

Abstract
Background:
Both stress and prematurity can induce hyperglycemia in the neonatal intensive care unit, which, in turn, is associated with worsened outcomes. Endogenous glucose production (EGP) is the formation of glucose by the body from substrates and contributes to blood glucose (BG) levels. Due to the inherent fragility of the extremely low birth weight (ELBW) neonates, true fasting EGP cannot be explicitly determined, introducing uncertainty into glycemic models that rely on quantifying glucose sources. Stochastic targeting, or STAR, is one such glycemic control framework.
Methods:
A literature review was carried out to gather metabolic and EGP values on preterm infants with a gestational age (GA) <32 weeks and a birth weight (BW) <2 kg. The data were analyzed for EGP trends with BW, GA, BG, plasma insulin, and glucose infusion (GI) rates. Trends were modeled and compared with a literature-derived range of population constant EGP models using clinically validated virtual trials on retrospective clinical data.
Results:
No clear relationship was found for EGP and BW, GA, or plasma insulin. Some evidence of suppression of EGP with increasing GI or BG was seen. Virtual trial results showed that population-constant EGP models fit clinical data best and gave tighter control performance to a target band in virtual trials.
Conclusions:
Variation in EGP cannot easily be quantified, and EGP is sufficiently modeled as a population constant in the neonatal intensive care insulin–nutrition–glucose model. Analysis of the clinical data and fitting error suggests that ELBW hyperglycemic preterm neonates have unsuppressed EGP in the higher range than that seen in literature.
Keywords: endogenous glucose production, extremely preterm infants, glycemic control, insulin therapy, physiological modeling
Introduction
Hyperglycemia, elevated blood glucose (BG) levels, is a common complication of prematurity in neonatal intensive care units (NICUs) and is associated with increased morbidity and mortality,1 worsened outcomes, 2 and increased risk of severe infection 3 and multiple organ failure.4 Conversely, hypoglycemia, a frequent result of insulin therapy,5,6 is associated with negative outcomes and mortality.7
Endogenous glucose production (EGP) is the formation of glucose by the body from substrates and is a physiological function that normally assists in self-regulation of BG levels and the avoidance of hypoglycemia. It encapsulates two main metabolic processes: (1) gluconeogenesis, a metabolic pathway generating glucose from noncarbohydrate carbon substrates, and (2) glycogenolysis, by which the body generates glucose through the breakdown of glycogen to glucose.
Endogenous glucose production can be measured by tracer studies.8–10 However, because of the inherent fragility of the extremely low birth weight (ELBW) cohort, the true fasting rate of EGP cannot be explicitly determined, introducing significant uncertainty to models that rely on its value. Studies measuring unfasted EGP are relatively few, so what literature data there are for similar cohorts must be extrapolated. In addition, interpatient variability has led to significant variation between results and conclusions in these studies.
Stochastic targeting (STAR) is a model-based glycemic control framework for insulin therapy that reduces hyperglycemia and directly quantifies and mitigates the risk of hypoglycemia.11 Model-based glycemic control has been effective in reducing morbidity and mortality. 11–15 Stochastic targeting has also been used in the NICU, where it has proven to be effective at controlling to a target normal range.16 Furthermore, STAR did not increase the incidence of hypoglycemia, 16 as seen in other NICU insulin therapy studies. 5,6
Stochastic targeting uses a time-varying clinically validated model-based insulin sensitivity (SI) to quantify patient variability. 13 Once a current SI is identified using a clinical measurement, forecast SI outcome bounds are generated based on population models. 17–19 These bands allow clinical interventions to be made that best overlap a range of predicted BG outcomes with a target BG range. 11 A treatment can be selected such that the maximum theoretical likelihood of future BG below a clinically specified lower target is 5%. Thus, STAR safely controls BG with a quantified risk of moderate hypoglycemia.
This study aims to quantify variation in EGP for the purposes of improving the performance and safety of STAR glycemic control. An analysis of EGP within the model-based glycemic control framework is augmented by a review and analysis of relevant literature data.
Methods
The analysis utilizes both literature review and clinical data. A literature review was carried out for the purposes of gathering data and examining reported trends. From identified trends, EGP models were created, and their efficacy was analyzed with respect to control outcomes in simulation. EGP population constants based on literature distributions were used to examine the effect of EGP on control in a clinical patient cohort across the entire range of possible EGP values. These methods can be found summarized in fig1.
Figure 1.

Summary of methodological approach.
Literature Review
Inclusion Criteria
A literature search was carried out using search criteria of ‘glucose,’ ‘production,’ ‘preterm,’ and ‘neonate’ in the PubMed database. Studies were excluded if they were associated with maternal or fetal diabetes, subjects were not human, subjects were full-term or older, or studies were unrelated to glucose metabolism. Studies were chosen from the remaining literature on the basis that they reported sufficient data, including the rate of EGP, the current BG, birth weight (BW) <2 kg, gestational age (GA) <32 weeks, and glucose infusion (GI) feed regimes. A total of 177 data points were collected from 21 studies. Study methods and primary conclusions are summarized in tbl1. Endogenous glucose production is shown in fig2 as a function of BG.
Table 1.
