

Abstract
We studied the effects of self-administered neuromuscular electrical stimulation (NMES) on changes in strength, endurance, selected anthropometric measures, and subject’s perceived shape and satisfaction of the abdominal wall. Twenty-four adults (experimental group) stimulated their abdominals 5 days per week (20-40 minutes per session) for 8 weeks and refrained from engaging in any additional exercise during the study. A control group (N=16) refrained from exercising the abdominals or engaging in any other exercise training during the study. Subjects were tested at the beginning, mid-point, and end of the study. Isometric strength of the abdominal muscles was tested using a isokinetic dynamometer, endurance was measured using the ACSM curl-up test, abdominal circumference was measured using a steel tape measure, and body shape and satisfaction were assessed via questionnaire. The stimulation group had a 58% increase in abdominal strength, whereas the control group did not change. The stimulation group also had a 100% increase in abdominal endurance versus a 28% increase in the control group. Waist circumference decreased by of 3.5 cm in the stimulation group compared to no significant change in the control group. All 24 subjects in the stimulation group felt that their midsections were more “toned” and “firmed” and 13/24 (54%) felt that their posture had improved as a result of the stimulation. None of the control group subjects reported changes in these parameters. There were no significant differences in body weight, BMI, or skinfold thickness over the course of the study in either group. NMES, as used in the current study, resulted in significant improvements in the muscular strength and endurance of the abdominal region, as well as subject’s perceived shape and satisfaction of the mid-section.
Key Points.
Electrical muscle stimulation (EMS) was effective in increasing muscle strength and endurance
All subjects perceived their abdominal muscles to be firmer and more toned as a result of EMS
Abdominal and waist girth was also significantly reduced, despite no changes in body weight or subcutaneous fat
Key Words: Fitness, training, isometric
Introduction
Neuromuscular electrical stimulation (NMES) has been used been used for many years by physical therapists to retard atrophy in denervated muscle and to maintain or improve muscular strength in immobilized muscle following surgery. In the 1960’s, Kots used NMES with elite athletes in the former Soviet Union (Kots, 1977) and found strength improvements of 30-40%, using what came to be known as “Russian stimulation“. He even suggested that NMES might be more effective than exercise alone for strength development.
In recent years, fitness equipment companies have tried to market the benefits of NMES as another in the long line of “get-fit-quick” schemes. The potential to attain “rock-hard abs” or “buns of steel” without having to actually exercise is an attractive lure for many people who do not have the time or motivation to engage in traditional exercise programs. One area that has drawn considerable attention is the mid-section. Alon and colleagues conducted a series of studies that investigated the effects of NMES on the strength and endurance of the abdominal region (Alon et al., 1987; 1992; Alon and Taylor, 1997). They found that NMES to the abdominal musculature was well tolerated and resulted in strength improvements ranging from 14-22%. Alon et al. (1992) also found that 5 days of stimulation was better than 3 days at inducing changes (Alon et al., 1992). Similarly, when NMES was applied to induce contraction of the knee extensors or plantar flexors, strength gains in the range of 17-31% have been found (Balogun et al., 1993; Currier and Mann, 1983; Maffiuletti et al., 2002; Romero et al., 1982; Selkowitz, 1985). A common finding among these studies was that the stimulation was reasonably comfortable, allowing subjects to obtain muscular contractions in excess of 60% of their maximal voluntary contraction (MVC).
Trying to capitalize on the vanity of consumers, a number of companies have incorporated NMES technology into abdominal stimulation belts and pad systems. A well-controlled study from our laboratory (Porcari et al., 2002) found no improvement in muscle strength, body composition, or physical appearance using one of these commercially available stimulators. The lack of positive results was attributed to the poor quality of the stimulators themselves and the uncomfortable nature of the stimulation, which prevented subjects from attaining sufficiently intense contractions to improve strength. The results of this study prompted the Federal Trade Commission (FTC) to remove several NMES belt products from the market (Green, 2002).
A relatively new abdominal stimulation belt on the market, the Slendertone FLEXTM (Compex Technologies, Minneapolis, MN), has been cleared for use by the Federal Drug Administration (FDA) to strengthen, tone, and firm the abdominal muscles. Two studies conducted by the manufacturer found that use of this system improved isometric strength, isometric and dynamic endurance, and a number of self-perceived outcome measures (Caulfield et al., 2002; Cullinane et al., 2002). However, given the inherent bias characteristic of in-house studies, independent evidence of the accuracy of manufacturer claims is desirable. Accordingly, the purpose of this study was to independently investigate the effects of 8 weeks of NMES on similar parameters.
