

Abstract
Background
Bone fracture treatment usually involves restoring of the fractured parts to their initial position and immobilizing them until the healing takes place. Drilling of bone is common to produce hole for screw insertion to fix the fractured parts for immobilization. Orthopaedic drilling during surgical process causes increase in the bone temperature and forces which can cause osteonecrosis reducing the stability and strength of the fixation.
Methods
A comprehensive review of all the relevant investigations carried on bone drilling is conducted. The experimental method used, results obtained and the conclusions made by the various researchers are described and compared.
Result
Review suggests that the further improvement in the area of bone drilling is possible. The systematic review identified several consequential factors (drilling parameters and drill specifications) affecting bone drilling on which there no general agreement among investigators or are not adequately evaluated. These factors are highlighted and use of more advanced methods of drilling is accentuated. The use of more precise experimental set up which resembles the actual situation and the development of automated bone drilling system to minimize human error is addressed.
Conclusion
In this review, an attempt has been made to systematically organize the research investigations conducted on bone drilling. Methods of treatment of bone fracture, studies on the determination of the threshold for thermal osteonecrosis, studies on the parameters influencing bone drilling and methods of the temperature measurement used are reviewed and the future work for the further improvement of bone drilling process is highlighted.
Keywords: Bone fracture, Bone drilling, Immobilization, Thermal osteonecrosis
1. Introduction
Bone is a calcified connective tissue forming the major portion of the skeleton of most vertebrates. A bone is said to be fractured if there is a break in its continuity. Fractured bones are capable to heal itself by producing new bone forming cells and blood vessel at the fracture site. There are two basic approaches for bone fracture treatment.1
-
1)
Conventional approach
-
2)
Direct approach
In conventional approach the setting and immobilization of the fractured parts is done from outside whereas direct approach implicates the internal fixation of fractures using immobilization screws, wires and plates. The limitation of the conventional approach lies in the fact that the parts cannot be optimally aligned, in some cases the alignment from outside is not possible and the healing takes a long time.1 These limitations are overcome by direct approach in which bone drilling is a common operation for internal fixation of fracture by immobilization screws or for prosthetic device installation. Fig. 1 shows a bone drilling operation in which drill makes hole in the bone, by removing the material from it.2
Fig. 1.
Process of bone drilling and temperature measurement without coolant.2
During this process temperature rises which can result in bone necrosis i.e. irreversible death of the bone cells when the temperature increases above a threshold.3–5 The compressive force acting on the fixation usually demands for high degree of stability of the fixating screws. To ensure this stability the threads of the screw must engage or grip the bone enclosing the drilled hole. But necrosis causes breakdown of bone around the implantation site leading to the loosening of fixation.6 Thus the method of internal fixation of fracture for faster recovery is advantageous only if the thermal necrosis of the bone can be avoided. Therefore the bone drilling studies plays a very vital role in improving the chances of avoiding thermal osteonecrosis. Few researches, mostly experimental, pertaining to establish optimum drilling conditions and drill geometry has been reported in the literature. It has been more than a half century since which the investigation on bone drilling is carried out but still there is no general agreement on the mechanical modelling of this process to determine optimum drill design and drilling parameters for avoiding bone necrosis. An attempt has been made to compile the work related to bone drilling to develop a technological database of orthopaedic drilling process. The present paper not only summarizes important studies but also reviews meticulously the area for minimizing heat and force induced bone tissue injury.
The present review is categorized into the following sections
-
1)
Studies on the determination of the threshold for thermal osteonecrosis.
-
2)
Studies on the parameters influencing the bone drilling.
-
3)
Miscellaneous factors affecting bone drilling.
-
4)
Heat generation and temperature measurement during bone drilling.
-
5)
Conclusion and future directions.
2. Studies on the determination of threshold for thermal osteonecrosis
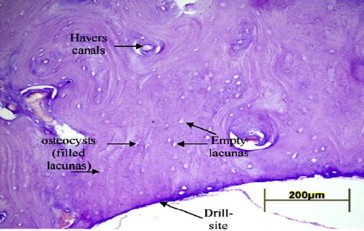
Osteonecrosis (ON) is a disease resulting from the temporary or permanent loss of blood supply to the bones. In the absence of the blood supply, the bone tissue dies and causes the bone to collapse. There are several reasons which may cause the loss of blood supply to the bones. Trauma related necrosis can result from an injury whereas non traumatic necrosis is caused due to some medications, blood coagulation disorders or excessive use of alcohol. Thermal trauma is a subtype of traumatic necrosis called as thermal necrosis of bone or thermal ON.7 ON associated with the drilling is very complex phenomenon. Apart from the thermal damage, drilling of bone can also cause micro damage to the bone. Small cracks accumulate in the mineralized matrix of bone which can cause osteocytes apoptosis.8 Death of osteocytes due to drilling may therefore increase the risk of osteonecrosis due to depletion of the osteocytes, reduction in blood flow and increased osteoclastic resorption resulting in structurally weaker bone.9 The presence of empty osteocyte lacunae is the histological distinctive characteristic of osteonecrosis3,10 as shown in Fig. 2. Necrotic bone adjacent to a pin tract is denoted by presence of empty osteocyte lacunae marked with dots. Healthy osteocytes are encircled. The line indicates the border between the present and disappeared osteocytes.10
Fig. 2.
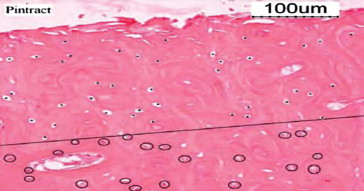
Histological image showing the status of osteocytes during drilling.10
The primary objective for carrying out these studies is to investigate the viability of bone after thermal trauma. Thermal damage to the living tissue is related to the magnitude of temperature elevation and the time for which the tissue is subjected to the damaging temperatures.11,12 The inverse relationship of thermal necrosis temperature and necrosis time for a wide range of temperature (44 °C–100 °C) was studied and it was found that an increase in temperature above 70 °C causes immediate damage of epithelial cells4 as shown in Fig. 3. Bone necrosis was consistently seen in histological sections of rabbit at temperatures greater than or equal to 70 °C.13
Fig. 3.
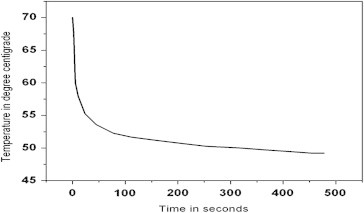
Time–temperature curve showing thermal necrosis of epithelial cells.4
Lundskog performed his studies on rabbit and stated that a temperature of 55 °C for 30 s will induce irreversible death of the bone cells.5 Bonfield and Li demonstrated that irreversible bone changes occur when dog femora were heated to 56 °C in vivo.12 Eriksson et al3 performed histological, histochemical and vital microscopic study in the rabbit and established a threshold of 47 °C for 1 min to cause thermal necrosis of the cortical bone. Also they evaluated the effects of defined temperature rise on bone regeneration and found that heating of the test implants (titanium) to 47 °C or 50 °C for 1 min caused a significant reduction in the bone formation in the implants while no significant effects were observed when the heating was done to 44 °C for 1 min.14 These results reflected the importance of controlling the heat generated during the orthopaedic surgical process that hampers the proper bone regeneration. The above experiments were not conducted on human bone. The human femoral bone tissue is different microscopically from bovine femoral tissue.15 Therefore exact threshold temperature for the death of the human cortical bone due to overheating is unknown. However, majority of the authors believes that an average temperature of 47 °C for 1 min as threshold, above which the necrosis of the human bone will take place.3,11,14,16–18 Table 1 summarizes some of the important studies on the determination of threshold for thermal osteonecrosis.
Table 1.
Investigation on the threshold for thermal osteonecrosis.
| Authors (year) | Species investigated | Conclusions |
|---|---|---|
| Moritz and Henriques (1946) | Pig |
|
| Bonfield and Li (1968) | Dog |
|
| Lundskog (1972) | Rabbit |
|
| Eriksson and Albrektsson (1983) | Rabbit |
|
3. Studies on the parameters influencing the bone drilling
The temperature generated during the bone drilling depends upon various parameters such as drill diameter, drill rotational speed, axial drilling forces, cooling etc. The most important parameters reported in the literature can be broadly divided into two groups: 1) drilling parameters and 2) drill specifications. Table 2 depicts detailed information on the parameters affecting bone drilling.
Table 2.
Parameters influencing the temperature rise during bone drilling.
| Drilling parameters | Drill specifications |
|---|---|
| Drilling speed | Drill diameter |
| Feed rate | Cutting face
|
| Drilling energy | Flutes and helix angle |
Cooling
|
Drill point
|
| Drilling depth | Drill wear |
| Predrilling |
3.1. Drilling parameters
Drilling parameters play a very vital role for controlling the temperature generated during drilling. From last few decades many researchers have investigated on this aspect so as to minimize the chances of necrosis during drilling.
3.1.1. Influence of drilling speed and feed rate
Many researches in the past have been carried out to determine the influence of drilling speed, axial drilling force and feed rate on bone drilling temperature. Most of the researchers have described it in interrelated terms of the speed of drill with force or feed applied during drilling. Therefore to make the topic better and convenient to understand for the reader all the above parameters are reviewed together.
