

Abstract
Several methods are used for estimating the anaerobic threshold (AT) during exercise. The aim of the present study was to compare AT values based on blood lactate measurements with those obtained from computerised calculations of different respiratory gas indices. Twelve healthy, well-trained men performed a stepwise incremental test on both treadmill and cycle ergometer. Respiratory gases were measured continuously, and blood samples were drawn every third minute. AT was determined, based on 1) blood lactate concentrations (Lactate-AT), 2) respiratory exchange ratio (RER-AT), 3) V- slope method (Vslope-AT), and 4) ventilatory equivalent for VO2 (EqO2-AT). Lactate-AT and RER-AT values showed similar values, both on treadmill and on cycle ergometer. EqO2-AT showed a trend towards lower values for AT, while Vslope-AT gave significantly lower values for AT for both exercise modes. Bland-Altman plots showed an even distribution of data for RER-AT, while a more scattered and skewed distribution of data was observed when EqO2-AT and Vslope-AT were compared with Lactate-AT. The study demonstrates that RER-based estimates of AT correlate well with the blood lactate-based AT determination. The RER method is non-invasive and simple to perform, and, in the present study, seemed to be the best respiratory index for estimation of AT.
Key Points.
Anaerobic threshold can reliably be estimated by respiratory gas indices in well fit subjects.
Sophisticated computerassisted equations are not superior to the use of a simple cut-off value of Respiratory Exchange Ratio in estimating the anaerobic threshold.
Estimation of anaerobic threshold, by using a pre-defined cut-off value for Respiratory Exchange Ratio, is non- invasive and simple to perform in a respiratory laboratory.
Key words: Anaerobic threshold, exercise test
Introduction
Exercise physiologists have for many years had knowledge about a critical work intensity above which lactate accumulation occurs (Owles, 1930; Wasserman and McIlroy, 1964). Although somewhat controversial, AT has been widely used as an objective measure for aerobic work capacity in both athletes and patients (Wasserman and McIlroy, 1964; Katz et al., 1992; Roecker et al., 1998; Coen et al., 2001). AT has also been used to help in discriminating between cardiovascular and pulmonary limitation to exercise (Wasserman 1984). Several methods, both invasive and non-invasive, have been used for estimating the AT, and there is no international consensus about what is the best procedure.
Invasive methods require repeated measurements of blood lactate concentration and give a lactate defined anaerobic threshold (Lactate-AT). Both the point of abrupt increase in lactate level and the non-linear rise in blood lactate concentration have been used (Beaver et al., 1985; Katz et al. 1992), inferring visual inspection of plotted curves of data. Others define a specific blood lactate cut-off value, such as 2.0, 3.0 or 4.0 mmol·l-1 (Yeh et al., 1983; Hech et al., 1985; Borch et al., 1993). Some laboratories calculate an individual anaerobic threshold based on for example the resting value of blood lactate plus 1.5 mmol·l-1 (Roecker et al., 1998, Helgerud et al., 2001). Whether lactate is measured in arterial, capillary or venous blood will also influence the results (Yeh et al., 1983).
Non-invasive methods are based on continuous measurement of respiratory gases and give a respiratory gases defined anaerobic threshold (RAT). In an old method for estimating RAT, the relationship between expired CO2 and inspired O2 (respiratory exchange ratio, RER) is used, and AT is detected either at the point where RER starts to rise, or where RER exceeds a certain defined cut-off value, such as 1.0 (RER-AT) (Yeh et al., 1983; Anderson and Rhodes, 1989; Dickstein et al., 1990; Myers and Ashley, 1997). This method has later been considered inaccurate (Caiozzo et al., 1982), and several other methods have been proposed (Anderson and Rhodes, 1989; Myers and Ashley, 1997), for example the V-slope method (Beaver at al., 1986), and the ventilation equivalent for O2 (EqO2) (Reinhard et al., 1979).