Methods
Subjects
Forty-one volunteer subjects were recruited from the La Crosse area community to participate in the study. Inclusion criteria required the subjects to be between the ages of 25-50 years old, to have a Body Mass Index (BMI) between 18-30, and not have been involved in any type of formal abdominal training program within the previous 6 months. In addition, subjects with a cardiac pacemaker, any abdominal implants, or who were currently pregnant or had been pregnant within the past 3 months were not eligible to participate in the study. The 41 individuals were randomly assigned into two groups: a control group and a stimulation group. Both groups were instructed not to alter their diet or engage in any additional exercise over the course of the 8-week study period. All subjects provided informed consent. The protocol was previously approved by the Institutional Review Board for the Protection of Human Subjects. Subjects in the stimulation group were paid $100 to participate in the study in order to assure compliance with the study protocol. In addition they got to keep the stimulation belt they had used for training. Subjects in the control group received a free stimulation belt at the conclusion of the study.
Testing
Both groups underwent an identical battery of tests at the beginning, midpoint (4 weeks), and end (8 weeks) of the study. The testing consisted of a series of questionnaires, skinfold measurements, circumference measurements, abdominal strength assessment, and measurement of abdominal endurance. Height and weight were also measured using a standard laboratory scale.
Questionnaires
Subjects were asked to fill out three questionnaires: the Shape Evaluation Scale (Caulfield et al., 2002; Cullinane et al., 2002), the Body Satisfaction Scale (Caulfield et al., 2002; Cullinane et al., 2002), and Rosenberg’s Self-Esteem Scale (Rosenberg, 1989). The Shape Evaluation Scale assesses perceived abdominal shape using a set of ten dichotomous items taken to describe various aspects concerning the shape and appearance of the abdominal region. The items are rated on a five point semantic differential scale. The Body Evaluation Scale consists of 12 items that measure feelings about body shape on a five point Likert scale ranging from “strongly agree” to “strongly disagree.” Rosenberg’s Self-Esteem Scale consists of 10 items on a four point Likert scale that refer to aspects of self-esteem including pride in self, general competence, and equal worth to others.
Skinfold and circumference measurements
All skinfold and circumference measurements were made by the same research assistant throughout the study. Skinfold measurements were made at two sites using Lange callipers (Cambridge Scientific Industries, Inc., Cambridge, MD): an umbilical site and a suprailiac site. For the umbilical measurement, a vertical skinfold was taken one inch to the right of the umbilicus. For the suprailiac skinfold, a diagonal skinfold was taken just above and slightly forward of the iliac crest. Three measurements were taken at each site and the closest two measurements were averaged for use in the analysis.
Abdominal and waist circumferences were measured using a steel tape measure. For the abdomen, the smallest horizontal circumference was measured in the area between the ribs and the iliac crest: the level of the natural waist. The waist circumference was measured horizontally at the level of the umbilicus. Two measurements were taken at each site and the average of the two measurements was used in the analysis.
Front to back anthropometry
The diameter of the torso at the level of the largest protrusion of the abdomen was measured using a pair of large, sliding calipers. The measurement was made from the side, with the anthropometer blades in contact with the middle of the spinal column in the back and just touching the abdomen in the front. Two measurements were taken and the average of the two measurements was used in the analysis.
Abdominal endurance
Abdominal endurance was assessed using the American College of Sports Medicine (ACSM) paced curl-up test (Figure 1). The test was conducted using a prerecorded audiotape. The subject laid supine on a padded exercise mat, with knees bent at 90 degrees (as verified via a goniometer) and both arms extended to the sides with fingers touching a piece of masking tape. A second piece of tape was placed 12 cm beyond the first. At the start of the tape (cadence of 40 curl-ups per minute), the subjects lifted their shoulder blades off the mat and slid their fingers forward until their fingertips touched the second strip of tape. Subjects performed as many curl-ups as possible without stopping. The test was terminated when the subjects could no longer keep up with the cadence or could not reach the second strip of tape. The prerecorded audiotape included 6 warm-up repetitions before the actual test began.
Figure 1.
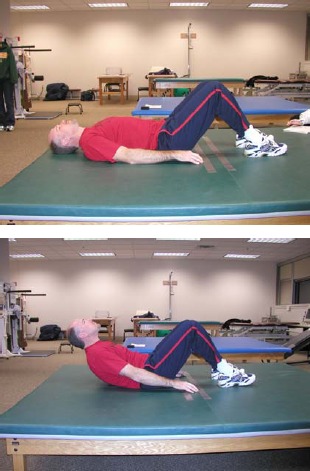
Starting and ending positions for the muscular endurance tests.
Abdominal strength
Abdominal strength was assessed using an isokinetic dynamometer (Cybex 6000, USA, Figure 2). The subject laid supine on a movable bench in a bent knee position. The lever arm of the isokinetic dynamometer was set at 180 degrees (horizontal with the ground) and the padded extension was placed just below the nipple line on the lower third of the sternum. The height of the bench was adjusted for each subject so that the extension arm remained at 180 degrees. Each subject was given several practice trials to make sure the position of the lever arm was comfortable on their chest. Subjects then performed five isometric contractions, with approximately 30 seconds between each repetition. The average torque for the highest two repetitions was used in the analysis.
Figure 2.