The review on the drilling speed during bone drilling suggests no consistent trend. Some suggest low drilling speed as they showed that the temperature increases with increase in drill speed while others suggests a decrease in the temperature with increase in drill speed. Thompson19 found that the temperature increases at 2.5 mm and 5.0 mm from the drill site with increasing speed from 125 rpm to 2000 rpm during skeletal pin insertion in vivo. Vaughan and Peyton20 studied the influence of the rotational speed on temperature rise during cavity preparation and reported that with the increase in drill speed, the temperature generated increases. Matthews and Hirsch21 investigated human cadaveric femora and found that increasing the rotational speed from 345 rpm to 2900 rpm did not have any significant change in the temperature during drilling. But increasing the thrust force was associated with decrease in both maximum temperatures and their duration. They measured the effect of applied force from 19.6 N to 117.6 N along with the drill speeds varying from 345 rpm to 2900 rpm and concluded that both the temperature and time duration above 50 °C decreases as the applied load increases. These results are also shown by Augustin et al22 who concluded that the peak temperature during drilling decreases as the feed rate increases. Brisman23 reported that the drill speed of 1800 rpm and load of 1.2 produced same heat as with the drill speed of 2400 rpm and the load of 2.4 kg while drilling bovine cortical bone. Independently increasing either the speed or the load caused an increase in temperature in bone. However, increasing both the speed and the load together allowed for more efficient cutting with no significant increase in temperature. Hillery and Shuaib24 showed that there is a significant decrease in the temperatures generated during bone drilling with increasing drill speed from 400 rpm to 2000 rpm with a drill diameter of 3.2 mm. Bachus et al25 examined cadaveric femur and found that the duration and magnitude of maximum temperature decreases with increasing axial thrust force at 820 rpm. Nam et al26 found that increasing either the speed or the force resulted in temperature rise while conducting experiments on bovine ribs by applying a load of 500 g and 1000 g with a drill speed of 600 rpm and 1200 rpm. Sharawy et al27 conducted experiments using 4 thermocouple technology to measure the heat generated from three drilling speeds (1225, 1667, and 2500 rpm) and found that the mean rise in the temperature, the time of drilling and the time needed for the pig jaw bones specimen to return to the initial temperature decreases as the drilling speed increases. Apart from the studies of Matthews (1972), Hillery (1999) and Sharawy (2002) there is a general agreement in the literature that the temperature increases with drill speed approximately up to 10,000 rpm.
Histological studies were done to examine the effect of high speed rotary instruments on bone during orthopaedic surgical processes by Boyne,28 Moss29 and Spartz.30 These studies suggested that high speed drilling could cause less noxious effect to the bone than the low speed drilling. Abouzgia and James31 conducted drilling experiments on bovine femora without coolant, for forces ranging from 1.5 N to 9.0 N and drill speed of 49,000 rpm. They found that the temperature increases with force up to 4.0 N, and then decreases at forces greater than 4.0 N. They concluded that with an increase in forces heat generation rate increases but the drilling time reduces hence less heat is produced therefore higher forces has been recommended during bone drilling. But higher the axial force applied during drilling can cause micro cracks in the bone and drill breakage.32 So it is necessary to find out optimal feed rate such that the drilling force is not excessive to cause the breakage of the drill (Fig. 4) or bone damage besides maintaining the drilling time as short as possible.
Fig. 4.

A broken portion of drill bit left in situ.32
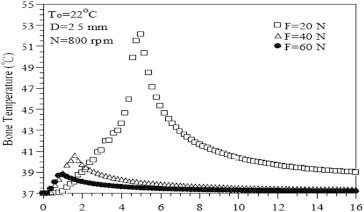
Iyer et al33 performed histological studies of rabbit tibia. They measured the heat generated in vivo during osteotomy preparation at low (2000 rpm), intermediate (30,000 rpm), and high (400,000 rpm) speeds and observed an inverse relationship between drill speed and heat generated. They also evaluated the rate and quality of healing after drilling osteotomies at the above three speeds in the mandible. The histologic findings suggested that in the initial 6 weeks, the rate of healing and quality of new bone formation are higher for high speed drilling as compared to low or intermediate speed drilling.34 In the same year Reingewirtz35 investigated the influence of various parameters on bone heating during drilling in vitro in a bovine cortical femur model. He proposed that the temperature is positively correlated with the speed in the range of 400 rpm–7000 rpm and negatively correlated with speed above 700 rpm–24,000 rpm and thereafter remains constant up to 40,000 rpm. He also concluded that for lower speeds of 400 rpm–800 rpm an enhancement in axial thrust from 80 N to 200 N has no effect on temperature generated. Udiljak et al1 carried out high speed drilling experiments on pig bone with speeds ranging between 140 m/min to 225 m/min using 4.5 mm drill (standard surgical twist drill and two-step drill) with constant feed per tooth of 0.1 mm. They concluded that for both the types of tested drill, high speed drilling (140 m/min) causes less increase in the temperature as compared to standard speed drilling (6.53 m/min). They also reported that the results of high speed bone drilling above 140 m/min don't causes a significant reduction in the temperature hence it makes no sense in increasing the speed above 140 m/min. Tu et al36 used a three dimensional elastic–plastic dynamic temperature–displacement finite element model in Abaqus to simulate the Kirschner pin and bone thermal contact during drilling process. Based on the numerical results they concluded that a larger applied force can reduce the temperature rise effectively. Tu et al37 also carried out similar simulation of drill and bone during drilling. The results showed that the temperature induced during drilling decreases with an increase in drilling speed or the applied force (Figs. 5 and 6).
Fig. 5.
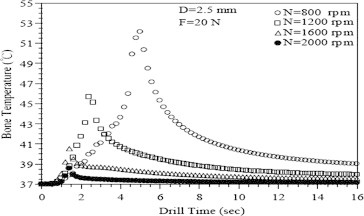
Variation of bone temperature with drill time for different rotating speeds.37
Fig. 6.
Variation of bone temperature with drill time for different forces applied.37
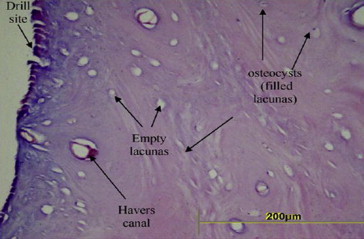
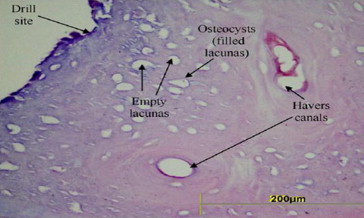
Recently the influence of drilling speed and force on temperatures generated during orthopaedic drilling process and histopathology of bovine tibia was evaluated by Karaca et al.38 They concluded from the experimental and statistical analysis that the temperature decreases with increasing drill force and decreases with increasing drill speed. The histopathological studies revealed that the volume and the amount of damage along the drilling site in the bone tissue are absolutely affecting the quality of the drilled bone and its regeneration speed along the drilling site. They showed the effect of recorded temperature in terms of osteocyte density, empty or filled lacunas, the Haversian canals and the distance between the drilled site and the filled osteocyte (Figs. 7–9).
Fig. 7.
Histogram of sample drilled with 4.5 mm drill diameter with a speed of 570 rpm and drilling force of 40 N.38
Fig. 8.
Histogram of sample drilled with 4.5 mm drill diameter with a speed of 570 rpm and drilling force of 100 N.38
Fig. 9.
The histogram of sample drilled with 4.5 mm drill diameter with a speed of 1180 rpm.38
Histogram in the Figs. 7 and 8 in which maximum temperatures generated are 83 °C and 57 °C respectively clearly indicates that at higher drill forces less temperature is produced during drilling. The histogram processed by the authors for lower drill forces were better than the histogram of higher drill temperature, in terms of filled osteocyte, which indicates lower bone damage. Also, they observed that drilling with lower speed consists of more filled osteocyte and are exposed to lower drilling temperatures as compared to drilling with the higher speeds thereby influencing the structure of bone in a negative way as shown in Figs. 8 and 9 (maximum temperature generated is 57 °C). In 2012 Lee et al39 through their experimental investigations on the effect of feed rate and drilling speed during drilling of a bovine femur showed that the maximum temperature increases with increasing spindle speed and decreases with increasing feed rate. From the above studies there is no clear indication about the optimum bone drilling speed and axial drilling force but majorities of the experimental investigations recommend high speed with larger force or feed rate for minimum temperature generation during bone drilling.
3.1.2. Drilling energy
Drilling energy is defined as the energy expensed for producing a hole. Drilling energy is directly related with the amount of heat generated during drilling. Lower cutting energy is associated with less residual and thermal damage (cracking and necrosis) in the cutting region.40 Higher the energy consumed implies higher heat generated leading to higher rise in temperature.41 Greater the forces induced during drilling implies higher drilling energy expensed to produce hole. Few researchers in the past have done the calculation of energy consumed during bone drilling. Almost all of the energy used in material removal is converted into heat.42 Jacob and Berry40 measured the torque and thrust during drilling of mature bovine tibia using several drills with different speed and feed rate. They found that at lower rotational speeds the forces are much higher as compared to the higher speeds and, as the feed is increased the forces increases. In 1976 Wiggins and Malkin43 performed an experimental investigation on bone drilling using different types of drill bits of various diameters. The drilling behaviour with constant thrust force was measured in terms of feed rate, torque and specific energy. They have identified that the clogging of drill bit causes substantial increase in the drilling torque hence increases specific cutting energy. No measurements for the temperature generated were done. Abouzgia and James41 investigated the effect of the force on the energy consumed during the drilling process using forces between 1.5 and 9.0 N and for free-running speeds from 20,000 to 100,000 rpm. The measurements of electric power showed that the total energy consumed generally decreases with increasing speed and force, primarily because of decrease in drilling time. They suggested that high drilling speed with a large force is desirable because bone temperature is reduced. Karmani and Lam44 studied the effect of rake angle on the cutting efficiency and the specific energy requirement during the bone drilling process and concluded that the selection of the optimum rake angle facilitates cutting, improves the chip flow and reduces the specific cutting energy.