Overview of Literature Studies
| Study (first author) | Methods | Study conclusion(s) | |
|---|---|---|---|
| Tracers | Tracer infusion duration | ||
| Hertz20 | [6-6-d2] glucose | Primer dose, 5 min Study period, 4 h |
|
| Sunehag21 | [6-6-d2] glucose | Primer dose, 10 min Study period, 2 h |
|
| Sunehag22 | [6-6-d2] glucose | Primer dose, 5 min Study period, 160–180 min |
|
| Tyrala23 | [6-6-d2] glucose | Primer dose, 1 min Study period, 2 h |
|
| Sunehag24 | [6-6-d2] glucose [2-13C] glycerol | Primed 2 h |
|
| Farrag25 | - | - |
|
| Keshen26 | [U-13C ] glucose | 4 h |
|
| Sunehag27 | U-13C ] glucose [2-13C] glycerol | 10 h |
|
| Sunehag28 | [U-13C ] glucose [2-13C] glycerol | 8 h |
|
| Diderholm29 | [6-6-d2] glucose [2-13C] glycerol | 3.5 h |
|
| Sunehag30 | [U-13C] glucose [2-13C] glycerol [6-6-d2] glucose | 11 h |
|
| Poindexter31 | [6-6-d2] glucose + unlabeled glucose | 3 h |
|
| Sunehag32 | [U-13C] glucose | 8 h |
|
| Sunehag33 | [2-13C] glycerol | 10 h |
|
| Van Kempen34 | [6-6-d2] glucose [2-13C] glycerol | 6 h |
|
| Van Kempen35 | [6-6-d2] glucose [2-13C] glycerol | 6 h baseline (unlabeled) infusion Study period, 3 h |
|
| Van Kempen36 | [6-6-d2] glucose [2-13C] glycerol | 6 h baseline Study period, 1h |
|
| Van Den Akker37 | [U-13C] glucose | 6–7 h |
|
| Van Kempen38 | [6-6-d2] glucose [2-13C] glycerol | 9 h |
|
| Chacko39 | [6-6-d2] glucose | Primer 2H20 Study period, 8 h |
|
| Chacko40 | [U-13C] glucose | 11 h |
|
Figure 2.
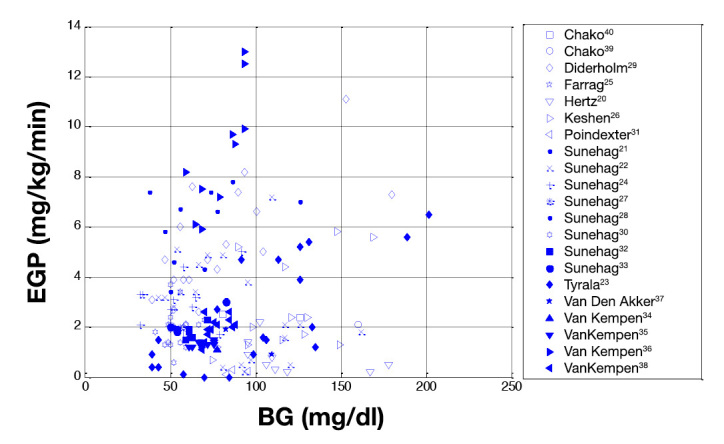
Endogenous glucose production as a function of BG over the literature cohort of 177 data points.
Data Analysis and Trend Generation
Endogenous glucose production was analyzed for trends with respect to BW, GA, GI, and BG. A linear function was then fit using least squares for EGP versus GI, the strongest correlated pair of parameters. A piecewise linear function was also used to describe the suppression of EGP with increasing BG. The piecewise linear model was chosen because of the high variation shown in the data in fig2. It was clear that EGP was often higher at lower BG and lower at higher BG, but no trend or consistent value was evident between these BG levels. Upper and lower limits were chosen as representative of the average EGP response over that glucose range, and linear trend was fit between.
Clinical Data and Model Fit
Clinical Patient Cohort
The clinical patient cohort, see tbl2, consists of data from 21 retrospective patients (25 patient episodes) and 40 patients (8 short-term, 32 long-term, 53 patient episodes total) from prospective BG control studies using STAR. 16,41 Patients who received no insulin or had no BG measurements for greater than 8 hours were separated into different patient episodes. Typically, subsequent patient episodes were separated by more than 24 h.
Table 2.
Clinical Patient Summary Statistics
| Short-term (n = 8) | Long-term (n = 45) | Retrospective (n = 25) | ||||
|---|---|---|---|---|---|---|
| Median | (IQR) | Median | (IQR) | Median | (IQR) | |
| GA at birth (weeks) | 25.6 | (24.9–26.4) | 25.7 | (25.0–28.4)v | 26.6 | (25.4–27.7) |
| Weight at birth (g) | 745 | (681–814) | 770 | (627–972) | 845 | (800–904) |
| Age at start of trial (days) | 6.6 | (3.6–7.7) | 4 | (1.0–10.3) | – |
The median GA and BW of the literature cohort are higher than that of the clinical data but within the interquartile range (IQR). The average BG for the literature data is significantly lower than that of the clinical data, as shown in tbl3.
Table 3.
Summary of Patient Metrics between the Literature Data and Our Clinical Data CohortsCohort medians
| Cohort medians | |||
|---|---|---|---|
| Cohort (first author) | GA (weeks) | BW (g) | BG (mg/dl) |
| Hertz20 | 25.5 | 8900 | 109.8 |
| Sunehag21 | 26 | 796 | 63 |
| Sunehag22 | 27 | 1196 | 86.4 |
| Tyrala23 | Range, 23–28 | Mean, 858 | 101.7 |
| Sunehag24 | 26 | 865 | 55.8 |
| Keshen26 | 28 | 1110 | 117 |
| Sunehag27 | Mean, 27 | Mean, 1020 | Mean, 55.8 |
| Sunehag28 | 27.6 | 1060 | 3.8 |
| Diderholm29 | 28.5 | 1160 | 68.4 |
| Sunehag30 | 27 | 1050 | 50.4 |
| Farrag25 | – | 677 | 70.2 |
| Poindexter31 | 32 | 1500 | 86.4 |
| Sunehag32 | 28 | 1030 | 63 |
| Sunehag33 | 27.5 | 995 | 54 |
| Van Kempen34 | 29.1 | 1140 | 70.2 |
| Van Kempen35 | <32 | Appropriate for GA | 70.2 |
| Van Kempen36 | 30.5 | 1244 | 82.8 |
| Van Den Akker37 | 27.4 | 946 | 97.2 |
| Van Kempen38 | 29.4 | 1335 | 75.6 |
| Chacko39 | Mean, 26.5 | Mean, 955 | Mean, 160.2 |
| Chacko40 | 25.4 | 820 | 73.8 |
| Median literature data (IQR) | 27.5 (26–29) | 1080 (921–1315) | 73.8 (68.4–97.2) |
| Median clinical data (IQR) | 25.9 (25.0–27.0) | 805 (640–930) | 138.4 (126–155) |
| P:-values of median measurements | <0.0001 | <0.0001 | <0.0001 |
Neonatal Intensive Care Insulin–Nutrition–Glucose Model
The clinically validated NICING (neonatal intensive care insulin–nutrition–glucose) model 42 describes glucose–insulin dynamics in the extremely preterm neonate. The model is described by the ordinary differential equations given in Equations (1)–(7). Pictorial representation and parameter origins are given in Appendix A.