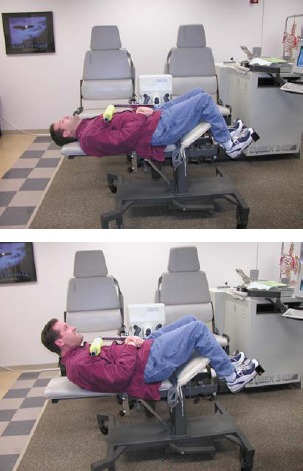
Starting and ending positions for the isometric strength test.
Training
Subjects in the stimulation group underwent stimulation 5 times per week for 8 weeks. The abdominal stimulation system consisted of a contoured neoprene belt with detachable, pre-gelled electrodes that are connected to the stimulator without externally visible leads. The electrodes were replaced at the end of the 3rd and 6th weeks of the study. Each subject was given their own belt and had to attend a minimum of two supervised sessions per week for the first 2 weeks of the study, and one supervised session per week for the remainder of the study. All other sessions were conducted on their own. During each stimulation session, subjects were encouraged to increase the amplitude on the stimulator to the highest tolerable level in order to achieve the strongest possible contractions. They were instructed not to perform volitional contractions in conjunction with the stimulator and were allowed to conduct the stimulation sessions in any positions they preferred. After every session, the subject recorded the average level of intensity used as well as the peak intensity achieved during that session.
During Week 1, the subjects completed two sessions using Program 1 (20 minutes per session), and three sessions using Program 2 (25 minutes per session). During Weeks 2-4, the subjects used Program 3 (30 minutes per session) for all of their stimulation sessions. During Weeks 5-8, subjects used Program 4 (40 minutes per session) for all of their stimulation sessions (Table 1).
Table 1.
Slendertone FLEXTM stimulator parameters.
| Time | Frequency | Pulse Duration | On Time | Rump Up | Ramp Down | Off Time | Interphase Delay | |
|---|---|---|---|---|---|---|---|---|
| min | Hz | msec | sec | sec | sec | sec | μsec | |
| Program 1 | ||||||||
| Warm-up | 1 | 70 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Treatment | 18 | 70 | 200 | 2.5 | 2.0 | 2.0 | 2.5 | 140 |
| Cool-down | 1 | 70 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Program 2 | ||||||||
| Warm-up | 1 | 60 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Treatment | 23 | 60 | 200 | 3.5 | 2.0 | 2.0 | 3.5 | 140 |
| Cool-down | 1 | 60 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Program 3 | ||||||||
| Warm-up | 1 | 50 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Treatment | 28 | 50 | 200 | 4.5 | 2.0 | 2.0 | 4.5 | 140 |
| Cool-down | 1 | 50 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Program 4 | ||||||||
| Warm-up | 1 | 50 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
| Treatment | 38 | 50 | 200 | 5.5 | 2.0 | 2.0 | 5.5 | 140 |
| Cool-down | 1 | 50 | 200 | 2.0 | 2.0 | 2.0 | 2.0 | 140 |
Statistics
Differences between groups, gender, and time (Pre-test, 4 Week, and 8 Week) were assessed using a 3-way ANOVA with repeated measures for each variable. Differences within each group were assessed using a 2-way ANOVA (gender X time) with repeated measures. If there was a significant F ratio, Tukey’s post-hoc tests were used to assess pair- wise comparisons. Differences in change scores between the control and stimulation groups at each time point (Pre-test to 4 Week and Pre-test to 8 Week) were assessed using independent t-tests with a Bonferoni adjustment of the alpha level (.05).
Results
All 41 subjects successfully completed the study. Data for one male in the stimulation group were not used in the analysis, due to unreliable testing results. Descriptive characteristics of the subjects who were used in the analysis are presented in Table 2. The only significant difference between the groups at the start of the study was in age, with the control group being significantly younger than the stimulation group.
Table 2.
Descriptive characteristics of the subjects at the beginning of the study. Data are means (±SD).
| Groups | Gender | Age (yrs) | Height (m) | Weight (kg) | BMI |
|---|---|---|---|---|---|
| Stimulation | Males (n=12) | 44 (4) * | 1.78 (.05) | 88.1 (7.0) | 28.1 (2.1) |
| Females (n=12) | 45 (4) * | 164 (.05) | 69.3 (7.0) | 26.0 (2.7) | |
| Control | Males (n=8) | 39 (8) | 177 (.06) | 83.0 (8.6) | 26.5 (2.6) |
| Females (n=8) | 40 (6) | 163 (.05) | 67.1 (6.5) | 25.3 (2.9) |
* Significantly different than Control group (p < 0.05).
The stimulation group was urged to use as high an intensity as possible on the stimulator in order to elicit the most vigorous contractions. The average intensity and the peak intensity for each workout were recorded in a daily log. A weekly summary of the data is presented in Table 3. Subjects were also asked to rate the strength of the contraction they felt they were getting from the stimulator on a scale of 0-10 (0 = no contraction, 10 = maximal tolerable contraction). At the mid-point in the study, subjects rated the strength of contraction as 8.2 ± 1.2. At the end of the study, subjects rated the strength of contraction as 8.5 ± 1.5.