3.1.3. Influence of coolant
The effect of use of coolant during bone drilling for orthopaedic surgery is investigated by many researchers22,45–48 they found that cooling is one of the most important factor as it significantly decreases the temperature induced during drilling. Two methods internal and external cooling are often employed for the supply of coolant during drilling (shown in Fig. 10(a) and (b) respectively). The types of cooling systems are7:
-
1)Internal cooling systems.
-
1.1)Closed type.
-
1.2)Open type.
-
1.1)
-
2)
External cooling systems
Fig. 10.
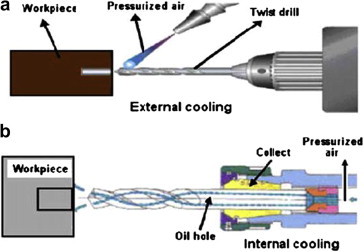
(a) External cooling and (b) internal cooling approaches.49
Internal cooling involves feeding of the coolant to the drill tip through the tubules in the drill shaft whereas external cooling involves feeding the coolant to the surface of the drill at the entry point.
In closed type internal cooling system the coolant circulates through the tunnels incorporated inside the drill and back to the central heat exchanger. Cooling is achieved by the mechanism of conduction of heat from the drill to the coolant flowing through tunnels. No contact between coolant and the bone takes place. In open type internal cooling system the coolant flows of through the tunnels in the drill and exits from the opening at the drill tip, thereby taking away the heat generated during the drilling process. Besides taking away the heat by conduction, the coolant also provides lubrication and irrigation (excluding closed loop internal cooling system).7 Lubrication reduces the friction during drilling and hence less heat is generated. Bone produces short chips when it is dry but during orthopaedic treatment it is wet therefore the chips produced get clogged which increases the friction and raises the temperature during drilling. Irrigation causes the effective removal of chips and debris which avoids clogging of flutes during bone drilling and facilitates less heat generation. Matthews and Hirsch21 studied the effect of the use of coolant during drilling of human cortical bone and found that the cooling is highly effective in limiting the maximum temperature elevations. The experimental holes were drilled while being irrigated with water at room temperature at flow rates of 300, 500 and 1000 ml per minute. They showed that higher the irrigation rate lower is the bone temperature developed during drilling and the temperature never increases beyond 50 °C for the irrigation rate of 500 ml/min or above (shown in Fig. 11).
Fig. 11.
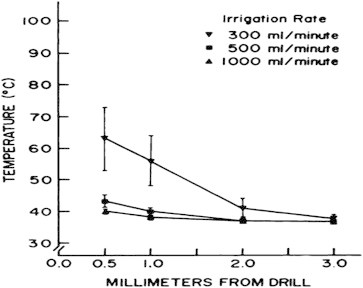
Effect of cooling rates on average maximum cortical temperatures recorded at specific distances from the drill.21
Kirschner and Meyer50 used open type internal cooling system for dental drilling. They concluded that as the internal cooling feeds the coolant at the tip of the drill, a combined rinsing and cooling effect on bone is obtained which maintains bone temperature lower as compared to temperature generated with external or no cooling. Lavelle and Wedgwood45 performed an in vitro study at low rotational speed of 350 rpm with force of 19 N and showed that internal irrigation reduces the temperature more effectively when compared to external irrigation. Haider et al46 performed histographical studies on sheep and compared the effects of external and internal cooling. They concluded that external irrigation is more effective on the surface whereas internal irrigation in the depth. Effectiveness of internal irrigation compared to external irrigation increases as the depth increases. But Benington et al47 in their experiment observed the thermal changes at implant sites with internal and external cooling and found no appreciable difference in the temperate generated. So they concluded that there is no benefit of expensive internal irrigation system over the external irrigation. Kalidindi48 observed a significant rise in temperature during drilling without coolant. He performed various experiments with external cooling to observe its impact on drilling temperature and found that the external cooling reduces the temperature generated during drilling. Augustin et al22 carried out drilling experiments on porcine femora to evaluate the influence of different drilling parameters on the increase of bone temperature. They concluded that cooling with water at 26 °C is the most important factor in reducing the bone temperature during drilling. Sener et al51 performed in vitro experimental studies on bovine mandible and observed that more heat is generated on the surface of the drilling cavity as compared to the bottom surface. Therefore, they suggested external irrigation can provide sufficient cooling during drilling. Besides that they also examined the effects of external irrigation using saline at 25 °C and 10 °C and found that lower coolant temperature causes lower temperature generated during bone drilling. Similar results were obtained by Al-Dabag and Sultan52 using the coolant at 5 °C and 25 °C. Augustin et al53 investigated the performance of internally cooled step drill during drilling of porcine femora. They found that with all combinations of parameters, the use of internal type irrigation system produces bone temperatures much below the threshold for thermal osteonecrosis. From the review of literature under this section it is clear that only few researchers had carried out the investigations for the comparison of the internal and external cooling and there is no clear suggestion of the better and convenient of the two to be used during bone drilling.
3.1.4. Drilling depth and cortical bone thickness
Drilling depth and cortical bone thickness also influence the temperature during drilling and both are positively correlated.24,38,39,43,48,54–56 The frictional resistance offered by the compact cortical bone to the drill causes increase in temperature. Greater the cortical thickness greater is the drilling depth and so the friction and heat generated. Eriksson et al16 performed in vivo experiments to study the temperature rise during drilling of rabbit, dog and human tibiae under similar conditions and found that the temperatures generated is highest in humans followed by dog and than in the rabbit. They concluded that the variations in the drilling temperature measured for different species were due to the difference in the mean cortical thickness. Hillery and Shuaib24 also carried out their experiments with constant drilling parameters and drill specifications for both bovine and human bone and found significantly higher temperature for the bovine bone as compared to human bones. They explained that this result is due to the difference in the mean cortical thickness of the bovine (7 mm–9 mm) and human cadaveric (3 mm–5 mm) bone. Wiggins and Malkin43 found that the temperature produced during drilling is directly proportional to the drilling depth. Since the clogging of drill flutes by bone chips causes a substantial increase in torque and friction as the drilling depth increases. Cordioli and Majzoub54 carried out their bone drilling investigations on bovine femurs with twist drills of 2 mm and 3 mm diameter running at 1500 rpm with external irrigation. They observed higher temperature at 8 mm depth as compared to 4 mm depth regardless of the drill diameter and the presence of cooling. Kalidindi48 found that the increasing behaviour of the temperature with depth is due to increase in the contact time between the workpiece and the drilling tool which increases the overall friction and hence higher heat is produced. But Tehemar55 recommended that the influence of drilling depth on the increase in temperature is not so important when open type internal cooling system is used during bone drilling. Oliveira et al56 and Lee et al39 from their investigations suggested that depth is the predominant factor influencing the temperature induced during bone drilling.
There is a general agreement in the literature that greater the drilling depth higher is the temperature generated despite of any drilling conditions and cortical bone thickness is positively correlated with the temperature generated during bone drilling.
3.1.5. Predrilling
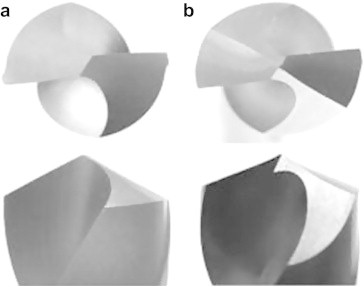
Drilling can be done either in single step or in multistep. In single step only one drill of required diameter is used to produce the desired hole whereas in multistep drilling known as predrilling, drill diameter is gradually increased from minimum to the required diameter using a number of drills. Matthews et al57 conducted experiments on human-cadaveric cortical bone to examine the effect of predrilling during drilling of bone and found that, predrilling is highly effective method of minimizing temperature elevation. Branemark58 recommended incremental drilling as it gradually removes the material from the drilling site, resulting in less friction and better heat dissipation. Itay and Tsur59 also suggested that predrilling can effectively lessen the temperature during drilling of bone. Udiljak et al1 investigated with the conventional drill and step drill (Fig. 12) and showed that the maximum bone drilling temperature was much lower in case of step drill as compared to conventional drill.
Fig. 12.
(a) A classic surgical drill and (b) step drill (two phase drill).1
Kalidindi48 also found similar results and concluded that the maximum temperature obtained using incremental drilling is far less as compared to single stretch drilling to produce same hole. They suggested that it may be due to the time gap between the change of drills during incremental drilling and hence the new drill is in cool environment as compared to the single stretch drill. They have also reported that the temperature reduction is due to the reduction in the debris to expel with step drilling, but with the predrilling there is a disadvantage of drilling time being increased resulting in extended operation time. Recently Augustin et al53 examined the temperature changes in the cortical bone during drilling with a step drill. They reported no differences in the maximum bone temperature with two-step drill as compared to the standard drill of the same diameter.