The rate of change of BG (G), in mg/dl/min, is defined in Equation 1:
| (1) |
Insulin-mediated glucose clearance is determined by insulin sensitivity (SI), units (liter/mU/min) and non-insulin-mediated uptake includes a clearance term (pG = 0.0030 min -1), including kidney clearance, and a central nervous system (CNS) uptake (CNS = 15.84 mmol/kg/min). ‘Glucose sources include exogenous glucose (Pex(t) [mmol]) and endogenous production (EGP = 5.11 mg/kg/min). mbody is the body mass, and mbrain is the brain mass (approxi-mated as 14% of mbody). The rate of change of plasma (I) and interstitial (Q) insulin (units [mU/liter/min]) are defined in Equations (2)–(4):
| (2) |
| (3) |
| (4) |
Plasma insulin is cleared via the liver (nL = 1/min), the kidney (nK = 0.150/min), and transport into interstitial fluid (nI = 0.003/min). Insulin enters the system exogenously [uex [mU/min]) or endogenously [uen (mU/min)] through pancreatic secretion, as described in Equation (3) (basal secretion IB = 15 mU/liter/min, interstitial transport rate kI = 0.1 min -1). Insulin leaves the interstitial fluid through degradation (nc = 0.003/min).
Appearance of glucose via the enteral route is modeled by two intermediate compartments, the stomach (P1 [mg]) and the gut (P2 [mg]), and is described by Equations (5)–(7):
| (5) |
| (6) |
| (7) |
Transport rates between the stomach and gut and gut and blood (d,1 = 0.0347/min and d2 = 0.0069/min, respectively) are limited to a maximum flux (Pmax [mg/min]). Solutions to Equations (1)–(7) (giving profiles for G,I,Q,P1, and P2) are generated simultaneously in the time domain using a Runga–Kutta 4-based ordinary differential equation solver.
SI is patient specific and time varying, describing a patient’s current metabolic state. It is fit using integral-based fitting methods 43 on a retrospective hour-to-hour basis and assumed constant over an hour-long period. In addition to being a marker of peripheral insulin sensitivity, SI also incorporates uncertainty around patient-specific endogenous insulin and glucose production. A SI of 1 × 10 -7 liter/mU/min, which is very close to zero, represents the lower physiological bound in insulin sensitivity, where no glucose is leaving the blood plasma via the insulin-mediated uptake path.
Fitting Error
Accuracy of model fit to clinical data was one metric used to evaluate the effect of the new EGP models. This fitting error is defined as the average percentage difference between the real and modeled BG levels at BG measurements. When using an integral-based fitting method, 43 the identified SI must remain positive to be physiologically correct; the lower limit of SI was set to a lower limit of 1 × 10 -7 liter/mU/min.
In cases where fitting error was poor, with modeled BG failing to reach clinical measurements, a negative SI had been forced to a lower limited value of 1 × 10 -7 liter/mU/min. In such cases, Equation (1) was rearranged and EGP was then solved under the assumption of SI 1 × 10 -7 liter/mU/min. The resulting EGPmin values gave an indication of the magnitude of minimum EGP required in the NICING model to adequately fit clinical data under the assumption of minimum peripheral insulin sensitivity. These results should thus show the minimum level of interpatient variability.
Control-Based Analysis
Control Performance with Endogenous Glucose Production Models
Modeling EGP as a population constant was examined through the use of a range of EGP values from literature data (tbl2). This range is based on percentiles of the literature data, defined in tbl4. Other EGP values between the median and 95th percentile were included for completeness.
Table 4.
Values of Constant Endogenous Glucose Production Used to Investigate Effect on Control
| Percentile | EGP (mg/kg/min) |
|---|---|
| 5th | 0.29 |
| 25th | 1.40 |
| 50th | 2.1 |
| 75th | 4.6 |
| 95th | 7.7 |
| Currently used: Lin and coauthors19 | 5.11 |
| Other EGP: | 5.50, 6.00, 6.50, 7.00, and 7.50 |
For each EGP value, SI was identified for the whole cohort and a new stochastic model generated. Control was tested using clinically validated virtual trial methods, 13,41 and the control protocol selected insulin such that the predicted outcome likelihood of BG <79 mg/dl (4.4 mmol/liter) was 5%. 44
Control Performance Metrics
Percentage time in band (BG between 72 and 144 mg/dl) evaluated the performance of control, while the number of severe hypoglycemic patients (BG < 47 mg/dl) evaluated safety.
Results
Literature Analysis
Studies have attempted to quantify variability EGP, with mixed results. Gluconeogenesis has been shown to persist in infants receiving total parenteral nutrition (TPN). 39 Endogenous glucose production has been shown to remain unaffected by amino acid administration, 28,31,35 but lipids have been shown to support 33 or enhance EGP. 38 Glycerol has been shown to enhance gluconeogenesis 32 and to be a principal gluconeogenetic substrate. 32,45 Furthermore, the extremely preterm infant is capable of generating glycerol at a rate similar to much larger, term infants. 21,24 Preterm infants have been shown to produce glucose at a rate similar to 21,24 or exceeding 23,26,39 that of term infants, or adults, and there is evidence of some relationship between GA and EGP 39,46 or weight and EGP. 26
Some studies conclude that glucose production has been regulated by BG levels, 9,20 but the majority report the reverse. 39,40,47,48 Preterm infants display varying ability to suppress EGP with increasing GI, with complete, 20 incomplete, 22,34 and failed 39 suppression reported. Although one study suggests that insulin plays an important role in EGP regulation, 22 other studies show that EGP is not suppressed by plasma insulin levels. 21,39,40,47
Endogenous Glucose Production with Respect to Patient Metrics
Comparing reported values of EGP with BW and GA showed little or no correlation in fig3. High interpatient variability between similar patients is seen in the large scatter of EGP across all metrics. Similarly, as shown in fig4:, there is no distinct correlation between BG and EGP or plasma insulin and EGP. Across all literature studies, a suppression of EGP with increasing GI can be seen. However, at any given GI rate, there is significant variation in EGP, with no clear distribution with BW or GA. A piecewise linear trend of GI and EGP from fig4 is defined as follows:
| (8) |
where EGP and GI have units of mg/kg/min.