In the present study we wanted to compare three different computer-based methods for estimating AT from respiratory gases analysis, with the more invasive method of Lactate-AT. We also wanted to investigate whether the relationship between these methods were dependent on the mode of exercise. Therefore the study subjects were exercised both on treadmill and cycle ergometer.
Methods
Subjects
Twelve healthy men were recruited (Table 1). All subjects were endurance trained and were familiar with treadmill running and ergometer cycling. The study was approved by the Regional Ethics Committee and in accordance with the Helsinki Declaration.
Table 1.
Anthropometrical- and haematological data.
| Mean (±SD) | |
|---|---|
| Age (years) | 26.5 (4.81) |
| Height (cm) | 1.83 (.06) |
| Weight (kg) | 74.7 (6.28) |
| Hb (g·dl-1) | 14.2 (.98) |
| Hematocrit (fraction) | .41 (.07) |
| Endurance training per week(hours) | 4.2 (.23) |
Testing procedure
The subjects were randomised to perform either the treadmill test (n = 6) or the cycle ergometer test (n = 6) first. All participants had two days of rest between the two tests. Restrictions against intensive training two days ahead of testing, and in the two days between testing, were given. The subjects fasted for 4 hours prior to each exercise. All subjects were examined by a physician. Dynamic spirometry and electrocardiogram (ECG) were performed, confirming normal lung function and ECG.
The respiratory gas measurements were done using a Jaeger Oxycon Champion spirometric analysator (Erich Jaeger GmBH & Co Wuerzburg, Germany). Calibrations of flow transducer and gas analysers were performed daily. A Triple V transducer with mouthpiece detecting breath-by-breath- registrations of oxygen uptake (VO2), expired CO2 (VCO2), minute ventilation (VE) was used. The dead space in this unit was 42 ml. Breath-by-breath-registrations were registered, and mean values of registrations from every minute were used in further statistical analyses. Double capillary samples were drawn from a finger using an Outlet 2000 pistol and Unilet 2000 lancets. The samples were taken two minutes after each increase in workload and immediately analysed for lactate concentration (YSI 1500 sport, USA). The analysator was calibrated between each subject with five- and 15 mmol·l-1 standard solutions. The double lactate samples showed a mean difference of 0.02 mmol·l-1 with a standard deviation of 0.25 mmol·l-1. The participants stated their subjective feeling of exhaustion by using Borg’s CR10 exhaustion scale (Borg, 1982). Heart rate was monitored at the end of each exercise level using a Polar Sport Tester (HRM, Finland).
Before starting the exercise test, resting values of VO2 were to be stabilized below 3.5 ml-1·min-1·kg-1 for three minutes (1 MET). The subjects were instructed to warm up for ten minutes without mouthpiece, and a capillary blood sample for lactate analysis was taken. An incremental test with increasing workload every three minutes was employed.
The treadmill test
The subjects exercised on a Jaeger LE 300 C treadmill (Erich Jaeger GmBH & Co Wuerzburg, Germany). A five percent slope was used during the whole test. Starting speed was eight km·h-1, and the speed was increased by two km·h-1 every three minutes to subjective exhaustion. One subject lost the mouthpiece, and his treadmill test was excluded from further analyses.
The cycle ergometer test
The subjects exercised on a Jaeger ER 900 cycle ergometer (Erich Jaeger GmBH & Co Wuerzburg, Germany). The cycling position was standardised with a 160° knee angle with pedal in lowest position. During exercise the cadence should be held at constant 70 r·min-1. The first workload was 150 W, increasing by 50 W every three minutes to subjective exhaustion.
The AT-calculations
Lactate-AT: The lactate threshold was defined as the mean value of lactate concentrations in capillary blood during warm-up and the first workload + 1.5 mmol·l-1 (Helgerud et al., 1990; 2001). From the lactate concentrations, which were determined every three minutes, a third order curve linear regression was calculated. From this regression curve, Lactate-AT was expressed as the VO2 at the time when the lactate threshold was superseded (example in Figure 1a).