3.2. Drill specifications
Drill specifications are also a major factor influencing the temperature generation during drilling. Several researches showed that many features of drill are responsible for increase in thermal injury to the bone.22,32,60 Any drill is usually characterized by the drill diameter, cutting face, helix angle and the drill point (Fig. 13a). The drill cutting face is further specified by rake angle and clearance angle whereas point angle, flank and the chisel edge defines the drill point32 (shown in Fig. 13b).
Fig. 13.
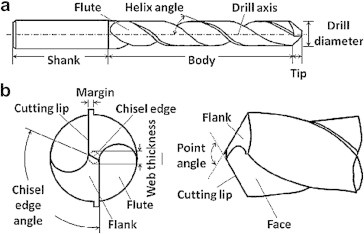
(a) Twist drill bit. (b) Drill bit tip.61
3.2.1. Drill diameter
Several researchers have carried out bone drilling experiments to determine the effect of drill diameter on the temperature generated during drilling.22,48 They found that the diameter of the drill significantly influences the drilling temperature. Kalidindi48 studied the temperatures produced while drilling with three different drills of diameters 2, 3.5 and 4.3 mm at a feed rate of 0.42 mm/s and speed of 1200 rpm. He found that the temperature increases exponentially with increasing drill diameter. Similar observation is also reported by Augustin et al22 in drilling porcine femora. They concluded that with increase in drill diameter contact surface between the bone and the drill increases resulting in the increase in overall friction and the heat produced. Larger drill hole reduces the strength of the bone and takes longer time for recovery. Bechtol et al62 suggested that the drill hole of 20% of the diameter of the bone reduces the strength by 40% of its original strength. Burstein et al63 inserted screws in the femoral diaphysis of dogs and concluded that the drill holes are present up to 12 weeks which increases the chances of refracture due to decrease in strength of the bone. They reported that reducing the diameter greatly result in the breakage or bending of drill bit during drilling. Hufner et al64 carried out investigations to see the effect of drill diameter and length on the deviation of the actual to the planned target point during bone drilling. The results suggested that drill bit deviation from the planned target point increases using small diameter and longer drill bits.
3.2.2. Cutting face
-
1)
Rake angle
-
2)
Clearance angle and flank
-
1)
Rake angle: it is defined as the angle between the cutting edge and the plane perpendicular to the workpiece. Rake angle is a critical factor influencing the cutting forces. Several investigations have been carried out to identify an optimal rake angle for bone drilling. There is a general agreement on the results obtained by Jacob et al65 that, as the rake angle increases the bone cutting forces decreases for a single edge cutting tool. Drill can be assumed to be formed by two single edge tool wrapped around a common axis,40 hence severe the rake angle lower are the cutting forces. Saha et al60 observed that the higher rake angle increases the cutting efficiency of the drill. An optimum rake of 20°–30° was recommended by Hillery and Shuaib24 as it sufficiently clears the chips and generates very low thrust force.
-
2)
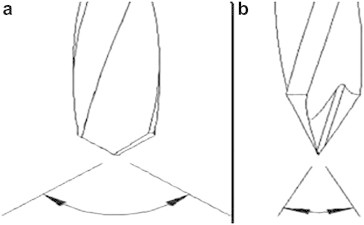
Clearance angle and flank: flank is the flat part of the drill when viewed end on (Fig. 13b). The flank of the drill represents a large surface area for friction during drilling. Clearance is the space provided to avoid undesirable contact of the flank with the workpiece. It is the angle by which the flank of the drill clears the material during drilling.32 Despite of the clearance provided the large surface of the flank results in high friction with workpiece, causes generation of the frictional heat and hence the temperature during drilling. Farnworth and Burton66 suggested a clearance angle of 15° for better cutting efficiency during bone drilling operation. Saha et al60 also recommended the same values as optimal clearance angle for bone drilling. Recently, Karmani and Lam44 investigated on the design of the surgical drill bits and demonstrated that the optimum clearance angle of the drill bit for bone drilling lies in the range of 12°–15°. Natali et al32 suggested that the friction between the flank and the bone can also be reduced by increasing the clearance angle half way along the surface termed as split point (shown in the Fig. 14). Split point causes reduction of the friction of the flank with workpiece so less heat is generated.
Fig. 14.
(a) Standard drill and (b) split point drill.
3.2.3. Flutes and helix angle
The flute is a deep groove that typically twists around the drill, giving the waste material a path out of the hole. In the absence of a flute, the drill would not cut as quickly, as the waste material would need to be removed before drilling could continue. Flutes can vary in size and the drills can be constructed with number of flutes with various helix angles. Bertollo et al67 examined 2-fluted and 3-fluted surgical drills and found that 3-fluted design offers a significant improvement over the 2-fluted design in terms of deviation from the planned target point as they have more acute tip. In 3-fluted designs the cutting edges tends to converge at a point by the virtue of symmetry (shown in Fig. 15) and also have superior bending stiffness. They emphasized that in the absence of drill-jigs and guides during orthopaedic drilling, 3-fluted drill can effectively reduce the skiving to avoid the difference in position of the intended hole or damage to the surrounding tissues.
Fig. 15.
Point angle of 2-fluted drills (a) are generally less acute than 3-fluted drills (b).68
In their further studies Bertollo et al69 highlighted that the cutting efficiency of 3-fluted designs were found to be greater than that of the 2-fluted drill, but this did not translate into a decrease in the maximum temperatures during drilling. They concluded that in 3-fluted type designs, the tendency of cutting lips to converge about a point causes the reduction of the chisel edge to a nominal value due to which the axial thrust force during drilling reduces. Despite the theoretical advantage of 3-fluted drills over 2-fluted counterparts, there is a lack of evidence in the literature in support of their use.
Helix angle of the drill is defined as the angle formed by the edge of the flute with the line parallel to drill centre line. Helix angle and rake angle of the drill bit are interrelated and larger helix angle results in a larger rake angle, which is desirable since torque and thrust during drilling decreases. Helix angle is decided in such a way that there is a compromise between the strength of the cutting edge and efficient chip ejection through the flutes.70 Helix provided on the drill bit can be slow, standard or quick depending upon the helix angle32 (shown in Fig. 16).
Fig. 16.
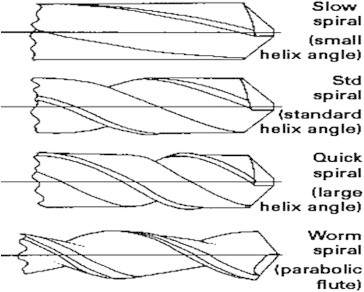
Variations in helix angle and a worm spiral drill bit.32
A slow helix or low helix have elongated drill flutes whereas high or quick helix drills have compact flutes i.e. number of turns is higher in quick helix than in slow helix. Short chipping materials are drilled with the slow helix as the debris gets cleared easily by the drill but for the kind of materials in which the chips get clogged, a quick helix is used. Most of the orthopaedic drill used presently has slow helix. Bone produces short chips when it is dry but during orthopaedic treatment it is wet with blood and marrow fat, therefore the chips produced get clogged which increases the friction and raises the temperature during drilling, hence theoretically a quick helix could be more efficient.32 For surgical drill, the range of 13°–35° helix angle are usually employed depending upon the drill diameter.60 Fuchsberger71 suggested a helix angle of 12°–14° for effective bone drilling. Farnworth and Burton66 recommended an optimal helix angle of 27° for performing an orthopaedic drilling operation. Wiggins and Malkin43 through their investigations showed that a helix angle of 28° generates much lower torque and specific cutting energy during drilling. Narashima et al70 demonstrated that the torsional rigidity varies parabolically with helix angle and reaches maximum at 28°. They suggested that due to this reason the same angle is used for wide range of applications. Davidson and James72 also concluded that the temperature decreases uniformly with increasing helix angle. They proposed parabolic flute (known as worm spiral) provides an excellent clearance of debris and hence a higher feed rate is possible with this type of flutes (shown in Fig. 14). Higher feed rate increases the rate of heat generation but reduces drilling time hence less heat is produced.32
3.2.4. Drill point
-
1)
Point angle
-
2)
Chisel edge
-
1)
Point angle: point angle for a drill is defined as the angle formed by the projection of the cutting edges on to a plane passing through the longitudinal axis of the drill (Fig. 13b). Point angle prevents the walking of the drill and enables the user to drill at the desired site. Hence an optimum point angle is desirable as using drill guide is not always possible during orthopaedic drilling. The smaller point angles produces more acute tip which can easily stab in the material preventing the walking of the drill. But with acute tip less portion of the cutting lip is involved in the cutting action in the first moments of the drilling leading to higher rise in the temperature. On the other hand larger point angles provide full contact of the cutting lip with the bone as soon as drilling starts.7 Several researchers have carried out investigations to find the influence of drill point angle on bone drilling. There is no general agreement on the optimum drill point angle. Bechtol et al62 investigated the effect of point angle during bone drilling and recommended an angle of 90°for surgical drill. Later same result was also shown by Jacobs and Berry.40 Sneath73 suggested a larger drill point angle of the range of 130°–140° to be used for orthopaedic drilling. Similarly, Farnworth and Burton66 suggested that the point angle in the range of 120°–140° gives most satisfactory performance in terms of thrust force, torque, rate of penetration and the quality of the holes. Wiggins and Malkin43 performed investigations with three different types of drill bits (surgical twist drill, general purpose twist drill and a spade drill) having different point angles and observed that the drill with a point angle of 118° generates much lower torque and energy as compared to the other two. Saha et al60 and Natali et al32 investigated the drilling performance of various design of the drill and found 118° point angle is best suited for surgical drilling. Thrust force generated varies parabolically with the point angle and reaches the minimum value at approximately 118°.74 Fuchsberger71 in his investigations recommended an optimum point angle of 70° to reduce the temperature produced in bone drilling process. Hillery and Shuaib24 found no significant difference in the temperatures generated while drilling bovine tibia and cadaveric bone with drills of point angles 70°, 80°or 90° with 23° positive rake angle. Later, Augustin et al22 carried out the drilling experiments on porcine femora to evaluate the influence of the drill point angle (80°, 100° and 120°) on the temperatures generated during bone drilling. They concluded that using different drill point angles don't have any significant difference on the increase in the temperature during drilling. Karmani and Lam44 suggested a range of 110°–118° point angle for the design of orthopaedic drill.
