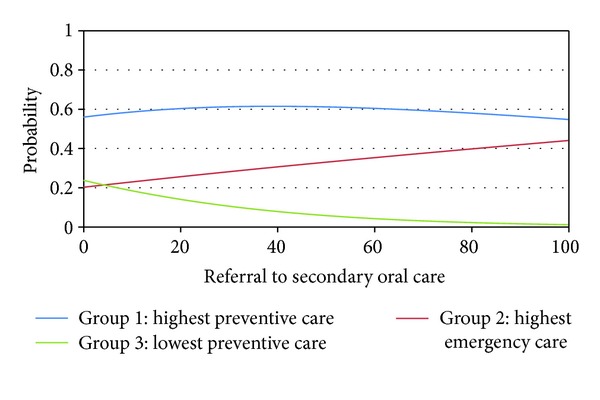
Probability of pertaining to each cluster according to referral to secondary oral care in Belo Horizonte, Brazil, 2010.
Figure 3.
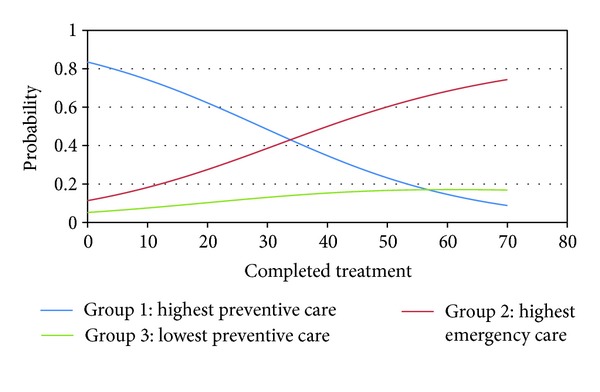
Probability of pertaining to each cluster according to completed treatment (more than 3 teeth with cavities and/or requiring extraction) in Belo Horizonte, Brazil, 2010.
4. Discussion
We found that in the same city there are different PHCs in terms of performance of primary care services. Some demographic, epidemiological, and health care organization indicators were associated with this performance.
High proportion of high-vulnerability patients in the PHCs of cluster 3 could explain the low proportion of preventive dental procedures. The proportion of individual preventive procedures is calculated as the number of preventive procedures divided by the total of all clinical procedures (preventive, restorative, and surgeries). Therefore, the less the proportion of preventive procedures, the more the proportion of restorative procedures and surgeries. The PHCs that faced greater social vulnerability challenges performed a greater proportion of restorative procedures and surgeries. In general, populations from more vulnerable areas had a greater need for restorative and surgical dental procedures as a result of poor access to preventative dental care [25]. As such, more vulnerable populations may indeed require more of a health team's time to address more immediate needs, such as pain or the restoration of impaired teeth. It is possible that the OHTs in cluster 3 prioritized the treatment of these conditions to the detriment of procedures aimed at disease prevention. The results of the present study inspire a reflection on the equity of dental care. There is a tendency to favor equity in the organization of health services in this large Brazilian city. Additionally, our results suggest that the dental services in the city are aimed at reducing inequality between population groups through the implementation of procedures that are appropriately targeted to the local needs (in this case, restorative and surgical procedures) and through providing services in socially disadvantaged areas. On the other hand, we found that these socially vulnerable populations tend to have fewer resources aimed at the prevention of disease. Considering that these procedures are also important for oral health and oral health quality of life, these results seem to reflect the law of inverse care. The law of inverse care tends to prevail in less equal societies, with better access to health services in populations with more favorable social conditions [26].
The higher rate of completed dental treatment needs identified in the PHCs of cluster 2 and 3 compared to cluster 1could explain their performance of primary dental care services. Services with patients that had greater proportion of decayed and missing teeth are more likely to provide emergency dental services [27, 28] and are less likely to use preventive services. In the same way, high dental treatment needs result in less access to individual dental treatment because the number of dental appointments required for each individual is greater.
In cluster 3, the rate of referrals to secondary oral care is inferior to cluster 1, independent of other explanatory variables. In cluster 3 there was higher rate of completed dental treatment needs (more than 3 teeth with cavities and/or requiring extraction) and higher social vulnerability. It is necessary to investigate the organizational, epidemiological, and/or social characteristics of these PHCs in order to identify the difficulties of referring patients to secondary care. Qualitative research could be useful to investigate this issue.
Other variables in the Behavior Model of Health Services Use were tested. However, no further variables were associated with the performance of primary dental care services. The clusters were homogenous in terms of age group distribution. The population coverage per family health team and per oral health team could in theory affect the performance of the services. However, this indicator had no influence on the primary dental care performance.