Table 3.
Stimulator average and peak intensity values used during the study. Data are means (±SD).
| Week | Males | Females | Overall | |
|---|---|---|---|---|
| 1 | Average | 61 (20) | 64 (16) | 62 (17) |
| Peak | 71 (20) | 77 (15) | 74 (17) | |
| 2 | Average | 80 (15) | 84 (13) | 82 (14) |
| Peak | 90 (15) | 93 (10) | 91 (13) | |
| 3 | Average | 87 (12) | 88 (11) | 87 (11) |
| Peak | 94 (12) | 95 (6) | 95 (10) | |
| 4 | Average | 90 (8) | 90 (10) | 90 (9) |
| Peak | 97 (6) | 98 (4) | 97 (5) | |
| 5 | Average | 93 (4) | 92 (9) | 93 (7) |
| Peak | 99 (1) | 98 (3) | 98 (2) | |
| 6 | Average | 94 (3) | 93 (9) | 93 (7) |
| Peak | 99 (0) | 98 (3) | 99 (2) | |
| 7 | Average | 95 (2) | 93 (9) | 94 (6) |
| Peak | 99 (0) | 98 (3) | 99 (2) | |
| 8 | Average | 95 (3) | 93 (8) | 94 (6) |
| Peak | 99 (0) | 98 (3) | 99 (2) |
Changes in abdominal strength and endurance are presented in Table 4. The stimulation group had 58% improvement in isometric abdominal strength over the course of the study. The control group did not change. Results were similar for both males and females.
Table 4.
Changes in body composition measures over the course of the study. Data are means (±SD).
| Variables | Groups | Pre-test | 4 Week | 8 Week | |
|---|---|---|---|---|---|
| Body Weight (kg) | Stimulation | Males | 88.1 (7.0) | 88.1 (7.4) | 87.6 (7.8) |
| Females | 69.3 (7.0) | 69.5 (6.3) | 67.0 (6.6) | ||
| Overall | 78.7 (11.8) | 78.8 (11.7) | 78.3 (11.9) | ||
| Control | Males | 83.0 (8.6) | 83.7 (8.6) | 84.0 (8.9) | |
| Females | 67.1 (6.5) | 67.1 (6.3) | 66.6 (6.0) | ||
| Overall | 75.0 (11.0) | 75.4 (11.3) | 75.3 (11.6) | ||
| Body Mass Index | Stimulation | Males | 28.1 (2.1) | 28.1 (2.3) | 27.9 (2.4) |
| Females | 25.6 (2.7) | 26.0 (2.5) | 25.9 (2.6) | ||
| Overall | 27.0 (2.6) | 27.0 (2.6) | 26.9 (2.7) | ||
| Control | Males | 26.5 (2.6) | 26.7 (2.5) | 26.8 (2.6) | |
| Females | 25.3 (2.9) | 25.3 (2.9) | 25.1 (2.9) | ||
| Overall | 25.9 (2.8) | 26.0 (2.7) | 26.0 (2.8) | ||
| Umbilical Skinfold(mm) | Stimulation | Males | 29.0 (4.1) | 28.9 (4.1) | 30.0 (3.7) |
| Females | 22.1 (5.0) | 22.2 (5.5) | 22.9 (5.1) | ||
| Overall | 25.6 (5.7) | 25.6 (5.8) | 26.4 (5.7) | ||
| Control | Males | 28.6 (7.3) | 29.3 (7.1) | 28.9 (6.9) | |
| Females | 22.3 (6.2) | 22.5 (5.3) | 21.7 (5.7) | ||
| Overall | 25.4 (7.3) | 25.9 (7.0 | 25.3 (7.1) | ||
| Suprailiac Skinfold (mm) | Stimulation | Males | 15.4 (3.4) | 14.4 (3.3) | 15.0 (3.4) |
| Females | 15.8 (5.0) | 14.9 (5.0) | 15.0 (5.4) | ||
| Overall | 15.6 (4.2) | 14.7 (4.2) | 15.0 (4.4) | ||
| Control | Males | 14.9 (3.4) | 14.0 (4.7) | 15.0 (3.4) | |
| Females | 15.1 (4.8) | 15.5 (4.4) | 15.4 (3.7) | ||
| Overall | 15.0 (4.3) | 14.8 (4.4) | 15.2 (4.0) | ||
| Abdominal Circumference (cm) | Stimulation | Males | 96.6 (4.6) | 96.3 (5.3) | 94.1 (6.0) *# |
| Females | 82.4 (6.3) | 82.3 (5.3) | 79.6 (5.4) *# | ||
| Overall | 89.5 (9.0) | 89.3 (8.9) | 86.9 (9.3) *# | ||
| Control | Males | 91.8 (6.7) | 91.7 (7.4) | 91.9 (6.9) | |
| Females | 81.6 (6.4) | 81.5 (8.0) | 81.0 (7.3) | ||
| Overall | 86.7 (8.2) | 86.6 (9.1) | 86.4 (8.9) | ||
| Waist Circumference (cm) | Stimulation | Males | 101.2 (4.2) | 99.8 (5.0) | 97.9 (5.5) *# |
| Females | 92.2 (5.9) | 90.1 (6.4) * | 88.4 (7.7) *# | ||
| Overall | 96.7 (6.8) | 94.9 (7.5) *# | 93.1 (8.1) *# | ||
| Control | Males | 94.8 (6.7) | 94.9 (7.4) | 94.8 (7.1) | |
| Females | 86.5 (7.8) | 86.3 (8.2) | 86.0 (7.0) | ||
| Overall | 90.7 (8.2) | 90.6 (8.8) | 90.4 (8.2) | ||
| Front-to-Back Anthropometry (cm) | Stimulation | Males | 25.8 (1.4) | 24.8 (1.7) | 24.3 (2.1) * |
| Females | 23.1 (2.1) | 22.4 (2.2) | 22.0 (2.6) | ||
| Overall | 24.5 (2.2) | 23.6 (2.3) * | 22.0 (2.6) | ||
| Control | Males | 24.3 (2.9) | 23.8 (3.0) | 23.9 (2.6) | |
| Females | 23.0 (2.8) | 21.3 (2.6) | 21.3 (2.3) | ||
| Overall | 23.0 (2.8) | 22.6 (3.0) | 22.6 (2.7) |
* Significantly different than Pre-test (p < 0.05).