-
2)
Chisel edge: is defined as the edge at the end of the web that connects the cutting lips (Fig. 11). The chisel edge length is equal to the web thickness and it also determines the difference between the cutting edges about the axis of rotation. The chisel edge significantly contributes to the thrust force produced during drilling. It also hampers the centering of drill bit on an irregularly curved bone surface. The amount of contribution made by the chisel edge to the axial thrust produced during drilling depends upon the ratio of lengths of chisel and the cutting edges.68 Stephenson and Agapiou74 suggested that the relationship of contribution of the chisel edge to the thrust force with respect to ratio of the web thickness to the drill diameter. They reported that at the ratio of 20%, the contribution is 50%, for a ratio of 30% the contribution doubles and for 40% it becomes four times. The straight chisel line edge has a large negative rake angle which does not have any cutting action but some sort of extrusion effect, giving rise to a considerable amount of thrust force during drilling.60 Saha et al,60 to design an improved orthopaedic drill suggested that the width of the chisel edge can be reduced by grinding to improve the cutting efficiency. However the maximum amount of web thinning is limited by minimum strength of the web necessary to avoid the breakage of the drill due to the cutting force. Natali et al32 suggested that incorporating a split point in the drill can reduce the chisel edge to almost a tip hence the extrusion effect of the chisel edge is transformed to the cutting action by imparting positive rake angle at the chisel edge zone. They also reported that this design facilitates the breaking of the chips into smaller pieces causing their easy ejection through the flutes. This modification of the drill also helped to have more acute tip which can be accurately positioned on the curved surface of the bone during drilling. From the study of the previous investigations it is clear that the reduction of the chisel edge can contribute significantly towards the lowering of the thrust forces during bone drilling with an increased accuracy in the position of the intended hole.
3.2.5. Drill wear
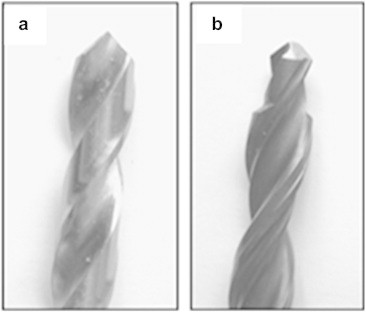
Drill wear is common during drilling. The repeated use of drill causes the cutting edges to wear out due to mechanical and thermal load encountered by them during drilling. Matthews and Hirsch21 suggested that during the bone drilling, bone temperature increases with the multiple use of drill. The wear increases the surface roughness of cutting lips resulting in the increase of axial thrust force, temperature and cutting vibrations. Drill wear can be detected by using scanning electron microscopy (SEM) or by light microscope. Jochum and Reichart75 investigated using 20 Timedur cannon drills (ZL-Duraplant-Implant-4System) for 51 times in vitro experimental setting using pig's mandibles. They concluded from the investigations that the use of drill more than 40 times causes significant wear and increase in temperature. Allan et al76 investigated the effect of drill wear on the temperature rise during drilling of the porcine mandibles in vitro. They examined three types of drills bits: one was new (Leibinger 1.5 mm diameter with two flutes), one was which had drilled 600 holes, and the third drill had been in use for several months as shown in Fig. 17. They observed a significant difference in the temperatures generated by the three drills, and reported that the change in temperature was due to the amount of wear.
Fig. 17.
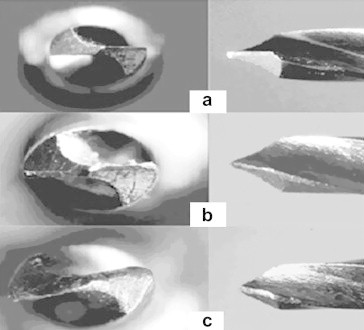
Images of the three drills end and side view. (a) The top image is of the fresh drill. (b) Worn drill (which had drilled 600 holes). (c) Worn drill (used for several months).76
Chacon et al77 measured heat generated in bone by 3 implant drill systems after repeated drilling and sterilization. Temperature was measured by them with thermocouple in vitro using the bovine femoral cortical bone specimen. Their results showed that the temperature increased with multiple uses of drill. Ercoli et al78 investigated on bovine rib and found that the TiN-coated drills showed greater wear and significantly lower material removal rates as compared to non coated drills. Misir et al79 measured increase in temperature of 4 °C and 10 °C with K type thermocouple in vitro using the bovine femoral cortical bone specimen at a constant drill load of 2.0 kg with a speed of 1500 rpm after 35 and 45 uses respectively. Karaca et al38 performed studies on the protective coatings that have been applied to the drills with the intention of improving the durability of the drill bit. They found that TiBN coated drills generates more temperatures during drilling as compared to the drills without coating. Recently Oliveira et al56 conducted drilling experiments on bovine bone with twisted stainless steel and ceramic drills to find out the relation between the thermal changes and drill wear. They found a positive correlation between temperatures generated and the no of uses of drill. They also reported that no severe deformations or blunting was detected even after 50 uses.
The above discussion of the past studies on drill wear suggests that the drill wear and temperature generated during bone drilling increases with the number of times a drill is used. No clear suggestion is made on the number by which the drill can be used repeatedly until they become blunt and ineffective, producing a significant increase in temperature.
4. Miscellaneous factors
Several other factors are present in addition to those mentioned before which affect the bone drilling process. Most of the investigations on the bone drilling had been carried out in vitro without the skeletal blood flow. Cortical flow of blood in vivo may dissipate a portion of heat developed during drilling. Wootton et al80 suggested that in the cortical bone there is a very low flow of blood, also the coagulation takes place rapidly during drilling hence its effect is likely to be too small to be important. Matthews and Hirsch21 made a comparison between the vivo and vitro studies and showed that there is no significant effect of the skeletal blood flow on the bone drilling temperature. They reported that in vivo conditions the ambient body temperature is different from vitro therefore to obtain accurate results the investigations must be preferred in actual conditions rather than in made up situations. Recently Karaca et al38 performed experiments to investigate the drilling temperature variations with bone mineral density (BMD). They found that the temperature generated during drilling increased with increasing BMD. This is because bone hardness is influenced by BMD and hardness increases with increasing BMD. Age of the patient, site of the bone in the body and its variation in properties from person to person is also an influencing parameter on the forces and the temperature generated during bone drilling. These factors can be correlated with the bone mineral density. The overshoot of the drill after the drilling of cortical bone can also be a significant factor affecting the damage of the surrounding cells and the recovery time for patient.
5. Heat generation and temperature measurement
In orthopaedics and dental practices use of drilling process for producing holes is common. The heat is produced during bone drilling due to the plastic deformation of the chips and the friction between the bone and the drill. As bone is having poor thermal conductivity, heat could not be dissipated easily, raising its temperature. This heat is a significant problem because bone is very sensitive to increase in temperature which can cause its thermal necrosis. The complex relationships between the geometry of the drill bit, drilling conditions, mechanism of the chip removal and the properties of the bone presents a great challenge in developing a mathematical model for the calculation of the heat generated during bone drilling. In the past only a few attempts for the development of a thermal model for bone drilling had been made. Although the cutting action in drilling is more complicated than in machining but mostly theory of orthogonal cutting is applied for the calculation of the heat generated during bone drilling because the chips produced during bone drilling indicates shear failure similar to the chip separated from metal during machining.40 Heat generated during drilling mainly arises from three sources (shown in Fig. 18): (A) primary shear deformation within the shear zone, (B) friction between the rake face of the tool and the chip and (C) friction between the flank face of the tool and the newly created surface of the workpiece.
Fig. 18.
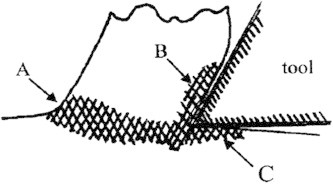
Zones of heating in orthogonal cutting.72
Davidson and James72 developed an analytical model for the calculation of rate of heat entering the bone using theory of orthogonal machining. In the development of the model for calculating the heat generated they considered only the energy used for shearing of material (Zone A) neglecting the significant effects of moving chips (Zone B), the heat produced between the tool flank and bone (Zone C) and the heat transfer between the drill bit and bone. The temperature distribution calculations were done by solving the Fourier heat conduction equation in two dimensional domain using Galerkin's Finite Element Method with Crank–Nicolson time stepping. Kalidindi48 derived and solved analytically homogeneous differential equation for the heat conduction in radial direction. Tu et al37 presented an elastic–plastic dynamic finite element model to simulate the temperature rise during drilling using commercially available finite element software Abaqus. Recently Lee et al61 suggested a new thermal model based on the theory of oblique cutting for applications into orthopaedic surgery. All the process parameters are taken as a function of the cutting radius. They considered the cutting lips to be divided into finite number of cutting elements, each of which experiences oblique cutting mechanics. The temperatures were calculated by using an explicit finite difference method.