Figure 1.
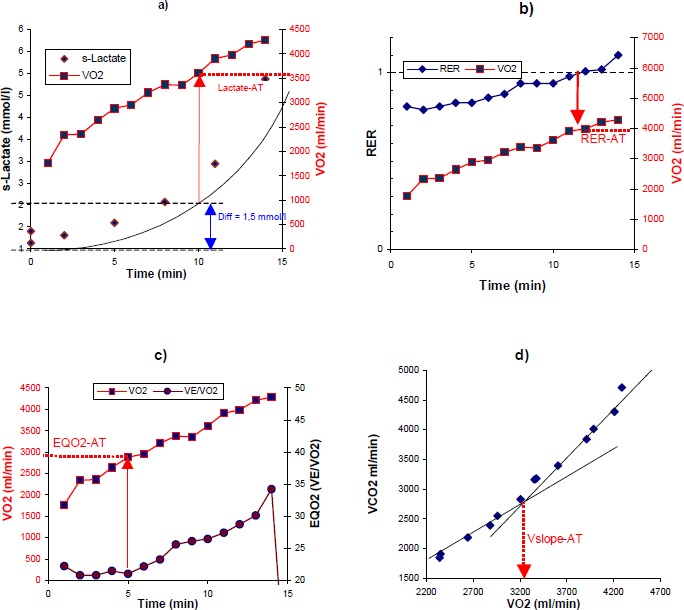
Examples showing methods of estimating the anaerobic threshold, see material and methods for detail. a) Lactate-AT is the point where the trend line for s-lactate exceeds pretest level + 1.5 mmol·l-1. b) RER-AT is the point where RER exceeds 1.0. c) EQ-AT is where EQO2 (VE/VO2) is at the minimum before it starts rising under exercise. d) Vslope-AT is the crossing point between the regression lines for VO2 plotted against VCO2 during first part of the exercise and during the last part of the exercise.
RER-AT: The software calculated the RER automatically. RER-AT was defined as the VO2 at the time when RER stabilized above 1.0 not returning to levels below (Yeh et al., 1983; Dickstein et al., 1990). Mean values for every minute were used in the calculations (example in Figure 1b).
EqO2-AT: The point of AT was detected using the EqO2 method (Reinhard et al., 1979). The ventilation equivalent of oxygen (VE/VO2) was computed, and the point where VE/VO2 starts rising was automatically detected by the computer software (example in Figure 1c).
Vslope-AT: The point of AT was detected using v-slope technique as described earlier (Beaver at al., 1986). The VCO2 versus VO2 curve is divided into two regions, each of which is fitted by linear regression, and the intersection between the two regression lines is regarded as the Vslope-AT. The software of the Jaeger equipment automatically established the regression lines and their crossing points (example in Figure 1d).
Statistics
Data are presented as mean (±standard deviation, SD) for description purpose, and as mean (±standard error of the mean, SE) for comparison purpose. Data were analysed by SPSS version 10.0. Histograms and Q-Q plots were used to check for normal distribution of data. To visualise the relationship between data, a Bland-Altman plot was used (Bland an Altman, 1986). A paired Student’s t-test to test for significant differences between the two test models was employed for ordinal data. Pearson’s two-tailed correlation test with 95 % confidence interval was used to test the correlation between Lactate-AT and the other methods of AT determination. Ninety-five percent confidence intervals (CI) for difference between methods were computed. P-values below 0.05 were considered statistical significant.
Results
The test was not designed as a VO2max test, but all the test persons had high peak VO2 with 61.8 ± 4.6 ml-1·min-1·kg-1 on the treadmill and 58.6 ± 4.8 ml-1·min-1·kg-1 on the cycle ergometer. The maximum attained lactate concentrations of 8.70 ± 1.47 mmol·l-1 on the treadmill and 8.71 ± 1.77 mmol·l-1 on the cycle ergometer indicated that all of the subjects exceeded their AT as defined in this study. This was also confirmed by the RER measurements which all exceeded 1.0 (1.22 ± 0.09 on the treadmill and 1.21 ± 0.06 on the cycle ergometer). Mean exhaustion time was 14.5 minutes and perceived dyspnoe at maximal workload was rated 6 on Borg’s scale (Borg, 1982) on cycle ergometer, versus 13.5 minutes and 7 on treadmill test.