# Change for the Stimulation group is significantly different than the Control group at the same time point (p < 0.05).
Both the stimulation and control groups increased their abdominal endurance over the course of the 8 weeks. The stimulation group increased by 100% and the control group increased by 28%, yielding a net improvement of 72% for the experimental group. Results again were similar for males and females.
Data regarding body composition measures are presented in Table 5. There were no significant changes in body weight, Body Mass Index, umbilical skinfold, or suprailiac skinfold for either group over the course of the study. Overall, abdominal circumference decreased by 2.6 cm and waist circumference decreased by 3.6 cm in the stimulation group, with results being similar for males and females. The control did not change over the course of the study. There was also a significant decrease in the front-to-back diameter (1.4 cm) of the mid-section in the stimulation group. There were no changes in abdominal circumference, abdominal circumference, or front-to-back diameter in the control group.
Table 5.
Changes in abdominal strength and endurance over the course of the study. Data are means (±SD).
| Variables | Groups | Pre-test | 4 Week | 8 Week | |
|---|---|---|---|---|---|
| Abdominal Strength (N·m) | Stimulation | Males | 75.5 (27.3) | 99.9 (25.4) *# | 119.3 (25.0) *# |
| Females | 37.6 (13.6) | 51.5 (15.7) * | 59.0 (12.7) *# | ||
| Overall | 56.6 (28.7) | 75.8 (32.2) *# | 89.2 (36.4) *# | ||
| Control | Males | 78.4 (17.4) | 82.2 (16.9) | 84.9 (19.1) | |
| Females | 41.1 (10.7) | 45.6 (8.5) | 45.6 (9.8) | ||
| Overall | 59.7 (23.8) | 63.9 (22.9) | 65.2 (25.1) | ||
| Abdominal Endurance (repetitions) | Stimulation | Males | 39 (20) | 61 (40) | 80 (53) *# |
| Females | 31 (11) | 43 (10) | 60 (27) *# | ||
| Overall | 35 (16) | 52 (30) *# | 70 (42) *# | ||
| Control | Males | 34 (17) | 36 (16) | 44 (17) | |
| Females | 29 (14) | 29 (14) | 38 (15) | ||
| Overall | 32 (15) | 32 (14) | 41 (16) * |
* Significantly different than Pre-test (p<.05)
# Change for the Stimulation group is significantly different than the Control group at the same time point (p<.05)
Total scores for the three questionnaires are presented in Table 6. Results for both the Shape Evaluation Scale and the Body Satisfaction Scale were identical. Males and females had significant improvements in their scores at both the 4 Week and 8 Week testing points, and these changes were significantly greater than the control group. Consistent with these results were the answers to two other questions that were presented to subjects in written form at the end of the study. Subjects were asked if they felt their abdominal muscles felt more “firm” and “toned” after using the Slendertone FLEXTM for 8 weeks. All 24 subjects responded positively. They were also asked if they felt that their posture had improved as a result of using the Slendertone FLEXTM. Thirteen of the 24 subjects (54%) responded that they felt it had improved their posture. There was not a significant improvement in the total score for the Self-Esteem Scale (Table 6).
Table 6.