Figure 3.
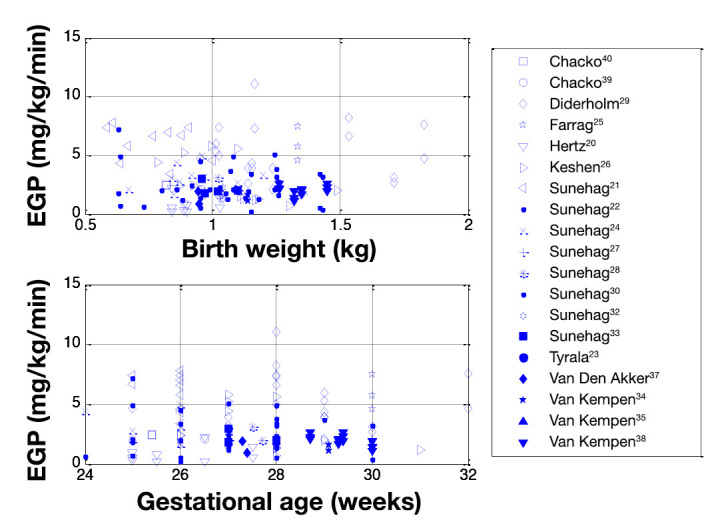
Relationships between EGP with BW and GA.
Figure 4.
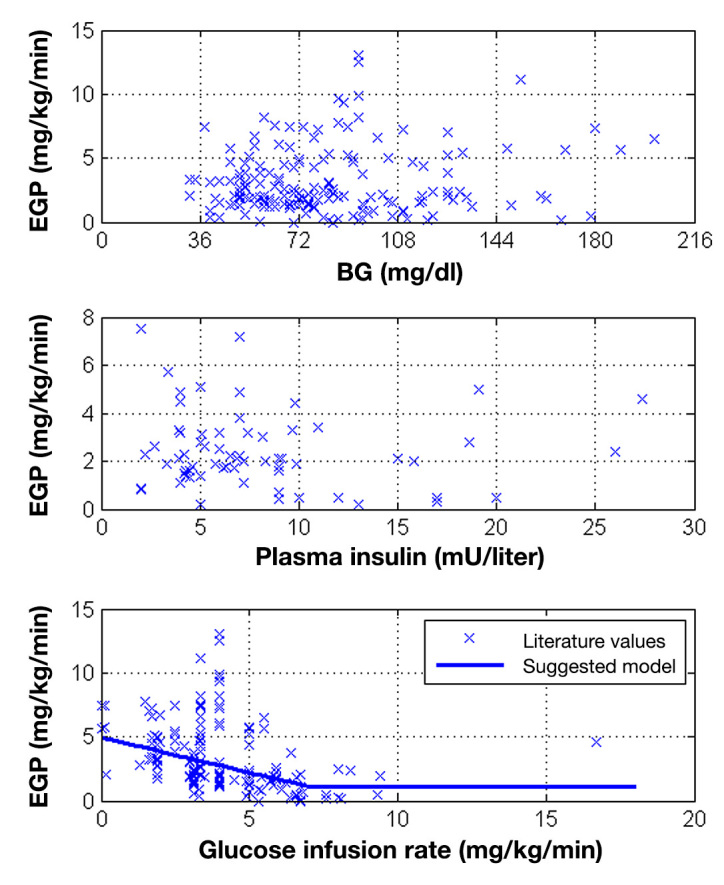
Relationships between EGP and BG, plasma insulin, and GI. Endogenous Glucose Production and Blood Glucose
Endogenous Glucose Production and Blood Glucose
Within the literature, a subcohort of studies show some degree of increase in EGP with BG. These studies are plotted in fig5A, with each study showing a different trend in the magnitude of EGP with respect to BG. All studies show high variation, as reflected in the R2 values from 0.2–0.5. If all the remaining studies are considered, a suppression of EGP with increasing BG can be seen. This suppression exists to varying degrees among and between studies, shown in fig5B
Figure 5.

Subcohorts of studies which show (A) increasing EGP with BG and (B) suppression of EGP with BG.
From Figure 5B, a suppressed EGP with BG can be modeled. The EGP variation with BG is modeled as follows:
| (9) |
Endogenous glucose production has units of mg/kg/min and BG mg/dl. With the suppression of EGP with BG, there was a fitting error of 3.77% over the whole cohort. However, many patients had one or more instances where SI was constrained to a lower limit of SI = 1 × 10 -7 liter/mU/min without fitting the data, indicating insufficient EGP production in the model. To estimate patient-specific EGP over these periods, the EGP was reverse calculated using an assumption of minimum SI, giving EGPmin, as in fig6. These minimum values suggest that EGP in hyperglycemic infants is generally higher than the literature data and not suppressed by elevated BG. EGPmin is also highly scattered across the cohort, with a far wider spread than the literature data.
Figure 6.

Comparison of literature-based model of EGP with BG and EGPmin: estimated from clinical data.
Effect of Endogenous Glucose Production on Control
The fitting and virtual trial control performance metric results for different EGP models are shown in tbl5. Endogenous glucose production as a function of GI and EGP as a function of BG both preformed worse than the currently used constant of EGP = 5.11 mg/kg/min. 19 In the first case, fitting error was increased, and in both cases, the percentage time in band and number of patients with hypoglycemic events increased.
Table 5.