In Table 2 the AT estimations by the four different methods are presented. There were no significant differences between VO2 values at attained Lactate-AT and RER-AT, neither for treadmill test nor for ergometer cycle test. The difference between RER-AT and Lactate-AT was 53 ml·min-1 (CI -258 to 152) for ergometer cycle test and 51 ml·min-1 (CI -79 to 182) for treadmill test.
Table 2.
Comparison of anaerobic thresholds as determined by blood lactate (Lactate-AT), respiratory exchange ratio (RER-AT), V-slopemethod (Vslope-AT), and ventilatory equivalent for O2 (EqO2-AT). Values in VO2 ml·min-1. Data are means (±SE).
| Lactate-AT | RER-AT | Vslope-AT | EqO2-AT | |
|---|---|---|---|---|
| Treadmill test | 3961 (119) | 4013 (138) | 3315 (190) * | 3632 (195) |
| Cycle ergometer test | 3409 (101) | 3356 (120) | 2729 (149) * | 3211 (251) |
* The differences are statistically significant for Vslope-AT vs Lactate-AT (p = 0.01 for treadmill test and p = 0.001 for ergometer test).
EqO2-AT and Vslope-AT gave lower values for AT, especially for Vslope-AT, where a significant difference from Lactate-AT was found. The difference between EqO2-AT and Lactate-AT was -198 ml·min-1 (CI -741 to 345) for ergometer cycle test and -329 ml·min-1 (CI -688 to 30) for treadmill test. The difference between Vslope-AT and Lactate-AT was -680 for ergometer cycle test (CI -1033 to -327) and -646 (CI -1111 to -181) for treadmill test.
Including data from both exercise modes we found a significant correlation between Lactate-AT and RER-AT (r = 0.87, p < 0.001). Similarly a positive correlation for Lactate-AT and EqO2-AT was found (r = 0.45, p < 0.05) and between Lactate-AT and Vslope-AT (r = 0.42, p < 0.05).
The Bland-Altman plot illustrates an even distribution of Lactate-AT and RER-AT without deviation depending on the mean value of AT (Figure 2). Vslope-AT and EqO2-AT, however, tends to show lower values than Lactate-AT, especially in the lower range of their mean values.
Figure 2.
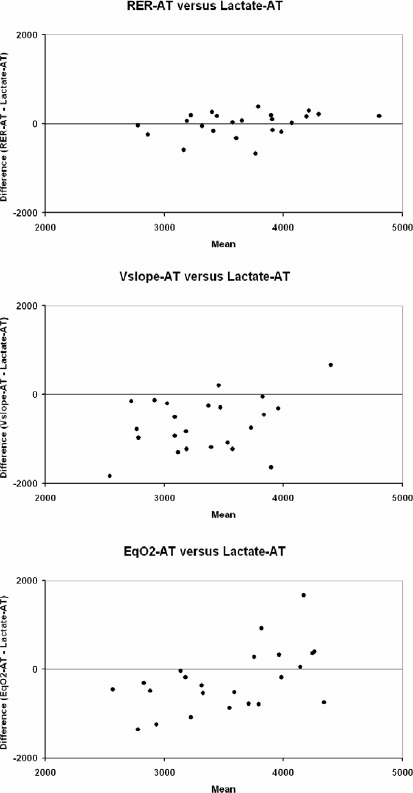
Altman-Bland plots showing difference between anaerobic threshold detected by the RER-AT, Vslope-AT and EqO2-AT method versus blood lactate detected AT (Lactate-AT). Both exercise modes are included in the plots. Values in VOO2 ml·min-1
Discussion
In this study we have compared well-known methods for estimating AT, one invasive method with direct measurement of lactate in blood, and three computer based, non-invasive methods. We have used standard test procedures and recruited a homogeneous group of subjects. The results indicated minimal difference between the obtained Lactate-AT and RER-AT data, both on treadmill and on cycle ergometer. The RER-AT method, which is simple to perform, thus seems to give a valuable estimate of the anaerobic threshold.
