

Abstract
Bangladesh is a developing country that is facing many challenges, especially in the health sector. Cancer management is a priority due to the current trend of increased incidence in this region. In this article, the current scenario of cancer in Bangladesh and its management with brief history is outlined. The combined effort of government and private sector is highlighted with the gradual progress in cancer management. Recent introduction of the state-of-the-art facilities and the training facilities for human resource development are also outlined. The existing challenges and cooperation from local NGOs and other overseas sources are also highlighted to provide an insight regarding possible ways to tackle these challenges to ensure a better future.
Keywords: Bangladesh, Cancer, developing country, SFO, development
Introduction
Cancer kills more people globally then tuberculosis, HIV, and malaria combined. In the 1960s, almost 25% of global cancer burden was diagnosed in low-income and lower-middle-income countries. In 2010, nearly 55% of the global cancer burden was found in these countries. By 2030, over 13 million people will die from cancer every year. Almost 9 million (about 70%) of these deaths will be in developing countries.[1] By 2050, at the present growth rate, the chances of contracting cancer in their lifetime for the people living in developing countries will be 50-60%. The cancer rate will increase from 650,000 to 2.2 million per year.[2]
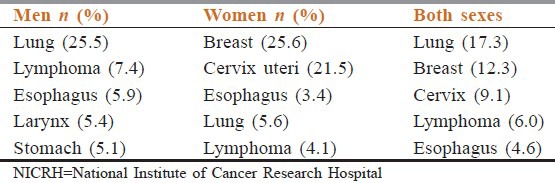
Bangladesh is one of the most densely populated countries of the world with an area of 147,570 km2 (56,977 square miles). According to GLOBOCAN 2008, the 5-year cancer survival prevalence is 291.2 thousand.[3] The number of new cases per year is 141.1 thousand and the number of cancer deaths is 103.3 thousand. New and old cases constitute 124.8 thousand. The top five malignancies are lung, breast, cervix uteri, lip and oral cavity, and esophagus, considering both sexes. Lung cancer tops the list in the case of men and breast cancer tops the list in the case of women.[1]
There is no population-based tumor registry in the country. The numbers and percentages of the top five malignancies in men, women, and both sexes are given in Table 1, as per the annual report 2007 of National Institute of Cancer Research Hospital (NICRH), the only tertiary-level cancer care center of the country.
Table 1.
Top five malignancies attending NICRH in 2007
History
The first teletherapy (cobalt 60) machine was installed at a private hospital named Kumudini Hospital at Mirzapur in 1953. The second cobalt 60 machine was installed at Dhaka Medical College Hospital (DMCH) in 1959. The third radiation therapy center with deep X-ray machine was installed at Chittagong Medical College in 1964. The only tertiary-level cancer hospital of the country, NICRH, was founded in 1981 by Rotary Club of Dhaka as Rotary Cancer Detection Centre. It was handed over to the government in 1986. It started its indoor activities with 50 beds in 1992. The cobalt 60 machine was installed at this center in 1995. The Bangladesh government declared this center as a center of excellence in 2001.[4]
Current Status
NICRH caters to the maximum load of cancer treatment and also contributes in the field of teaching and research. This center is currently functioning with 150-bed capacity equipped with three dual-energy linear accelerators and two cobalt 60 machines, high-dose-rate (HDR) brachytherapy, and standard support equipments. Medical Oncology, Surgical Oncology, and Gynaecological Oncology departments are functioning in this center since 1992. All the standard facilities required for diagnosis and treatment of cancer with a multidisciplinary approach are available at this center.
The various government medical college hospitals situated in different parts of the country as well as the university hospital of Bangabandhu Sheikh Mujib Medical University (BSMMU) at Dhaka have a Radiotherapy/Oncology department, but only nine of them have radiation therapy facilities. Other centers provide only medical oncology service.
A big revolution occurred in the management of cancer when the first linear accelerator was installed at NICRH in 2006. Later, two more government centers (DMCH and Shahid Ziaur Rahman Medical College Hospital, Bogra) were also equipped with dual-energy linear accelerators. Furthermore, there is an older model linear accelerator at Combined Military Hospital (CMH) and at a private oncology center (Delta Oncology Center). Installation of these new machines at government centers initiated the process of transition from two dimentional (2D) to three dimensional conformal radiation therapy (3D CRT).
At present, most of the chemotherapy drugs required to treat cancer are available in the country, including the common monoclonal antibodies used as targeted therapy. Recently, two local pharmaceutical companies (Beacon Pharmaceuticals Limited and Techno Drugs Ltd) started manufacturing the chemotherapy drugs within Bangladesh and have brought the cost of chemotherapy within the reach of general population.
Specialized Surgical Oncology and Gynecological Oncology service is provided by NICRH and BSMMU. Uro-oncology unit under the Department of Urology, which was founded in 2005, is the only super specialty of Surgical Oncology functioning at BSMMU. In other centers, general surgeons and Obstetrics and Gynecology specialists carry out surgical interventions of malignant cases.
Traditionally all the oncologists (around 120 in number) of the country act as clinical oncologists offering both radiation and medical oncology services. The line of demarcation between them remains to be clearly defined in Bangladesh practice.
Hematological malignancies are treated by hematologists and also by radiotherapy oncologists. At present, there are no bone marrow transplant (BMT) facilities existing in the country. The government has proposed to start one BMT at DMCH, the largest government medical college hospital of the country.
The only palliative care center under government management is functioning at BSMMU since 2007 with 18 beds in the inpatient department, in addition to outpatient, home care, and telephone care facilities. At present, this center has started a national training program with the collaboration of Asia Pacific Hospice Palliative Care Network to disseminate the concept of palliative care throughout the country. Few private organizations are also taking some independent initiatives to offer palliative care to cancer patients with limited capacity.