Comparison of Model Fit and Control Performance across Different Endogenous Glucose Production Models
| Case | Fitting | Control | |||
|---|---|---|---|---|---|
| EGP (mg/kg/min) | Fitting error | Time in band (72 – 144 g/dl) | Hyperglycemic (BG > 180 mg/dl) | Mild hypoglycemic (BG < 72 mg/dl) | Severe hypoglycemic (BG < 47 mg/dl) |
| Suppressed EGP (BG) | 2.77% | EGP too low to sustain modeled BG levels, indicating inability of the EGP model to replicate clinical results. | |||
| 0.3 (5th) | 4.78 % | ||||
| 1.40 (25th) | 3.07 % | ||||
| 2.1 (50th) | 2.58 % | 74.8 % | 8.08 % | 2.25 % | 6 |
| 4.20 | 2.16 % | 77.3 % | 7.10 % | 2.05 % | 3 |
| 4.6 (75th) | 2.11% | 78.0 % | 6.69% | 2.05 % | 3 |
| 5.11a | 2.11 % | 78.4 % | 6.52 % | 2.14 % | 2 |
| 5.50 | 2.10 % | 78.6 % | 6.61 % | 2.10 % | 1 |
| 6.00b | 2.09 % | 79.2 % | 6.35 % | 2.23 % | 1 |
| 6.50 | 2.09 % | 79.5 % | 6.42 % | 2.38 % | 2 |
| 7.00 | 2.08 % | 79.8 % | 6.34 % | 2.56 % | 1 |
| 7.50 | 2.08 % | 79.9 % | 6.17 % | 2.67 % | 1 |
| 7.7 (95th) | 2.08% | 80.7% | 5.86% | 2.60% | 1 |
| EGP (GI(t)) | 2.28% | 73.7 % | 8.24 % | 2.1 % | 8 |
Currently in use with EGP = 5.11 mg/kg/min.19
Optimum.
Due to high variation in EGP in Figures1 and 6, a range of constant EGP values were investigated. tbl5 shows that EGP values below 2 mg/kg/min had high fitting error due to insufficient EGP to reach clinically measured BG levels, and during simulation, EGP was insufficient to maintain a positive BG. Increasing EGP decreased fitting error and increased the performance and safety of STAR-model-based glycemic control. However, all fitting errors for EGP >2 mg/kg/min are within measurement error. Thus, compared with BG values in fig1, the current value of EGP = 5.11 mg/kg/min appears reasonable. From a control standpoint, EGP = 6.0 mg/kg/min provides the best compromise across all key metrics in tbl5; however, this improvement is unlikely to be clinically significant.
Discussion
The piecewise linear models of suppressed EGP with increasing BG and EGP with GI resulted in poor fitting and control performance, mainly because EGP values in the literature were too low during hyperglycemia to sustain the BG values measured clinically. These results suggest that hyperglycemic ELBW premature infants often fail to suppress or otherwise regulate EGP with BG or GI, compared with normal infants.
Literature data and EGPmin data points did not overlap, as shown in fig6. The literature BG data was in the normal range, so it is likely that the majority of these infants were healthy and therefore representative of normal EGP dynamics. In contrast, the clinical data are based on hyperglycemic infants, with higher average BG levels, suggesting this cohort is less healthy. This result implies that EGP may be higher in these preterm and hyperglycemic infants, which is physiologically intuitive, as BG is likely high at least in part due to elevated or unsuppressed EGP due to the stress of their condition. These results mimic the adult intensive care unit situation 49,50 and, again, suggest that hyperglycemic infants have less ability to suppress EGP with high BG or GI.
In support of these outcomes, the clinical data patients are typically younger (lower GA), lighter (lower BW), and generally start hyperglycemic, unlike literature data. Clinical data had a median starting BG of 176.4 mg/dl (IQR, 149.4–221.4 mg/dl) compared with the literature median BG of 73.8 mg/dl (IQR, 68.4–97.2 mg/dl). These statistics, summarized in tbl3, reflect a limitation in the use of the literature data to describe EGP model in hyperglycemic ELBW infants. However, no other data for EGP in this cohort exists. Due to the practical difficulty of measuring EGP in this cohort, literature data provides a valid basis for extrapolation.
fig5A suggests that some neonates are at higher BG levels because of a physiological inability to regulate EGP. In the case of deficient EGP, regulation BG is a complex function of EGP, endogenous insulin secretion, insulin therapy, and nutritional treatments. Thus it is extremely difficult to define a direct cause-and-effect relationship between BG and EGP. This is partially reflected in the low R2 values shown in fig5A. Higher EGP with increased BG, as seen in the subcohort of studies in fig5A, was not modeled, as this created a positive feedback system within the simulation software, which inhibited the controller’s ability to regulate BG to a target band.
No strong relationship was found with EGP and BW, plasma insulin, or GA over the entire literature data. Keshen and coauthors 26 have reported decreasing EGP with increasing body weight in babies less than 31 weeks GA and with a postnatal age of 4–9 days, but these data remain unconfirmed by any other literature study and were contradicted by the findings of Chacko and Sunehag 39 in a study with a similar patient cohort. Van Kempen and coauthors 34 have reported that the ability of neonates to maintain basal BG levels with a decrease in exogenous insulin is greater in neonates older than 30 weeks GA, but no studies have specifically investigated EGP over a range of GA, although preterm infant EGP has been shown to be similar or exceed that of term infants. 21,51
As the overall result of this study, we conclude that a population constant of EGP = 5.11 mg/kg/min is adequate for use in control. The population constant model best accounts for and reflects uncertainty due to variability between patients. Increases in controller performance at higher assumed EGP values are unlikely to be clinically significant.
A 2002 study in adults by Tigas and coauthors 52 suggests that using an isotope infusion period of 5 h or longer can reduce error in EGP measurements by at least 80% due to the time required for isotopes and substrates to equilibrate. As a result, some of the studies undertaken before 2002, where infusion periods tend to be shorter than 5 h, may have inherent error in EGP. However, using only literature with an infusion period of 5 h or greater changed none of the trends of EGP and did little to reduce the variation in EGP across all metrics.
With respect to limitations, the CNS glucose uptake is also a population constant based on literature data. It is possible that CNS in this population is lower, which would be reflected in this study as a higher EGP. In addition, a higher EGP term could result from a need for reduced endogenous insulin production. High variability in EGP seen in the literature may also suggest that model dynamics such as CNS and endogenous insulin secretion are not adequately modeled, setting a direction for future work.