The V-slope method and the EqO2 method did not correspond with the lactate-AT as well as the RER defined method. Both the EqO2-AT and Vslope-AT methods had a tendency to show lower values than the lactate-AT, especially in the lower range of AT. This is in accordance to the findings of Cheng et al (Cheng et al., 1992) where the ratio between Lactate-AT, Vslope-AT and EqO2-AT was similar to ours. One would perhaps expect closer estimations of RER-AT and Vslope-AT since they both originate from VCO2 versus VO2 values. Our values for Vslope-AT are generally lower than for RER-AT, and this might be due to the chosen cut-off value for RER.
Maximal oxygen uptake is usually higher on treadmill than on bicycle (Zeballos and Weisman, 1994), and anaerobic threshold is reported to occur at slightly higher values of VO2 during treadmill running (Medelli et al., 1993). Studies have also indicated adaptation to mode of exercise regarding both work economy and energy turnover (Hirakoba et al., 1992; Roecker et al., 2000). Ten out of twelve of our test subjects reported aerobic training with preference for running, and all the test subjects achieved higher VO2-values at AT on the treadmill than on the cycle ergometer. However, the ratio between AT estimated by the different methods were not essentially affected by mode of exercise.
Several methods for detecting the Lactate-AT are used. In order to avoid inter personal errors in determination, we have chosen to use a definite cut off value rather than trying to define the point at which blood lactate concentration starts to rise. This can probably result in somewhat higher estimates of Lactate-AT than in other studies. Using the initial rise in lactate might have decreased the difference between EqO2-AT and Lactate-AT and between Vslope-AT and Lactate-AT. In the Bland Altman plots, this would result in a shift along the y-axis towards higher values for all the respiratory parameters. However, still there is a problem with more scattered data for Vslope- AT, and the skewed distribution of data for and EqO2-AT in the Bland-Altman plots.
In the current study we chose a modified Bruce protocol (Zeballos and Weisman, 1994) using a three minutes stepwise incremental exercise test (Roecker et al., 1998; Coen et al., 2001). Others have used intervals of one minute to make the test shorter and easier to execute (Wasserman et al., 1973; Zeballos et al. 1998).
It should be stressed that the current study is performed on well-trained healthy subjects, and that the results cannot automatically be applied to patients. However there are data from previous studies indicating that Lactate-AT and RAT correspond reasonable well also in patients with heart diseases (Dickstein et al., 1990; Katz et al., 1992).
Several studies have investigated the relation between respiratory gases exchange indices and blood lactate levels in order to determine which respiratory gases index predict the Lactate-AT best (Wasserman et al., 1973; Davis et al., 1976; Caiozzo et al., 1982; Katz et al., 1992; Patessio et al., 1993). In the majority of these studies the anaerobic threshold has been detected by visual inspection of plotted data in search for an abrupt or non-linear rise in parameter values, either regarding Lactate-AT, RAT, or both. This may result in bias in the interpretation of data, and inter-observer errors have been a concern (Yeh et al., 1983; Garrard and Das, 1987). Computerized treatment of data may overcome this problem by computing regression lines of measured data, indices or log-converted data (Dickstein et al., 1990; Katz et al., 1992 von Duvillard et al., 1993; Miyahara et al., 2000 ). However, this does not necessarily improve the validity and reproducibility of the results. In this study we have shown that a simple parameter as RER, with a predefined cut-off value, can give a reasonable good estimate of the AT.