Changes in questionnaire responses over the course of the study. Data are means (±SD).
| Variables | Groups | Pre-test | 4 Week | 8 Week | |
|---|---|---|---|---|---|
| Shape Evaluation Scale | Stimulation | Males | 23.9 (3.5) | 30.5 (3.5) *# | 32.8 (2.9) *# |
| Females | 19.7 (4.4) | 26.0 (6.9) *# | 30.1 (7.2) *# | ||
| Overall | 21.8 (4.5) | 28.3 (5.2) *# | 31.5 (5.5) *# | ||
| Control | Males | 27.4 (6.5) | 28.5 (6.5) | 28.9 (6.3) | |
| Females | 22.1 (3.8) | 22.6 (2.5) | 24.0 (3.5) | ||
| Overall | 24.8 (5.8) | 25.6 (5.6) | 26.4 (5.5) | ||
| Body Satisfaction Scale | Stimulation | Males | 28.3 (5.6) | 37.2 (6.1) *# | 39.7 (6.2) *# |
| Females | 28.6 (4.5) | 36.7 (7.7) *# | 38.3 (8.2) *# | ||
| Overall | 28.4 (5.0) | 36.7 (6.8) *# | 39.0 (7.1) *# | ||
| Control | Males | 32.0 (5.8) | 30.3 (6.0) | 32.0 (5.6) | |
| Females | 30.0 (5.5) | 32.1 (5.8) | 32.1 (5.9) | ||
| Overall | 31.0 (5.5) | 31.2 (5.7) | 32.1 (5.6) | ||
| Self-Esteem Scale | Stimulation | Males | 33.6 (5.8) | 34.3 (4.5) | 34.9 (4.7) |
| Females | 36.3 (3.5) | 36.7 (3.6) | 37.1 (2.7) | ||
| Overall | 34.9 (4.8) | 35.5 (4.2) | 36.0 (3.9) | ||
| Control | Males | 32.3 (3.2) | 31.1 (2.6) | 31.0 (3.1) | |
| Females | 34.5 (2.6) | 33.0 (3.0) | 32.8 (3.3) | ||
| Overall | 33.4 (3.0) | 32.1 (2.9) | 31.9 (3.2) |
* Significantly different than Pre-test (p < 0.05).
# Change for the Stimulation group is significantly different than the Control group at the same time point (p < 0.05).
Discussion
The results of this study found that NMES significantly increased the isometric strength and dynamic endurance of the abdominal musculature. The strength gain of 58% is almost double that found by other researchers (Alon et al., 1987; 1992; Alon and Taylor, 1997; Ballantye and Donne, 1999). The most obvious explanations for this finding is that the length of the current study was 8 weeks, versus 4 weeks in studies conducted in Alon’s laboratory. The length of the study conducted by Ballantyne and Donne was 6 weeks in length, and their data suggested that the benefits of NMES tended to plateau after 4 weeks. In the current study a plateau was not realized. Strength improved by an average of 34% after 4 weeks and increased another 24% in the subsequent 4-week period. Another plausible explanation for this discrepancy is that the stimulation protocol was different between the two studies. In the current study stimulator “on time” increased from 4.5 to 5.5 seconds after the 4th week, and the length of the stimulations sessions increased from 30 minutes to 40 minutes. In the study by Ballantyne and Donne, stimulation parameters stayed constant throughout the 42-day period.
For abdominal endurance, the stimulation group had a 100% increase in curl-up performance. However, the control also had a 28% increase over the 8-week study period. The increase in the control group was attributed to a learning effect and was subsequently subtracted from the results of the stimulation group to yield a net improvement of 72%. Alon et al. (1987) did not find a significant improvement in abdominal endurance following NMES applied to the abdominals. However, the endurance task was a timed isometric holding task that was terminated based on decreased torque development. Goniometer fluctuation caused by thorax movements made decisions to terminate the test unreliable, as evidenced by the fact that the control group had a 112% increase in holding time (versus 144% in the stimulation group, p > 0.05). Ballantype and Donne (1999) did find highly significant improvements in isometric endurance of 154% and 114% at joint angles of 0° and 10° percent, respectively. They also found a 33% increase in dynamic abdominal endurance when using an incremental, timed curl-up test. The inconsistent results are probably a reflection of the fact that methods and procedures for testing and training varied considerably between studies.
The stimulation group also had a 2.6 cm decrease in abdominal circumference, a 3.6 cm decrease in waist circumference, and a 1.4 cm decrease in front-to-back diameter. These changes were significant in that they occurred despite any changes in body weight or umbilical or suprailiac skinfolds. None of the other studies reviewed found significant changes in girth measurements as a result of NMES. However, most of the other studies (Currier and Mann, 1983; Porcari et al., 2002; Romero et al., 1982) measured thigh girth. An increase in strength of the thighs would not be expected to decrease circumference of the thighs muscles in the absence of significant weight loss. If anything, the resultant hypertrophy would be manifest as an increase in thigh girth.
An increase in the strength of the abdominal muscles could theoretically reduce the circumference of the mid-section. Since, one of the roles of the abdominal musculature is to support the abdominal contents, it follows that strengthening the abdominal muscles could in effect “pull in” the abdomen, much like a girdle. This effect would decrease both the circumference and front-to-back diameter of the waist. In support of the decrease in waist circumference was the fact that 13 out of 24 (54%) subjects in the stimulation group felt that their cloths fit better around the mid-section at the conclusion of the study. None of the control group subjects reported any change in how their clothes fit.