Finally, this analysis is only relevant in the context of this model. The model itself has been validated by very successful, safe, and prolonged use in neonates. 16,53 The same model framework and in silico control modeling approach have been validated in adult cases where more independent data are available. 13 Thus, it is felt that the overall results showing enhanced EGP with elevated BG is realistic.
Conclusions
A wide range of literature studies have been found that report EGP. The studies themselves are divided in their conclusions, and no definitive relationship between EGP and BG, plasma insulin, or patient metrics such as weight and GA exists. Over all studies, EGP was shown to be highly variable between patients and studies. Endogenous glucose production was seen to decrease with increasing GI over all literature studies examined. Additionally, two trends were seen with glucose production and BG: the first saw higher EGP at higher BG and the second saw suppression of glucose production at higher BG. Both tends are physiologically reasonable. Stochastic targeted glycemic control was found to perform best when EGP was modeled as a population constant. Results indicate that hyperglycemic ELBW infants produce glucose at a higher rate than healthy counterparts.
Glossary
- (BG)
blood glucose
- (BW)
birth weight
- (CNS)
central nervous system
- (EGP)
endogenous glucose production
- (ELBW)
extremely low birth weight
- (GA)
gestational age
- (GI)
glucose infusion
- (IQR)
interquartile range
- (NICU)
neonatal intensive care unit
- (NICING)
neonatal intensive care insulin–nutrition–glucose
- (STAR)
stochastic targeting
- (TPN)
total parenteral nutrition
Appendix A. Model Parameter Origins

Funding
This work was supported by a University of Canterbury Doctoral Scholarship (Dickson) and the Canterbury Intensive Care Trust.
References
- 1.Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78(12):1471–1478. doi: 10.4065/78.12.1471. [DOI] [PubMed] [Google Scholar]
- 2.McCowen KC, Malhotra A, Bistrian BR. Stress-induced hyperglycemia. Crit Care Clin. 2001;17(1):107–124. doi: 10.1016/s0749-0704(05)70154-8. [DOI] [PubMed] [Google Scholar]
- 3.Bistrian BR. Hyperglycemia and infection: which is the chicken and which is the egg? JPEN J Parenter Enteral Nutr. 2001;25(4):180–181. doi: 10.1177/0148607101025004180. [DOI] [PubMed] [Google Scholar]
- 4.Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359–1367. doi: 10.1056/NEJMoa011300. [DOI] [PubMed] [Google Scholar]
- 5.Beardsall K, Vanhaesebrouck S, Ogilvy-Stuart AL, Vanhole C, Palmer CR, van Weissenbruch M, Midgley P, Thompson M, Thio M, Cornette L, Ossuetta I, Iglesias I, Theyskens C de Jong M, Ahluwalia JS, de Zegher F, Dunger DB. Early insulin therapy in very-low-birth-weight infants. N Engl J Med. 2008;359(18):1873–1884. doi: 10.1056/NEJMoa0803725. [DOI] [PubMed] [Google Scholar]
- 6.Alsweiler JM, Harding JE, Bloomfield FH. Tight glycemic control with insulin in hyperglycemic preterm babies: a randomized controlled trial. Pediatrics. 2012;129(4):639–647. doi: 10.1542/peds.2011-2470. [DOI] [PubMed] [Google Scholar]
- 7.Lucas A, Morley R, Cole TJ. Adverse neurodevelopmental outcome of moderate neonatal hypoglycaemia. BMJ. 1988;297(6659):1304–1308. doi: 10.1136/bmj.297.6659.1304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hovorka R, Shojaee-Moradie F, Carroll PV, Chassin LJ, Gowrie IJ, Jackson NC, Tudor RS, Umpleby AM, Jones RH. Partitioning glucose distribution/transport, disposal, and endogenous production during IVGTT. Am J Physiol Endocrinol Metab. 2002;282(5):E992–E1007. doi: 10.1152/ajpendo.00304.2001. [DOI] [PubMed] [Google Scholar]
- 9.Kalhan SC, Oliven A, King KC, Lucero C. Role of glucose in the regulation of endogenous glucose production in the human newborn. Pediatr Res. 1986;20(1):49–52. doi: 10.1203/00006450-198601000-00013. [DOI] [PubMed] [Google Scholar]
- 10.Vicini P, Sparacino G, Caumo A, Cobelli C. Estimation of endogenous glucose production after a glucose perturbation by nonparametric stochastic deconvolution. Comput Methods Programs Biomed. 1997;52(3):147–156. doi: 10.1016/s0169-2607(96)01784-1. [DOI] [PubMed] [Google Scholar]
- 11.Fisk LM, Le Compte AJ, Shaw GM, Penning S, Desaive T, Chase JG. STAR development and protocol comparison. IEEE Trans Biomed Eng. 2012;59(12):3357–64. doi: 10.1109/TBME.2012.2214384. [DOI] [PubMed] [Google Scholar]