There are few recent studies treating RER as a single parameter predicting the AT. Yeh et al. (1983) found that RER = 1.0 gives a valuable estimate of Lactate-AT in healthy subjects. Dickstein et al. (1990) found that RER = 1 corresponded well with Lactate-AT in patients with heart disease, although the RER-AT occurred at somewhat higher levels of VO2 than Lactate-AT. With regard to the present study, this discrepancy might be due to different definitions of the Lactate-AT. RER data have shown a low inter-observer variability (Cohen-Solal et al., 1994), and are easy to interpret. When calculating AT from respiratory gases, a standardised timetable for sampling is not necessary as it is for lactate measurements, since the measurement of respiratory gases is performed continuously. Hence, the risk of reaching AT in the interval between two sampling procedures, which can be a problem using blood samples in the calculations, is eliminated. Moreover invasive methods may require fixation of the arm with adjustment of the running technique during blood sampling. This was reported as a problem during the treadmill test since it resulted in a subjective feeling of muscle soreness.
Conclusions
Computerised determination of AT by the RER method gives comparable results with AT determined by blood lactate concentrations. Estimation of AT, by using a pre-defined cut-off value for RER, is non-invasive and simple to perform in a respiratory laboratory.
Biographies
Geir SOLBERG
Employment
SHO, Department of Pulmonary Medicine, Ullevål Univ. Hospital, and Faculty of Medicine, University of Oslo, Norway.
Degrees
MD
Research interests
Respiratory physiology and sports medicine.
Bjørn ROBSTAD
Employment
SHO, Department of Pulmonary Medicine, Ullevål Univ. Hospital, and Faculty of Medicine, University of Oslo, Norway.
Degrees
PhD
Research interests
Respiratory physiology and sports medicine.
Ole H. SKJØNSBERG
Employment
Professor of pulmonary medicine at the University of Oslo, and consultant, Department of Pulmonary Medicine, Ullevål Univ. Hospital, Oslo, Norway.
Degrees
MD, PhD
Research interests
Respiratory physiology and respiratory insufficiency.
E-mail: o.h.skjonsberg@medisin.uio.no
Fredrik BORCHSENIUS
Employment
The head of the Department of Pulmonary Medicine, Ullevål Univ. Hospital, Oslo, Norway
Degrees
MD
Research interests
Respiratory physiology.
E-mail: fborchse@online.no
References
- Anderson G.S., Rhodes E.C. (1989) A review of blood lactate and ventilatory methods of detecting tansition tresholds. Sports Medicine 8, 3-55 [DOI] [PubMed] [Google Scholar]
- Beaver W.L, Wasserman K., Whipp B.J. (1985) Improved detection of lactate tresholdduring exercise using a log-log transformation. Journal of Applied Physiology 59, 1936-1940 [DOI] [PubMed] [Google Scholar]
- Beaver W.L., Wasserman K., Whipp B.J. (1986) A new method for detecting anaerobic threshold by gas exchange. Journal of Applied Physiology 60, 2020-2027 [DOI] [PubMed] [Google Scholar]
- Bland J.M., Altman D.G. (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1(8476), 307-310 [PubMed] [Google Scholar]
- Borch K.W., Ingjer F., Larsen S., Tomten S.E. (1993) Rate of accumulation of blood lactate during graded exercise as a predictor of “anaerobic threshold”. Journal of Sports Sciences 11, 49-55 [DOI] [PubMed] [Google Scholar]
- Borg G.A. (1982) Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise 14, 377-381 [PubMed] [Google Scholar]
- Breuer H. (1997) Spiroergometrie. Indikationen, methodik, relevanz. Deutsche Medizinische Wochenschrift 122, 447-449(In German: English abstract) [DOI] [PubMed] [Google Scholar]