At present, there are two post graduate courses for Radiation Oncology offered in Bangladesh. Under the BSMMU, one can receive Doctor of Medicine (MD) in Radiation Oncology or obtain Fellowship in Radiotherapy from the Bangladesh College of Physicians and Surgeons. There are post graduate courses in Medical Oncology (MD Medical Oncology) and Surgical Oncology (MS Surgical Oncology) offered by the university, and conducted by NICRH.
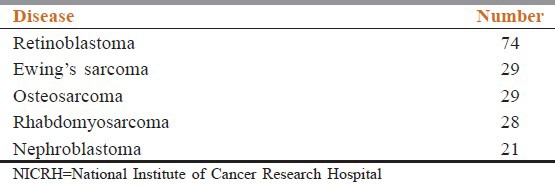
Pediatric cancer patients are treated by pediatric hematology and oncology consultants. In 2012, a total of 3360 adult cancer patients were admitted in NICRH, while the number of pediatric patients was only 471 (12%).[5] The number of patients suffering from top five pediatric cancers attending NICRH in 2012 is shown in Table 2.
Table 2.
Top five paediatric cancer attending NICRH in 2012
There are only 16 qualified pediatric hemato-oncologists in the country. Among them, majority (13) are working at four government centers including NICRH and BSMMU. Pediatric hematology and oncology of BSSMMU started data entry through Pediatric Oncology Network Database (POND).
Besides government facilities, few private centers are also providing cancer care in Bangladesh. Although Kumudini Hospital pioneered the radiation treatment in the country, it could not sustain this facility owing to overwhelming challenges. Another private center named Delta Oncology Centre started its activity at Dhaka in the year 1994. At present, this is the largest private cancer care center in the country having two linear accelerators, two cobalt and two brachytherapy machines (low dose rate (LDR) and HDR) with 350-bed capacity.
In addition, Square Hospital and United Hospital at Dhaka and Khwaja Yunus Ali Medical College Hospital at Sirajganj in northern Bangladesh are also equipped with modern dual-energy linear accelerator. Among them, United Hospital pioneered the first positron emission tomography computed tomography (PET CT) facility with its own cyclotron and claims to be the state-of-the-art cancer center having dual-energy linear accelerator with volumetric arc facility, HDR brachytherapy, and with in-house PET CT facility available.
Few more private centers are coming up with integrated cancer care facilities very soon. These private centers are making modern cancer treatment facilities available within the country, which is permitting a huge number of cancer patients to receive therapy in Bangladesh, whereas in the past, they had to travel abroad for better cancer care. Cancer diagnosis facilities have improved significantly in the past decade. Modern imaging techniques like CT and magnetic resonance imaging (MRI) are available at different district levels both at government and private levels. Tissue diagnosis by fine needle aspiration cytology (FNAC) and histopathology is now possible at divisional area.
Some non-governmental organizations (NGOs) are also involved in cancer care. Ahsania Mission, Cancer Society, Ashic foundation, Digonta Memorial, and Mosabbir Cancer Center are some such examples that are contributing in the field of cancer care with their own initiatives.
Few professional bodies like Oncology Club (Bangladesh Chapter of SAARC Federation of Oncologists), Cancer Society, Bangladesh Society of Radiation Oncologists, Gynae Oncology Society, etc., are also making significant contribution toward improvement of cancer care facilities of the country.
International organizations like International Atomic Energy Agency (IAEA) have been very much supportive in the development of manpower of radiation therapy. They also provided significant support in procuring radiation therapy equipment under their two technical cooperation projects for NICRH and BSMMU.
Some non resident Bangladeshi (NRBs) are playing a significant role in the process of development of cancer care in Bangladesh with their continuous support.
Challenges
The high cost of treatment, lack of adequate radiation facilities, dearth of trained manpower, and lack of awareness within the community are the main challenges impeding cancer care in Bangladesh. Unavailability of trained medical physicist is a significant barrier in the development of radiation treatment facilities in the country.
Conclusion
Bangladesh gave birth to world-renowned oncologists like Emeritus Professor ABMF Karim who was the study chair of European Organization for Research and Treatment of Cancer (EORTC) trial on dose study for low-grade glioma. He was the first person from the South Asian subcontinent to obtain the fellowship from the Royal College of England in radiotherapy. His long profile of success is inspirational for the current oncologists of Bangladesh. At the later stage of his life, he founded the SAARC Federation of Oncologists (SFO) which is now playing a significant role in bringing all the oncologists of SAARC countries together to find a way out to fight against cancer in our own way. With the current trend of development at both government and private sectors, it is assumed that the scenario of cancer management will move to a much more impressive state in the near future.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Noronha V, Tsomo U, Jamshed A, Hai MA, Wattegama S, Baral RP, et al. A fresh look at oncology facts on south central Asia and SAARC countries. South Asian J Cancer. 2012;1:1–4. doi: 10.4103/2278-330X.96489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kumar P, Bhattacharyya GS, Dattatreya S, Malhotra H. Tackling the cancer Tsunami. Indian J Cancer. 2009;46:1–4. doi: 10.4103/0019-509x.48588. [DOI] [PubMed] [Google Scholar]
- 3.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 4.Fighting Cancer in developing countries. IAEA Bulletin. 2010:52–11. [Google Scholar]
- 5.Zaman MM, Baki MO. Cancer Registry Report National Institue of Cancer Reserach and Hospital. 2005-2007:10. [Google Scholar]