Another role of the abdominal muscles is to maintain posture (Juker et al., 1998; Mulhearn and George, 1999). Thirteen of the 24 (54%) subjects felt that using NMES improved their posture. This is theoretically possible if the increase in strength of the abdominal muscles pulled the pelvis up in the front, thus decreasing the spinal curve in the lower back.
Perceptually, every one of the subjects felt that their abdominal muscles felt more “firm” and “toned” after using NMES for 8 weeks. These feelings were supported by significant improvements on the scores for the Body Shape Scale and the Body Satisfaction Scale. These results are in agreement with the findings of Caulfield et al. (2002) and Cullinane et al. (2002), who also found abdominal NMES to provide self-perceived benefits.
Despite the fact that subjects perceived their abdomens to be more firmed and toned, they did not have significant improvements in their self-esteem. Individual items on the self-esteem questionnaire indicated that the subjects did not feel more confident, compare their shape more favorably to others, or feel healthier after completing the study. This was probably due to the fact that even though the subjects felt that their abdomens were stronger and firmer, they didn’t perceive themselves to look any different because they did not lose any subcutaneous fat.
The big question is: Why did this study have such positive results when studies using other commercially available NMES products found little improvement in many of the same parameters? The answer probably is related to the strength of the electrically induced contractions attained by subjects in the current study. In order to improve the strength of a muscle, whether through resistance training or NMES, the muscle must be overloaded above a critical threshold. While this threshold can be as low as 30% of MVC in deconditioned individuals (Mueller, 1959), it must typically be in the range of 60-80% of MVC to induce changes (Currier and Mann, 1983; Selkowitz, 1989; Soo et al., 1988). The studies that have shown a positive benefit using NMES (Currier and Mann, 1983; Muffiuletti, 2002; Selkowitz, 1985) have all utilized contractions in excess of 60% of pre-training MVC. Selkowitz (1985) reported a strong relationship between the % MVC utilized for training and the magnitude of strength improvement. In the study by Porcari et al. (2002) that found no benefit of NMES, the elicited contractions were less than 20% of MVC.
In the current study, the strength of contraction was not assessed directly, but subjects were asked to rate the strength of contraction they felt they were receiving on a scale of 0 (no contraction) to 10 (maximal tolerable contraction). Subjects rated the contractions as 8.2 at the mid-point of the study and 8.5 at the conclusion of the study. While it is impossible to translate this into a % MVC value, it is obvious that subjects were obtaining forceful contractions.
The ability of the product used in this study to elicit strong contractions is most likely due to two factors. First, the NMES unit uses large, pre-gelled electrodes. Thus, the electrical current applied to the muscle is spread out over a large area. In the study by Porcari et al. (2002), the electrodes were made of rubber and water was used as the conducting medium. This made the electrically induced contractions very uncomfortable. Second, the stimulator used in the current study has a “ramp” function built into it. In other words, rather than suddenly coming on and then suddenly going off, the current builds up to the desired level, stays there for the programmed time, and then slowly dissipates. The combination of the above two factors made the stimulation much easier to tolerate and allowed users to obtain very strong muscular contractions.
Conclusions
This study found that the use of the Slendertone FLEXTM belt significantly increased abdominal strength and endurance, decreased waist girth, and improved self-perceived abdominal firmness and tone. The results probably can be attributed to the strength of the electrically induced muscle contractions made possible by the quality of the electrodes utilized in the belt system, as well as the stimulator itself. Future studies may want to compare the benefits of using NMES using this product to those of performing abdominal curls, matching the number of contractions performed. Additionally, studies may want to explore the potential benefits of using NMES on abdominal strength and endurance in individuals who have low back pain and are unable to perform traditional abdominal exercises.
Acknowledgements
The authors would like to thank Compex Technologies (Minneapolis, Minnesota) for proving the funding and abdominal stimulation belts used in this study.