- Caiozzo V.J., Davis J.A., Ellis J.F., Azus J.L., Vandagriff R., Prietto C.A., McMaster W.C. (1982) A comparison of gas exchange indices used to detect the anaerobic threshold. Journal of Applied Physiology 53, 1184-1189 [DOI] [PubMed] [Google Scholar]
- Cheng B., Kuipers H., Snyder A.C., Keizer H.A., Jeukendrup A., Hesselink M. (1992) A new approach for the determination of ventilatory and lactate thresholds. International Journal of Sports Medicine 13, 518-522 [DOI] [PubMed] [Google Scholar]
- Coen B., Urhausen A., Kindermann W. (2001) Individual anaerobic threshold: Methological aspects of its assessment in running. International Journal of Sports Medicine 22, 8-16 [DOI] [PubMed] [Google Scholar]
- Cohen-Solal A., Aupetit J.F., Gueret P., Kolsky H., Zannad F. (1994) Can anaerobic threshold be used as an end-point for therapeutic trials in heart failure?. Lessons from a multicentre randomised placebo-controlled trial. European Heart Journal 15, 236-241 [DOI] [PubMed] [Google Scholar]
- Cooper C.B., Beaver W.L., Cooper D.M., Wasserman K. (1992) Factors affecting the components of the alveolar CO2 output - O2 uptake during incremental exercise in man. Experimental Physiology 77, 51-64 [DOI] [PubMed] [Google Scholar]
- Davis J.A., Vodak P., Wilmore J.H., Vodak J., Kurtz P. (1976) Anaerobic threshold and maximal aerobic power for three modes of exercise. Journal of Applied Physiology 41, 544-550 [DOI] [PubMed] [Google Scholar]
- Dennis S.C., Noakes T.D., Bosch A.N. (1992) Ventilation and blood lactate increase exponentially during incremental exercise. Journal of Sports Sciences 10, 437-449 [DOI] [PubMed] [Google Scholar]
- Dickstein K., Barvik S., Aarsland T., Snapinn S., Millerhagen J. (1990) Validation of a computerized technique for detection of the gas exchange anaerobic threshold in cardiac disease. The American Journal of Cardiology 66, 1363-1367 [DOI] [PubMed] [Google Scholar]
- Dickstein K., Barvik S., Aarsland T., Snapinn S., Karlsson J. (1990) A comparison of methodologies in detection of the anaerobic threshold. Circulation81 (Suppl. 2), 38-46 [PubMed] [Google Scholar]
- Garrard C.S., Das R. (1987) Sources of error and variability in the determination of anaerobic threshold in healthy humans. Respiration 51, 137-145 [DOI] [PubMed] [Google Scholar]
- Hech H., Mader A., Hess G., Mucke S., Muller R., Hollmann W. (1985) Justification of the 4 mmol/l lactate threshold. International Journal of Sports Medicine 6, 117-130 [DOI] [PubMed] [Google Scholar]
- Helgerud J., Ingjer F., Strømme S.B. (1990) Sex difference in performance-matched marathon runners. European Journal of Applied Physiology and Occupational Physiology 61, 433-439 [DOI] [PubMed] [Google Scholar]
- Helgerud J., Engen L.C., Wisløff U., Hoff J. (2001) Aeroboc endurance training improves soccer performance. Medicine and Science in Sports and Exercise 33, 1925-1931 [DOI] [PubMed] [Google Scholar]
- Hirakoba K., Mauyana A., Inaki M., Misaka K. (1992) Effect of endurance training on excessive CO2 expiration due to lactate production in exercise. European Journal of Applied Physiology and Occupational Physiology 64, 73-77 [DOI] [PubMed] [Google Scholar]
- Katz S.D., Berkowitz R., LeJemtel T.H. (1992) Anaerobic threshold detection in patients with congestive heart failure. The American Journal of Cardiology 69, 1565-1569 [DOI] [PubMed] [Google Scholar]
- Medelli J., Maingourd Y., Bouferrache B., Bach V., Freville M., Libert J-P. (1993) Maximal oxygen uptake and aerobic-anaerobic transition on treadmill and bicycle in triathletes. Japanese Journal of Physiology 43, 347-360 [DOI] [PubMed] [Google Scholar]