In this city, the dental care performance was closely associated with the HVI of the area. The growth of health resources (physical, human, technological, and equipment) in more vulnerable areas may contribute to the implementation of preventive procedures, which will reduce the prevalence of oral disease in the long term.
This study has some limitations that should be addressed. The cross-sectional methodology does not permit the inference of causal relationships. Data for each variable were collected by different public health care providers and reproducibility cannot be accessed. We do not evaluate private dental practice. However, because ecologic studies allow the analysis of the impact of contextual variables, this approach can be of great use, considering the need to evaluate the effects of health policies [29].
Our results also indicate that goals for oral health, even within the same city, should be different. Global oral health goals, objectives, and targets from the WHO indicate the need for a framework at different levels—regional, national, and local [30].
The evaluation of indicators of access to service and the monitoring of oral disease may enhance health interventions by directing additional resources to the areas of greatest need. Ecological studies that evaluate health services in a large, socially diverse city can contribute to the understanding of the effects of inequalities in health care. These studies facilitate the planning of health care services and an improved distribution and allocation of resources in this and other health care systems worldwide.
5. Conclusions
The performance of primary dental care services was associated with patient demographics, dental treatment need, and referrals. The results of this study have implications for the planning of more inclusive public policies.
Conflict of Interests
The authors declare that there is no conflict of interests.
Acknowledgments
The authors are grateful to the Brazilian funding agency Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG). The authors also thank the Pró-reitoria de Pesquisa da Universidade Federal de Minas Gerais for financial assistance. Mauro Henrique Nogueira Guimarães Abreu is a fellow of CNPq.
References
- 1.Andersen RM. National health surveys and the behavioral model of health services use. Medical Care. 2008;46(7):647–653. doi: 10.1097/MLR.0b013e31817a835d. [DOI] [PubMed] [Google Scholar]
- 2.Baldani MH, Almeida ES, Antunes JL. Equity and provision of public dental services in the state of Paraná, Southern Brazil. Revista de Saúde Pública. 2009;43(3):446–454. doi: 10.1590/s0034-89102009000300008. [DOI] [PubMed] [Google Scholar]
- 3.Fernandes LS, Peres MA. Associação entre atenção básica em saúde bucal e indicadores socioeconômicos municipais. Revista de Saúde Pública. 2005;39(6):930–936. doi: 10.1590/s0034-89102005000600010. [DOI] [PubMed] [Google Scholar]
- 4.Fischer TK, Peres KG, Kupek E, Peres MA. Primary dental care indicators: association with socioeconomic status, dental care, water fluoridation and family health program in Southern Brazil. Revista Brasileira de Epidemiologia. 2010;13(1):126–138. doi: 10.1590/s1415-790x2010000100012. [DOI] [PubMed] [Google Scholar]
- 5.Barros AJD, Bertoldi AD. Inequalities in utilization and access to dental services: a nationwide assessment. Ciência & Saude Coletiva. 2002;7(4):709–717. [Google Scholar]
- 6.Antunes JLF, Narvai PC, Nugent ZJ. Measuring inequalities in the distribution of dental caries. Community Dentistry and Oral Epidemiology. 2004;32(1):41–48. doi: 10.1111/j.1600-0528.2004.00125.x. [DOI] [PubMed] [Google Scholar]
- 7.Baldani MH, Vasconcelos AGG, Antunes JLF. Association of the DMFT index with socioeconomic and dental services indicators in the state of Paraná, Brazil. Cadernos de Saúde Pública. 2004;20(1):143–152. doi: 10.1590/s0102-311x2004000100030. [DOI] [PubMed] [Google Scholar]
- 8.Antunes JLF, Peres MA, Frias AC, Crosato EM, Biazevic MGH. Gingival health of adolescents and the utilization of dental services, state of São Paulo, Brazil. Revista de Saúde Pública. 2008;42(2):191–199. doi: 10.1590/s0034-89102008000200002. [DOI] [PubMed] [Google Scholar]
- 9.Gallagher JE, Cooper DJ, Wright D. Deprivation and access to dental care in a socially diverse metropolitan area. Community Dental Health. 2009;26(2):92–98. [PubMed] [Google Scholar]