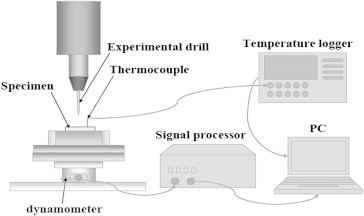
Measurement of the temperature produced during bone drilling at the tool–bone interface is egregiously difficult due to the dilemma associated with the placement of the temperature measurement device at this location. Traditionally thermocouple technique has been commonly used for the determination of the temperature elevation in both vivo and in vitro experiments (shown in Fig. 19a). But recently, use of thermographic camera has increased for the determination of the bone temperature during drilling due to its ease in measuring the temperature at any desired location (Fig. 19b).
Fig. 19.
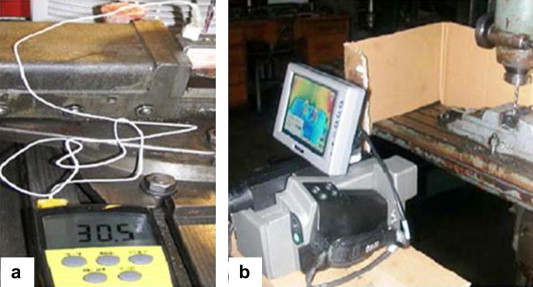
Common methods for the estimation of temperature experimentally during bone drilling: (a) thermocouple technique17 and (b) infrared (IR) thermography.80
During investigations researchers have usually used two or more thermocouples due to bone anisotropy. The review of the related literatures suggests that the thermocouples are normally placed at increasing radial distances of 0.5 mm, 1 mm and 3 mm from the drilling site. Sharawy et al27 used four thermocouple technique by using thermocouples in four orientations from the hole at the same depth. Kalidindi48 used both the techniques, where the thermographic image was utilized as a template for the placement of the thermocouple. Recently Goran et al81 investigated the temperature distributions during drilling of the porcine femora with infrared thermographic camera. The thermographic picture showed that the temperature is maximum along cortical bone, which is the most compact component of the bone. Both the methods are accompanied by certain disadvantages. These are:
-
•
Temperature measurement by thermocouple is not a satisfactory method because of poor thermal conductivity and inconsistent properties of bone.
-
•
Large number of pilot holes is to be prepared for thermocouple insertion during experiments.
-
•
Infrared thermographic camera only detects the surface temperature so it cannot accurately predict the temperature at the actual drilling site.
6. Conclusions and future directions
Almost every aspect of the bone drilling has been covered in the present review. Due to the large variations in the results obtained from bone drilling researches it is difficult to conclude briefly. The important points have been highlighted under different headings. From the above review the following points can be concluded:
-
1.
Irreversible death of the bone cells (necrosis) takes place if the temperature increases above 47° for 1 min.
-
2.
No clear indication about the optimum bone drilling speed and axial force but majority of the experimental investigations recommends high speed with larger force (of the magnitude so that the bursting of bones doesn't take place) for minimum temperature generation.
-
3.
Irrigation is the most important factor to avoid bone necrosis but no clear recommendation on better and convenient of the internal or external irrigation is reported.
-
4.
Two phase drill bit (step drill bit) is recommended over the conventional drill bits as material removal from drilling site takes place gradually which lowers the temperatures generated during drilling.
-
5.
For efficient removal of the debris and to minimize friction during bone drilling use of quick helix or worm spiral with split point and large point angle (100°–120°) is suggested.
Based on the above literature review, the guidelines for bone drilling are shown in Table 3 to highlight some common points that an orthopaedic surgeon should keep in mind to perform bone drilling with minimum drilling induced bone tissue injury.
Table 3.
Guidelines for bone drilling with minimum bone tissue injury.
| Guideline for bone drilling | Literature review recommendation | Reason |
|---|---|---|
| High drill speed with larger force (of the order so that the bursting of the bone should not take place) | No clear indication from the past studies but majority of the studies recommends high drill speed with larger force for minimum heat generation | Increase in speed and force increases the rate of heat generation but reduces the time of drilling. Hence overall less total heat is generated |
| Supply of coolant | Coolant should be used whenever it is feasible | Coolant helps in dissipating the heat through conduction. Besides taking away the heat by conduction, the coolant also provides lubrication and irrigation (excluding closed loop internal cooling system). Lubrication reduces the friction during drilling and hence less heat is generated. Irrigation causes the effective removal of chips and debris which avoids clogging of flutes during bone drilling and facilitates less heat generation |
| High drill rake angle | Rake angle of 20°–30° is recommended | Higher the rake angle, lower are the cutting forces which increases its cutting efficiency and reduces the heat generation |
| Use of split point | Can be used effectively for bone drilling as the friction between the flank and the bone is reduced by increasing the clearance angle half way along the surface | Split point causes reduction of the friction of the flank with workpiece so less heat is generated |
| Quick helix or worm spiral | Temperature decreases uniformly with increasing helix angle. The recommended ranges are 25°–35° or drill bit with parabolic flutes can be used | High helix/parabolic flutes provides an excellent clearance of debris which reduces the friction and hence reduces the heat generated |
| Two phase drill bit (step drill bit) | Step drilling is highly effective method of minimizing temperature elevation | Material removal from drilling site takes place gradually which lowers the temperatures generated during drilling |
| Large point angle | Point angle in the range of 100°–130° is recommended by most of the researches | Larger point angles provide full contact of the cutting lip with the bone as soon as drilling starts and hence less total heat is produced due to the faster cutting action |
Review suggests that the further improvement in bone drilling is possible. Continuous efforts are being made for the improvement of drill design and for optimizing the drilling parameters. There are several significant factors influencing the bone drilling on which no general agreement is yet been made, or are not investigated and need an evaluation in the future. Better understanding of these factors will enhance the performance of the surgeon and the post-operative outcome for the patient. Future work in this area includes:
-
•
Development of the model predicting the relationship of drilling force, drill temperature and surface roughness of hole with drill geometry and drilling parameters, and the effect of their variation on the force, temperature generated and surface roughness of hole produced during drilling.
-
•
Examination of the effects of internal and external cooling during bone drill and predicting more advantageous and feasible of the two.
-
•
Investigation of the effects of drill coatings on the temperature and forces produced during bone drilling. A coating which reduces the friction and is resistant to corrosion can prove to be effective for decreasing the heat generated during orthopaedic drilling.
-
•
Use of drill guides increases the friction during bone drilling and acts as a barrier preventing the contact of the coolant with the drill thus resulting in the generation of higher temperature. An investigation on the use of drill guide can provide a clear picture of its effect during orthopaedic drilling.
-
•
Non-conventional methods of drilling can be used against the conventional bone drilling and the better method can be suggested. Ultrasonically assisted bone drilling performed by Alam et al82 showed a better surface finish of the hole produced by ultrasonic method than the conventional drilling. Eshet et al83 demonstrated the use of microwave drilling of the bone for the insertion of pins, nails, screws into bone for orthopaedic and dentistry applications. Microwave drilling of bone did not degrade the mechanical properties more than the rotary drill in vitro, also smoother holes are produced than the conventional drilling with no partial bone fragments. All the above researches gives an indication that the further investigations to use these techniques for bone drilling can be beneficial.
-
•
The studies on delamination in bone have not been reported so far. An investigation of delamination can contribute significantly for minimizing bone tissue injury during drilling.
-
•
Micro drilling of the bone can be an area which can contribute significantly to improve the processes of orthopaedic fracture treatment. Forces and the temperature generated with varying drilling conditions and drill parameters can be observed during micro drilling of cortical and cancellous bone.
-
•
Automated drilling systems can be developed to minimize human error during bone drilling. The accuracy of the hole drilled during orthopaedic fracture treatment greatly depends upon the surgeons' manual skills. Currently, bone drilling tools used in surgery do not include any means for the control of penetration. Hsu et al84 proposed a mechatronic system to avoid excessive protrusion of the drill bit using a fuzzy logic controller which analyzed the current consumed by the DC motor. The experiments on the human skull showed that in none of the cases the overshoot was above 2 mm. The use of robotics and navigation system with automated provision for cooling can prove to be very effective to control the accuracy of drilled hole and the temperature generated during drilling.