- 12.Chase JG, Shaw G, Le Compte A, Lonergan T, Willacy M, Wong XW, Lin J, Lotz T, Lee D, Hann C. Implementation and evaluation of the SPRINT protocol for tight glycaemic control in critically ill patients: a clinical practice change. Crit Care. 2008;12(2):R49. doi: 10.1186/cc6868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chase JG, Suhaimi F, Penning S, Preiser JC, Le Compte AJ, Lin J, Pretty CG, Shaw GM, Moorhead KT, Desaive T. Validation of a model-based virtual trials method for tight glycemic control in intensive care. Biomed Eng Online. 2010;9:84. doi: 10.1186/1475-925X-9-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Evans A, Shaw GM, Le Compte A, Tan CS, Ward L, Steel J, Pretty CG, Pfeifer L, Penning S, Suhaimi F, Signal M, Desaive T, Chase JG. Pilot proof of concept clinical trials of Stochastic Targeted (STAR) glycemic control. Ann Intensive Care. 2011;1:38. doi: 10.1186/2110-5820-1-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chase JG, Pretty CG, Pfeifer L, Shaw GM, Preiser JC, Le Compte AJ, Lin J, Hewett D, Moorhead KT, Desaive T. Organ failure and tight glycemic control in the SPRINT study. Crit Care. 2010;14(4):R154. doi: 10.1186/cc9224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Le Compte AJ, Lynn AM, Lin J, Pretty CG, Shaw GM, Chase JG. Pilot study of a model-based approach to blood glucose control in very-low-birthweight neonates. BMC Pediatr. 2012;12:117. doi: 10.1186/1471-2431-12-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Le Compte AJ, Lee DS, Chase JG, Lin J, Lynn A, Shaw GM. Blood glucose prediction using stochastic modeling in neonatal intensive care. IEEE Trans Biomed Eng. 2010;57(3):509–518. doi: 10.1109/TBME.2009.2035517. [DOI] [PubMed] [Google Scholar]
- 18.Lin J, Lee D, Chase JG, Shaw GM, Le Compte A, Lotz T, Wong J, Lonergan T, Hann CE. Stochastic modelling of insulin sensitivity and adaptive glycemic control for critical care. Comput Methods Programs Biomed. 2008;89(2):141–152. doi: 10.1016/j.cmpb.2007.04.006. [DOI] [PubMed] [Google Scholar]
- 19.Lin J, Lee D, Chase J, Hann C, Lotz T, Wong X. Stochastic modelling of insulin sensitivity variability in critical care. Biomed Signal Proc Control. 2006;1:229–242. [Google Scholar]
- 20.Hertz DE, Karn CA, Liu YM, Liechty EA, Denne SC. Intravenous glucose suppresses glucose production but not proteolysis in extremely premature newborns. J Clin Invest. 1993;92(4):1752–1758. doi: 10.1172/JCI116763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sunehag A, Ewald U, Larsson A, Gustafsson J. Glucose production rate in extremely immature neonates (< 28 weeks) studied by use of deuterated glucose. Pediatr Res. 1993;33(2):97–100. doi: 10.1203/00006450-199302000-00001. [DOI] [PubMed] [Google Scholar]
- 22.Sunehag A, Gustafsson J, Ewald U. Very immature infants (< or = 30 Wk) respond to glucose infusion with incomplete suppression of glucose production. Pediatr Res. 1994;36(4):550–555. doi: 10.1203/00006450-199410000-00024. [DOI] [PubMed] [Google Scholar]
- 23.Tyrala EE, Chen X, Boden G. Glucose metabolism in the infant weighing less than 1100 grams. J Pediatr. 1994;125(2):283–287. doi: 10.1016/s0022-3476(94)70212-8. [DOI] [PubMed] [Google Scholar]
- 24.Sunehag A, Ewald U, Gustafsson J. Extremely preterm infants ( < 28 weeks) are capable of gluconeogenesis from glycerol on their first day of life. Pediatr Res. 1996;40(4):553–557. doi: 10.1203/00006450-199610000-00007. [DOI] [PubMed] [Google Scholar]
- 25.Farrag HM, Dorcus EJ, Cowett RM. Maturation of the glucose utilization response to insulin occurs before that of glucose production in the preterm neonate. Pediatr Res. 1996;39(4):308. [Google Scholar]
- 26.Keshen T, Miller R, Jahoor F, Jaksic T, Reeds PJ. Glucose production and gluconeogenesis are negatively related to body weight in mechanically ventilated, very low birth weight neonates. Pediatr Res. 1997;41(1):132–138. doi: 10.1203/00006450-199701000-00021. [DOI] [PubMed] [Google Scholar]
- 27.Sunehag A, Ewald U, Larsson A, Gustafsson J. Attenuated hepatic glucose production but unimpaired lipolysis in newborn infants of mothers with diabetes. Pediatr Res. 1997;42(4):492–497. doi: 10.1203/00006450-199710000-00012. [DOI] [PubMed] [Google Scholar]
- 28.Sunehag AL, Haymond MW, Schanler RJ, Reeds PJ, Bier DM. Gluconeogenesis from amino acids in VLBW infants receiving total parenteral nutrition. Pediatr Res. 1998;43(Suppl 4):269. doi: 10.2337/diabetes.48.4.791. [DOI] [PubMed] [Google Scholar]
- 29.Diderholm B, Ewald U, Gustafsson J. Effect of theophylline on glucose production and lipolysis in preterm infants (< or = 32 weeks) Pediatr Res. 1999;45(5 Pt 1):674–679. doi: 10.1203/00006450-199905010-00011. [DOI] [PubMed] [Google Scholar]
- 30.Sunehag AL, Haymond MW, Schanler RJ, Reeds PJ, Bier DM. Gluconeogenesis in very low birth weight infants receiving total parenteral nutrition. Diabetes. 1999;48(4):791–800. doi: 10.2337/diabetes.48.4.791. [DOI] [PubMed] [Google Scholar]
- 31.Poindexter BB, Karn CA, Leitch CA, Liechty EA, Denne SC. Amino acids do not suppress proteolysis in premature neonates. Am J Physiol Endocrinol Metab. 2001;281(3):E472–E478. doi: 10.1152/ajpendo.2001.281.3.E472. [DOI] [PubMed] [Google Scholar]
- 32.Sunehag AL. Parenteral glycerol enhances gluconeogenesis in very premature infants. Pediatr Res. 2003;53(4):635–641. doi: 10.1203/01.PDR.0000054774.90893.0F. [DOI] [PubMed] [Google Scholar]
- 33.Sunehag AL. The role of parenteral lipids in supporting gluconeogenesis in very premature infants. Pediatr Res. 2003;54(4):480–486. doi: 10.1203/01.PDR.0000081298.06751.76. [DOI] [PubMed] [Google Scholar]