- 10.Quinn BC, Catalano RA, Felber E. The effect of community-level unemployment on preventive oral health care utilization. Health Services Research. 2009;44(1):162–181. doi: 10.1111/j.1475-6773.2008.00901.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Roux AVD. The study of group-level factors in epidemiology: rethinking variables, study designs, and analytical approaches. Epidemiologic Reviews. 2004;26:104–111. doi: 10.1093/epirev/mxh006. [DOI] [PubMed] [Google Scholar]
- 12.Antunes JLF, Frazão P, Narvai PC, Bispo CM, Pegoretti T. Spatial analysis to identify differentials in dental needs by area-based measures. Community Dentistry and Oral Epidemiology. 2002;30(2):133–142. doi: 10.1034/j.1600-0528.2002.300207.x. [DOI] [PubMed] [Google Scholar]
- 13.Antunes JLF, Peres MA, Mello TRC. Individual and contextual determinants of dental treatment needs of children with primary dentition in Brazil. Ciência & Saúde Coletiva. 2006;11(1):79–87. [Google Scholar]
- 14.Antunes JLF, Peres MA, Mello TRC, Waldman EA. Multilevel assessment of determinants of dental caries experience in Brazil. Community Dentistry and Oral Epidemiology. 2006;34(2):146–152. doi: 10.1111/j.1600-0528.2006.00274.x. [DOI] [PubMed] [Google Scholar]
- 15.Victora CG, Barreto ML, Leal MC, et al. Health conditions and health-policy innovations in Brazil: the way forward. The Lancet. 2011;377(9782):2042–2053. doi: 10.1016/S0140-6736(11)60055-X. [DOI] [PubMed] [Google Scholar]
- 16.Barros SG, Chaves SCL. Use of the outpatient information system (SIA-SUS) to assess oral health activities. Epidemiologia e Serviços de Saúde. 2003;12(1):41–51. [Google Scholar]
- 17.Szwarcwald CL, Souza-Júnior PRB, Damacena GN. Socioeconomic inequalities in the use of outpatient services in Brazil according to health care need: evidence from the World Health Survey. BMC Health Services Research. 2010;10(article 217) doi: 10.1186/1472-6963-10-217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sousa A, Dal Poz MR, Carvalho CL. Monitoring inequalities in the health workforce: the case study of Brazil 1991–2005. PLoS One. 2012;7(3) doi: 10.1371/journal.pone.0033399.e33399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.World Health Organization-WHO. Country cooperation at a glance: Brazil. http://apps.who.int/iris/handle/10665/70263.
- 20.Ministério da Saúde Departamento de Informática do SUS (DATASUS) Sistema de informação da atenção básica. http://www2.datasus.gov.br/SIAB/index.php?area=04.
- 21.Johnson RA, Wichem DW. Applied Multivariate Statistical Analysis. 6th edition. Upper Saddle River, NJ, USA: Pearson Prentice Hall; 2007. [Google Scholar]
- 22.Instituto Brasileiro de Geografia e Estatística (IBGE) Censo demográfico 2000. http://www.ibge.gov.br/censo/
- 23.World Health Organization. Oral Health Surveys Basic Methods. 4th edition. Geneva, Switzerland: WHO; 1997. [Google Scholar]
- 24.Dumont AFS, Salla JT, Vilela MBL, Morais PC, Lucas SD. Rate of dental treatment needs: the case of the Xakriaba Indians. Ciência & Saúde Coletiva. 2008;13(3):1017–1022. doi: 10.1590/s1413-81232008000300024. [DOI] [PubMed] [Google Scholar]
- 25.Telford C, Murray L, Donaldson M, O’Neill C. An analysis examining socio-economic variations in the provision of NHS general dental practitioner care under a fee for service contract among adolescents: Northern Ireland longitudinal study. Community Dentistry and Oral Epidemiology. 2012;40(1):70–79. doi: 10.1111/j.1600-0528.2011.00649.x. [DOI] [PubMed] [Google Scholar]
- 26.Hart JT. The inverse care law. The Lancet. 1971;1(7696):405–412. doi: 10.1016/s0140-6736(71)92410-x. [DOI] [PubMed] [Google Scholar]
- 27.American Academy on Pediatric Dentistry Clinical Affairs Committee, American Academy on Pediatric Dentistry Council on Clinical Affairs Committee on the Adolescent. Guideline on adolescent oral health care. Pediatric Dentistry. 2012;34(supplment 7):137–144. [Google Scholar]
- 28.Carvalho JC, Nieuwenhuysen JPV, D’Hoore W. The decline in dental caries among Belgian children between 1983 and 1998. Community Dentistry and Oral Epidemiology. 2001;29(1):55–61. [PubMed] [Google Scholar]
- 29.Gushi LL, Soares MC, Forni TIB, Vieira V, Wada RS, Sousa MLR. Relationship between dental caries and socio-economic factors in adolescents. Journal of Applied Oral Sciences. 2005;13(3):305–311. doi: 10.1590/s1678-77572005000300019. [DOI] [PubMed] [Google Scholar]
- 30.Hobdell M, Petersen PE, Clarkson J, Johnson N. Global goals for oral health 2020. International Dental Journal. 2003;53(5):285–288. doi: 10.1111/j.1875-595x.2003.tb00761.x. [DOI] [PubMed] [Google Scholar]