Biographies

John PORCARI
Employment
Professor, Department of Exercise and Sports Science, University of Wisconsin - La Crosse
Degree
PhD
Research interests
Clinical exercise physiology, fitness equipment testing, cardiac rehabilitation
E-mail: porcari.john@uwlax.edu
Jennifer MILLER
Employment
Graduate student, University of Wisconsin - La Crosse
Degree
MS
Research interests
Clinical exercise physiology
Kelly CORNWELL
Employment
Graduate student University of Wisconsin - La Crosse
Degree
MS
Research interests
Clinical exercise physiology
Carl FOSTER
Employment
Professor, Department of Exercise and Sports Science, University of Wisconsin - La Crosse
Degree
PhD
Research interests
Clinical exercise physiology, speed skating, elite athletes
E-mail: foster.carl@uwlax.edu
Karen MCLEAN
Employment
Professor, Department of Physical Therapy, University of Wisconsin - La Crosse
Degree
PhD
Research interests
Therapeutic modalities, exercise physiology
E-mail: mclean.kare@uulax.edu
Tom KERNOZEK
Employment
Professor, Department of Physical Therapy, University of Wisconsin - La Crosse
Degree
PhD
Research interests
Therapeutic modalities, lectromyography, exercise physiology
E-mail: kernozek.thom@uwlax.edu
References
- Alon G., Frederickson R., Gallagher L., Rehwoldt C.T., Guillen M., Putnam Pement M.L., Barhart J.B. (1992) Electrical stimulation of the abdominals: The effects of three versus five weekly treatments. Journal of Clinical Electrophysiology 4, 5-11 [Google Scholar]
- Alon G., McCombe S.A., Koutsantinis S., Stumphauzer L.J., Burgwin K.C., Parent M.M., Bosworth R.A. (1987) Comparison of the effects of electrical stimulation and exercise on abdominal musculature. The Journaal of Orthopaedic and Sports Physical Therapy 8, 567-573 [DOI] [PubMed] [Google Scholar]
- Alon G., Taylor D.J. (1997) Electrically elicited minimal visible tetanic contraction and its effect on abdominal muscles strength and endurance. European Journal of Physical Medicine and Rehabilitation 7, 2-6 [Google Scholar]
- Ballantyne E., Donne B. (1999) Effects of neuromuscular electrical stimulation on static and dynamic abdominal strength and endurance in healthy males. Sports Sciene, 431 [Google Scholar]
- Balogun J.A., Onilari O.O., Akeju O.A., Marzouk D.K. (1993) High voltage electrical stimulation in the augmentation of muscle strength: Effects of pulse frequency. Archives in Physical Medicine and Rehabilitation, 74, 910-916 [PubMed] [Google Scholar]
- Caulfield B., Cullinane C., White C., Monique C. (2002) The effects of CSI electrical muscle stimulation on strength of the quadriceps femoris and hamstring muscles and on body satisfaction: A controlled study. Unpublished, Bio-Medical Research Institute, Dublin, Ireland [Google Scholar]
- Cullinane C., Caulfield B., Monique C., White C. (2002) The effects of CSI electrical muscle stimulation of the abdominal muscles and walking on body image and abdominal muscle strength. Unpublished, Bio-Medical Research Institute, Dublin, Ireland [Google Scholar]
- Currier D.P., Mann R. (1983) Muscular strength development by electrical stimulation in healthy individuals. Physical Therapy 63, 915-921 [DOI] [PubMed] [Google Scholar]
- Green D. (2002) FTC takes action against electrical ab belt manufacturers. ACE Fitness Matters July/August, 13 [Google Scholar]
- Juker D., McGill S.M., Kropf P., Steffen T. (1998) Quantitative intramuscular myoelectric activity of lumbar portions of psoas and abdominal wall during a wide variety of tasks. Medicine and Science in Sports and Exercise, 30, 301-310 [DOI] [PubMed] [Google Scholar]
- Kots Y. (1977). Electrostimulation of skeletal muscles. Canadian Soviet Exchange Symposium, Concoria Univeristy [Google Scholar]
- Maffiuletti N.A. Dugnani S. Folz M., Di Pierno E. Mauro F. (2002) Effect of combined electrostimlation and plyometric training on vertical jump height. Medicine and Science in Sports and Exercise, 34, 1638-1644 [DOI] [PubMed] [Google Scholar]
- Mueller E.A. (1959) Training muscle strength. Ergonomics 2, 216-222 [Google Scholar]
- Mulhearn S., George K. (1999) Abdominal muscle endurance and its association with posture and low back pain. Physioltherapy 85, 210-216 [Google Scholar]
- Porcari J.P., Palmer McLean K., Foster C., Kernozek T., Crenshaw B., Swenson C. (2002) Effects of electrical muscle stimulation on body composition, muscle strength, and physical appearance. Journal of Strength and Conditioning Association Research 16, 165-172 [PubMed] [Google Scholar]
- Romero J.A., Sanford T.L., Schroeder R.V., Fahey T.D. (1982) The effects of electrical stimulation of normal quadriceps on strength and girth. Medicine and Science in Sports and Exercise, 14, 194-197 [PubMed] [Google Scholar]
- Rosenberg M. (1989) Society and the adolescent self-image, Revised edition Middletown: Wesleyan University Press [Google Scholar]
- Selkowitz D.M. (1985) Improvements in isometric strength of the quadriceps femoris muscle after training with electrical stimulation. Physical Therapy 65, 186-196 [DOI] [PubMed] [Google Scholar]
- Selkowitz D.M. (1989) High frequency electrical stimulation in muscle strengthening. American Journal of Sports Medicine 17, 103-111 [DOI] [PubMed] [Google Scholar]
- Soo C.L., Currier D.P., Threlkeld A.J. (1988) Augmenting voluntary torque of healthy muscle by optimization of electrical stimulation. Physical Therapy 68, 333-337 [DOI] [PubMed] [Google Scholar]