- Miyahara N., Eda R., Takeyama H., Maeda T., Aoe K., Kunichika N., Kohara H., Harada M. (2000) Cardiorespiratory responses during cycle ergometer exercise with different ramp slope increments in patients with chronic obstructive pulmonary disease. Internal Medicine 39, 15-19 [DOI] [PubMed] [Google Scholar]
- Myers J., Ashley E. (1997) Dangerous curves. A perspective on exercise, lactate, and the anaerobic threshold. Chest 111, 787-795 [DOI] [PubMed] [Google Scholar]
- Owles W.H. (1930) Alterations in the lactic acid content of the blood as a result of light exercise, and associated changes in the CO2-combining power of the blood and in the alveolar CO2 pressure. The Journal of Physiology 69, 214-237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patessio A., Casaburi R., Carone M., Appendini L., Donner C.F., Wasserman K. (1993) Comparison of Gas Exchange, Lactate Acidosis Thresholds in Patients with Chronic Obstructive Pulmonary Disease. The American Review of Respiratory Disease 148, 622-626 [DOI] [PubMed] [Google Scholar]
- Reinhard U., Müller P.H., Schmülling R-M. (1979) Determination of anaerobic threshold by the ventilation equivalent in normal individuals. Respiration 38, 36-42 [DOI] [PubMed] [Google Scholar]
- Roecker K., Schotte O., Niess A.M., Horsmann T., Dickhuth H-M. (1998) Predicting competition performance in long-distance running by means of a treadmill test. Medicine and Science in Sports and Exercise 30, 1552-1557 [DOI] [PubMed] [Google Scholar]
- Roecker K., Mayer F., Striegel H., Dickhuth H-H. (2000) Increase Characteristics of the cumulated excess CO2 and the lactate concentration during exercise. International Journal of Sports Medicine 21, 419-423 [DOI] [PubMed] [Google Scholar]
- Sjödin B., Svedenhag J. (1985) Applied physiology of marathon running. Sports Medicine 2, 83-99 [DOI] [PubMed] [Google Scholar]
- Von Duvillard S.P., le Mura L.L., Bacharach D.W., di Vico P. (1993) Determination of lactate threshold by respiratory gas exchange measures and blood lactate levels during incremental load work. Journal of Manipulative and Physiological Therapeutics 16, 312-318 [PubMed] [Google Scholar]
- Walsh M.L., Banister E.W. (1988) Possible mechanisms of the anaerobic threshold. A review. Sports Medicine 5, 269-302 [DOI] [PubMed] [Google Scholar]
- Wasserman K., McIlroy M.B. (1964) Detecting the threshold of anaerobic metabolism in cardiac patients during exercise. The American Journal of Physiology 14, 844-852 [DOI] [PubMed] [Google Scholar]
- Wasserman K., Whipp B.J., Koyal S.N., Beaver W.L. (1973) Anaerobic Threshold and Respiratory Gas exchange during Exercise. Journal of Applied Physiology 35, 236-243 [DOI] [PubMed] [Google Scholar]
- Wasserman K. (1984) The anaerobic threshold measurement to evaluate exercise performance. The American Review of Respiratory Disease 129(Suppl.), S35-S40 [DOI] [PubMed] [Google Scholar]
- Yeh M.P., Gardner R.M., Adams T.D., Yanowitz F.G., Crapo R.O. (1983) “Anaerobic threshold”: problems of determination and validation. Journal of Applied Physiology 55, 1178-1186 [DOI] [PubMed] [Google Scholar]
- Zeballos R.J., Weisman I.M. (1994) Behind the scenes of cardiopulmonary exercise testing. Clinics in Chest Medicine 15, 193-213 [PubMed] [Google Scholar]
- Zeballos R., Jorge M.D., Weisman I.M., Connery S.M. (1998) Comparison of pulmonary gas exchange measurements between incremental and constant exercise above anaerobic threshold. Chest 113, 602-611 [DOI] [PubMed] [Google Scholar]