Conflicts of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1.Udiljak T., Ciglar D., Skoric S. Investigation into bone drilling and thermal bone necrosis. Adv Prod Eng Manag. 2007;2:103–112. [Google Scholar]
- 2.Ueda T., Wada A., Hasegawa K. Design optimization of surgical drills using the Taguchi method. J Biomech Sci Eng. 2010;5(5) [Google Scholar]
- 3.Eriksson R.A., Albrektsson T., Magnusson B. Assessment of bone viability after heat trauma. A histological, histochemical and vital microscopic study in the rabbit. Scand J Plast Reconstr Surg. 1984;18:261–268. doi: 10.3109/02844318409052849. [DOI] [PubMed] [Google Scholar]
- 4.Moritz A.R., Henriques F.C. Studies of thermal injury: II. The relative importance of time and surface temperature in the causation of cutaneous burns. Am J Pathol. 1947;23:695–720. [PMC free article] [PubMed] [Google Scholar]
- 5.Lundskog J. Heat and bone tissue. Scand J Plast Reconstr Surg Suppl. 1972;9:1–80. [PubMed] [Google Scholar]
- 6.Pallan F.G. Histological change in bone after insertion of skeletal fixation pins. J Oral Surg Anest Hosp Dent Serv. 1960;18:400–408. [PubMed] [Google Scholar]
- 7.Augustin G., Zigman T., Davila S. Cortical bone drilling and thermal osteonecrosis. J Clin Biomech. 2012;27(4):313–325. doi: 10.1016/j.clinbiomech.2011.10.010. [DOI] [PubMed] [Google Scholar]
- 8.Noble B. Bone microdamage and cell apoptosis. Eur Cell Mater. 2003;6:46–56. doi: 10.22203/ecm.v006a05. [DOI] [PubMed] [Google Scholar]
- 9.Baron R., Horne W.C. Bone resorption. In: Bronner F., Farach-Carson M.C., Rubin J., editors. Topics in Bone Biology. Springer; London: 2005. [Google Scholar]
- 10.Franssen Bas B.G.M., Van Diest Paul J., Schuurman Arnold H., Kon Moshe. Drilling K-wires, what about the osteocytes? An experimental study in rabbits. Arch Orthop Trauma Surg. 2008;128(1):83–87. doi: 10.1007/s00402-007-0382-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eriksson R.A., Albrektsson T. Temperature threshold levels for heat-induced bone tissue injury: a vital-microscopic study in the rabbit. J Prosthet Dent. 1983;50:101–107. doi: 10.1016/0022-3913(83)90174-9. [DOI] [PubMed] [Google Scholar]
- 12.Bonfield W., Li C.H. The temperature dependence of the deformation of bone. J Biomech. 1968;7(2):323–329. doi: 10.1016/0021-9290(68)90026-2. [DOI] [PubMed] [Google Scholar]
- 13.Berman A.T., Reid J.S., Yanicko D.R., Sih G.C., Zimmerman M.R. Thermally induced bone necrosis in rabbits: relation to implant failure in humans. Clin Orthop. 1984;186:284–292. [PubMed] [Google Scholar]
- 14.Eriksson R.A., Albrektsson T. The effect of heat on bone regeneration: an experimental study in the rabbit using bone growth chamber. J Oral Maxillofac Surg. 1984;42:705–711. doi: 10.1016/0278-2391(84)90417-8. [DOI] [PubMed] [Google Scholar]
- 15.Martin R.B., Burr D.B. Raven Press; New York: 1989. Structure, Function and Adaptation of Compact Bone. [Google Scholar]
- 16.Eriksson A.R., Albrektsson T., Albrektsson B. Heat caused by drilling cortical bone. Temperature measured in vivo in patients and animals. Acta Orthop Scand. 1984;55(6):629–631. doi: 10.3109/17453678408992410. [DOI] [PubMed] [Google Scholar]
- 17.Eriksson R.A., Albrektsson T., Grane B., Mcqueen D. Thermal-injury to bone – a vital-microscopic description of heat-effects. Int J Oral Surg. 1982;11(2):115–121. doi: 10.1016/s0300-9785(82)80020-3. [DOI] [PubMed] [Google Scholar]
- 18.Eriksson R.A., Adell R. Temperatures during drilling for the placement of implants using the osseointegration technique. J Oral Maxillofac Surg. 1986;44:4–7. doi: 10.1016/0278-2391(86)90006-6. [DOI] [PubMed] [Google Scholar]
- 19.Thompson H.C. Effect of drilling into bone. J Oral Surg. 1958;16:22–30. [PubMed] [Google Scholar]
- 20.Vaughan R.C., Peyton F.A. The influence of rotational speed on temperature rise during cavity preparation. J Dent Res. 1951;30(5):737–744. doi: 10.1177/00220345510300051801. [DOI] [PubMed] [Google Scholar]
- 21.Matthews Larry S., Hirsch C. Temperatures measured in human cortical bone when drilling. J Bone Joint Surg Am. 1972;54:297–308. [PubMed] [Google Scholar]
- 22.Augustin G., Davila S., Mihoci K., Udiljak T., Vedrina D.S., Antabak A. Thermal osteonecrosis and bone drilling parameters revisited. Arch Orthop Trauma Surg. 2008;128:71–77. doi: 10.1007/s00402-007-0427-3. [DOI] [PubMed] [Google Scholar]
- 23.Brisman D.L. The effect of speed, pressure, and time on bone temperature during the drilling of implant sites. Int J Oral Maxillofac Implants. 1996;11:35–37. [PubMed] [Google Scholar]
- 24.Hillery H.T., Shuaib I. Temperature effects in drilling of human and bovine bone. J Mater Process Technol. 1999;92–93:302–308. [Google Scholar]
- 25.Bachus K.N., Rondina M.T., Hutchinson D.T. The effects of drilling force on cortical temperatures and their duration: an in vitro study. Med Eng Phys. 2000;22:685–691. doi: 10.1016/s1350-4533(01)00016-9. [DOI] [PubMed] [Google Scholar]
- 26.Nam O.H., Yu W.J., Choi M.Y., Kyung H.M. Monitoring of bone temperature during osseous preparation for orthodontic micro-screw implants: effect of motor speed and pressure. Key Eng Mater. 2006;321–323:1044–1047. [Google Scholar]
- 27.Sharawy M., Misch C.E., Weller N., Tehemar S. Heat generation during implant drilling: the significance of the motor speed. J Oral Maxillofac Surg. 2002;60:1160–1169. doi: 10.1053/joms.2002.34992. [DOI] [PubMed] [Google Scholar]
- 28.Boyne P.J. Histologic response of bone to sectioning by high-speed rotary instruments. J Dent Res. 1964;45:270–276. doi: 10.1177/00220345660450020901. [DOI] [PubMed] [Google Scholar]
- 29.Moss R.W. Histopathologic reaction of bone to surgical cutting. Oral Surg Oral Med Oral Pathol. 1964;17:405–414. doi: 10.1016/0030-4220(64)90515-8. [DOI] [PubMed] [Google Scholar]
- 30.Spartz S. Early reaction in bone following the use of burs rotating at conventional and ultra speeds. Oral Surg Oral Med Oral Pathol. 1965;19:808–816. doi: 10.1016/0030-4220(65)90353-1. [DOI] [PubMed] [Google Scholar]
- 31.Abouzgia M.B., James D.F. Temperature rise during drilling through bone. Int J Oral Maxillofac Implants. 1997;12(3):342–353. [PubMed] [Google Scholar]
- 32.Natali C., Ingle P., Dowell J. Orthopaedic bone drills – can they be improved. J Bone Joint Surg Br. 1996;78-B:357–362. [PubMed] [Google Scholar]
- 33.Iyer S., Weiss C., Mehta A. Effect of drill speed on heat production and the rate and quality of bone formation in dental implant osteotomies. Part I: relationship between drill speed and heat production. Int J Prosthodont. 1997;10(5):411–414. [PubMed] [Google Scholar]
- 34.Iyer S., Weiss C., Mehta A. Effect of drill speed on heat production and the rate and quality of bone formation in dental implant osteotomies. Part II: relationship between drill speed and healing. Int J Prosthodont. 1997;10(6):536–540. [PubMed] [Google Scholar]
- 35.Reingewirtz Y., Szmukler-Moncler S., Senger B. Influence of different parameters on bone heating and drilling time in implantology. Clin Oral Implants Res. 1997;8:189–197. doi: 10.1034/j.1600-0501.1997.080305.x. [DOI] [PubMed] [Google Scholar]
- 36.Tu Yuan-Kun, Hong You-Yao, Chen Yung-Chuan. Finite element modeling of Kirschner pin and bone thermal contact during drilling. Life Sci J. 2009;6(4) [Google Scholar]
- 37.Tu Yuan-Kun, Chen Li-Wen, Chiang Chun-Hui, Chen Yung-Chuan, Lu Wei-Hua, Tsai Hsun-Heng. 2010. Thermal Contact Simulation of the Drill Bit and Bone During Drilling. 978-1-4244-4713-8/10.IEEE. [Google Scholar]
- 38.Karaca F., Aksakal B., Kom M. Influence of orthopaedic drilling parameters on temperature and histopathology of bovine tibia: an in vitro study. Med Eng Phys. 2011 doi: 10.1016/j.medengphy.2011.05.013. [DOI] [PubMed] [Google Scholar]
- 39.Lee J., Ozdoganlar O.B., Rabin Y. An experimental investigation on thermal exposure during bone drilling. Med Eng Phys. 2012 doi: 10.1016/j.medengphy.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 40.Jacob C.H., Berry J.T. A study of the bone machining process – drilling. J Biomech. 1976;9:343–349. [PubMed] [Google Scholar]
- 41.Abouzgia M.B., James D.F. Measurement of shaft speed while drilling through bone. Int J Oral Maxillofac Implants. 1995;53:1308–1315. doi: 10.1016/0278-2391(95)90590-1. [DOI] [PubMed] [Google Scholar]
- 42.Merchant M.E. Mechanics of metal cutting process. J Appl Phys. 1945;16:267–324. [Google Scholar]
- 43.Wiggins K.L., Malkin S. Drilling of bone. J Biomech. 1976;9:553–559. doi: 10.1016/0021-9290(76)90095-6. [DOI] [PubMed] [Google Scholar]
- 44.Karmani S., Lam F. The design and function of surgical drills and K-wires. Curr Orthop. 2004;18:484–490. [Google Scholar]
- 45.Lavelle C., Wedgwood D. Effect of internal irrigation on frictional heat generated from bone drilling. J Oral Surg. 1980;38:499–503. [PubMed] [Google Scholar]
- 46.Haider R., Watzek G., Plenk H. Effect of drill cooling and bone structure on IMZ implant fixation. Int J Oral Maxillofac Implants. 1993;8:83–91. [PubMed] [Google Scholar]
- 47.Benington I.C., Biagioni P.A., Briggs J., Shearidan S., Lamey P.J. Thermal changes observed at implant sites during internal and external irrigation. Clin Oral Implants Res. 2002;13(3):293–297. doi: 10.1034/j.1600-0501.2002.130309.x. [DOI] [PubMed] [Google Scholar]
- 48.Kalidindi V. Optimization of Drill Design and Coolant Systems During Dental Implant Surgery. MS thesis, University of Kentucky; 2004.