- 34.Van Kempen AA, Romijn JA, Ruiter AF, Ackermans MT, Endert E, Hoekstra JH, Kok JH, Sauerwein HP. Adaptation of glucose production and gluconeogenesis to diminishing glucose infusion in preterm infants at varying gestational ages. Pediatr Res. 2003;53(4):628–634. doi: 10.1203/01.PDR.0000054733.13366.AF. [DOI] [PubMed] [Google Scholar]
- 35.Van Kempen AA, Romijn JA, Ruiter AF, Endert E, Weverling GJ, Kok JH, Sauerwein HP. Alanine administration does not stimulate gluconeogenesis in preterm infants. Metabolism. 2003;52(8):945–949. doi: 10.1016/s0026-0495(03)00148-3. [DOI] [PubMed] [Google Scholar]
- 36.Van Kempen AA, Ackermans MT, Endert E, Kok JH, Sauerwein HP. Glucose production in response to glucagon is comparable in preterm AGA and SGA infants. Clin Nutr. 2005;24(5):727–736. doi: 10.1016/j.clnu.2005.02.004. [DOI] [PubMed] [Google Scholar]
- 37.Van den Akker CH, te Braake FW, Wattimena DJ, Voortman G, Schierbeek H, Vermes A, van Goudoever JB. Effects of early amino acid administration on leucine and glucose kinetics in premature infants. Pediatr Res. 2006;59(5):732–735. doi: 10.1203/01.pdr.0000214990.86879.26. [DOI] [PubMed] [Google Scholar]
- 38.Van Kempen AA, van der Crabben SN, Ackermans MT, Endert E, Kok JH, Sauerwein HP. Stimulation of gluconeogenesis by intravenous lipids in preterm infants: response depends on fatty acid profile. Am J Physiol Endocrinol Metab. 2006;290(4):E723–E730. doi: 10.1152/ajpendo.00303.2005. [DOI] [PubMed] [Google Scholar]
- 39.Chacko SK, Sunehag AL. Gluconeogenesis continues in premature infants receiving total parenteral nutrition. Arch Dis Child Fetal Neonatal Ed. 2010;95(6):F413–F418. doi: 10.1136/adc.2009.178020. [DOI] [PubMed] [Google Scholar]
- 40.Chacko SK, Ordonez J, Sauer PJ, Sunehag AL. Gluconeogenesis is not regulated by either glucose or insulin in extremely low birth weight infants receiving total parenteral nutrition. J Pediatr. 2011;158(6):891–896. doi: 10.1016/j.jpeds.2010.12.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Le Compte A, Chase JG, Lynn A, Hann C, Shaw G, Wong XW, Lin J. Blood glucose controller for neonatal intensive care: virtual trials development and first clinical trials. J Diabetes Sci Technol. 2009;3(5):1066–1081. doi: 10.1177/193229680900300510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Le Compte A, Chase JG, Lynn A, Hann C, Shaw G, Wong XW, Lin J. Blood glucose controller for neonatal intensive care: virtual trials development and first clinical trials. J Diabetes Sci Technol. 2009;3(5):1066–1081. doi: 10.1177/193229680900300510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hann CE, Chase JG, Shaw GM. Integral-based identification of patient specific parameters for a minimal cardiac model. Comput Methods Programs Biomed. 2006;81(2):181–192. doi: 10.1016/j.cmpb.2005.11.004. [DOI] [PubMed] [Google Scholar]
- 44.Dickson JL, Le Compte AJ, Floyd RP, Chase JG, Lynn A, Shaw GM. Development and optimisation of stochastic targeted (STAR) glycaemic control for pre-term infants in neonatal intensive care. Biomed Signal Proc Control. 2013;8(2):215–216. [Google Scholar]
- 45.Sunehag AL, Haymond MW, Schanler RJ, Reeds PJ, Bier DM. Gluconeogenesis in very low birth weight infants receiving total parenteral nutrition. Diabetes. 1999;48(4):791–800. doi: 10.2337/diabetes.48.4.791. [DOI] [PubMed] [Google Scholar]
- 46.Sunehag A, Ewald U, Larsson A, Gustafsson J. Glucose production rate in extremely immature neonates (< 28 weeks) studied by use of deuterated glucose. Pediatr Res. 1993;33(2):97–100. doi: 10.1203/00006450-199302000-00001. [DOI] [PubMed] [Google Scholar]
- 47.Van Goudoever JB, Sulkers EJ, Chapman TE, Carnielli VP, Efstatopoulos T, Degenhart HJ, Sauer PJ. Glucose kinetics and glucoregulatory hormone levels in ventilated preterm infants on the first day of life. Pediatr Res. 1993;33(6):583–589. doi: 10.1203/00006450-199306000-00010. [DOI] [PubMed] [Google Scholar]
- 48.Cowett RM, Oh W, Schwartz R. Persistent glucose production during glucose infusion in the neonate. J Clin Invest. 1983;71(3):467–475. doi: 10.1172/JCI110791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000;355(9206):773–778. doi: 10.1016/S0140-6736(99)08415-9. [DOI] [PubMed] [Google Scholar]
- 50.McCowen KC, Malhotra A, Bistrian BR. Stress-induced hyperglycemia. Crit Care Clin. 2001;17(1):107–124. doi: 10.1016/s0749-0704(05)70154-8. [DOI] [PubMed] [Google Scholar]
- 51.Sunehag A, Gustafsson J, Ewald U. Glycerol carbon contributes to hepatic glucose production during the first eight hours in healthy term infants. Acta Paediatr. 1996;85(11):1339–1343. doi: 10.1111/j.1651-2227.1996.tb13921.x. [DOI] [PubMed] [Google Scholar]
- 52.Tigas SK, Sunehag AL, Haymond MW. Impact of duration of infusion and choice of isotope label on isotope recycling in glucose homeostasis. Diabetes. 2002;51(11):3170–3175. doi: 10.2337/diabetes.51.11.3170. [DOI] [PubMed] [Google Scholar]
- 53.LeCompte AJ, Lynn A, Chase JG, Shaw GM, Pretty CG, Mayntzhusen K, Docherty PD, Parente J. Tight glycemic control in the neonatal intensive care unit - proof of concept pilot trials. In: American Diabetes Association (ADA) 69th Scientific Sessions, Jun 5-9, 2009, New Orleans, LA. Diabetes. 2009;58(Suppl 1):A162. [Google Scholar]