- 49.Bagci E., Ozcelik B. Effects of different cooling conditions on twist drill temperature. Int J Adv Manuf Technol. 2007;34:867–877. [Google Scholar]
- 50.Kirschner H., Meyer W. Entwichlung einer innenkuhlung fur chirurgische bohrer. Dtsch Zahnaztl Zeitschrift. 1975;30:436–438. [PubMed] [Google Scholar]
- 51.Sener B.C., Dergin G., Gursoy B., Kelesoglu E., Slih I. Effects of irrigation temperature on heat control in vitro at different drilling depths. Clin Oral Implants Res. 2009;20:294–298. doi: 10.1111/j.1600-0501.2008.01643.x. [DOI] [PubMed] [Google Scholar]
- 52.Al-Dabag A.N., Sultan Ahmed A. Effect of cooling an irrigation solution during preparation of implant site on heat generation using Elite system for implant. Al-Rafidain Dent J. 2010;10(2):260–264. (Experimental Study) [Google Scholar]
- 53.Augustin G., Davila S., Udilljak T., Staroveski T., Brezak D., Babic S. Temperature changes during cortical bone drilling with a newly designed step drill and internally cooled drill. Int Orthop. 2012 doi: 10.1007/s00264-012-1491-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Cardioli G., Majzoub Z. Heat generation during implant site preparation: an in vitro study. J Oral Maxillofac Implants. 1997;12:186–193. [PubMed] [Google Scholar]
- 55.Tehemer S.H. Factors affecting heat generation during implant site preparations: a review of biologic observations and future considerations. Int J Oral Maxillofac Implants. 1999;14:127–136. [PubMed] [Google Scholar]
- 56.Oliveira N., Alaejos-Algarra F., Mareque-Bueno J., Ferrés-Padró E., Hernández-Alfaro F. Thermal changes and drill wear in bovine bone during implant site preparation. A comparative in vitro study: twisted stainless steel and ceramic drills. Clin Oral Implants Res. 2011 doi: 10.1111/j.1600-0501.2011.02248.x. [DOI] [PubMed] [Google Scholar]
- 57.Matthews L.S., Green C.A., Goldstein S.A. The thermal effects of skeletal fixation-pin insertion in bone. J Bone Joint Surg Am. 1984;66:1077–1083. [PubMed] [Google Scholar]
- 58.Branemark P.I. Osseointegration and its experimental background. J Prosthet Dent. 1983;50:399–410. doi: 10.1016/s0022-3913(83)80101-2. [DOI] [PubMed] [Google Scholar]
- 59.Itay S., Tsur H. Thermal osteonecrosis complicating Steinmann pin insertion in plastic surgery. Plast Reconstr Surg. 1983;72:557–561. doi: 10.1097/00006534-198310000-00029. [DOI] [PubMed] [Google Scholar]
- 60.Saha S., Pal S., Albright J.A. Surgical drilling: design and performance of an improved drill. J Biomech Eng. 1982;104:245–252. doi: 10.1115/1.3138356. [DOI] [PubMed] [Google Scholar]
- 61.Lee J., Rabin Y., Ozdoganlar O.B. A new thermal model for bone drilling with application to orthopaedic surgery. Med Eng Phys. 2011 doi: 10.1016/j.medengphy.2011.05.014. [DOI] [PubMed] [Google Scholar]
- 62.Bechtol C.O., Ferguson A.B., Laing P.G. Williams and Wilkins; Baltimore: 1959. Metals and Engineering in Bone and Joint Surgery. [Google Scholar]
- 63.Burstein A., Currey J., Frankel V., Heiple K., Lunseth P., Vessely J. Bone strength, the effect of screw holes. J Bone Joint Surg Am. 1972;54A:1143–1156. [PubMed] [Google Scholar]
- 64.Hufner T., Geerling J., Oldag G., Richter M., Kfuri M., Pohlemann T. Accuracy study of computer-assisted drilling: the effect of bone density, drill bit characteristics and use of a mechanical guide. J Orthop Trauma. 2005;19:317–322. [PubMed] [Google Scholar]
- 65.Jacob C.H., Berry J.T., Pope M.H., Hoaglund F.T. A study of the bone machining process – orthogonal cutting. J Biomech. 1974;7:131–136. doi: 10.1016/0021-9290(74)90051-7. [DOI] [PubMed] [Google Scholar]
- 66.Farnworth G.H., Burton J.A. Int Mach Tool Des and Res Conf 15th Proc. 1974. Optimization of drill geometry for orthopaedic surgery; pp. 227–233. [Google Scholar]
- 67.Bertollo N., Gothelf T.K., Walsh W.R. 3-Fluted orthopaedic drills exhibit superior bending stiffness to their two fluted rivals: clinical implications for targeting ability and the incidence of drill bit failure. Injury. 2008;39:734–741. doi: 10.1016/j.injury.2007.11.286. [DOI] [PubMed] [Google Scholar]
- 68.Bertollo N., Walsh W.R. Drilling of bone: practicality, limitations and complications associated with surgical drill bits. Biomech Appl. 2011 [Google Scholar]
- 69.Bertollo N., Milne H.R.M., Ellis L.P., Stephens P.C., Gillies R.M., Walsh W.R. A comparison of thermal properties of 2- and 3- fluted drills and the effect on bone cell viability and screw pull out strength in an ovine model. Clin Biomech. 2010;25:613–617. doi: 10.1016/j.clinbiomech.2010.02.007. [DOI] [PubMed] [Google Scholar]
- 70.Narashimha K., Osman M.O.M., Chandrasekhar S., Frazao J. An investigation into the influence of helix angle on the torque-thrust coupling effect in twist drills. Int J Adv Manuf Technol. 1987;2(4):91–105. [Google Scholar]
- 71.Fuchsberger A. The damaging temperature at the machining of the bone. Unfallchirurgie. 1988;14(4):173–183. [PubMed] [Google Scholar]
- 72.Davidson S.R.H., James D.F. Measurement of thermal conductivity of bovine cortical bone. Med Eng Phys. 2000;22:741–747. doi: 10.1016/s1350-4533(01)00003-0. [DOI] [PubMed] [Google Scholar]
- 73.Sneath R.S. Proceedings of the Symposium of Glasgow. Peragamon Press; Oxford: 1964. The determination of optimum twist drill shape for bone. Biomechanics and related bioengineering topics. [Google Scholar]
- 74.Stephenson D.A., Agapiou J.S. 1997. Metal Cutting Theory and Practice. [Google Scholar]
- 75.Jochum R.M., Reichart P.A. Influence of multiple use of Timedur-titanium cannon drills: thermal response and scanning electron microscopic findings. Clin Oral Implants Res. 2000;11(2):139–143. [PubMed] [Google Scholar]
- 76.Allan W., Williams E.D., Kerawala C.J. Effects of repeated drill use on temperature of bone during preparation for osteosynthesis self-tapping screws. Br J Oral Maxillofac Surg. 2005;43(4):314–319. doi: 10.1016/j.bjoms.2004.11.007. [DOI] [PubMed] [Google Scholar]
- 77.Chacon G.E., Bower D.L., Larsen P.E., McGlumphy E.A., Beck F.M. Heat production by 3 implant drill systems after repeated drilling and sterilization. J Oral Maxillofac Surg. 2006;64(2):265–269. doi: 10.1016/j.joms.2005.10.011. [DOI] [PubMed] [Google Scholar]
- 78.Ercoli C., Funkenbusch P.D., Lee H.J., Moss M.E., Graser G.N. The influence of drill wear on cutting efficiency and heat production during osteotomy preparation for dental implants: a study of drill durability. Int J Oral Maxillofac Implants. 2004;19(3):335–349. [PubMed] [Google Scholar]
- 79.Misir A.F., Sumer M., Yenisey M., Ergioglu E. Effect of surgical drill guide on heat generated from implant drilling. J Oral Maxillofac Surg. 2009;67(12):2663–2668. doi: 10.1016/j.joms.2009.07.056. [DOI] [PubMed] [Google Scholar]
- 80.Wootton R., Reeve J., Veall N. The clinical measurement of skeletal blood flow. Clin Sci Mol Med. 1976;50:261–268. doi: 10.1042/cs0500261. [DOI] [PubMed] [Google Scholar]
- 81.Augustin G., Davila S., Udiljak T., Vedrina D.S., Bagatin D. Determination of spatial distribution of increase in bone temperature during drilling by infrared thermography: preliminary report. Arch Orthop Trauma Surg. 2009;129(5):703–709. doi: 10.1007/s00402-008-0630-x. [DOI] [PubMed] [Google Scholar]
- 82.Alam K., Mitrofanov A.V., Silberschmidt V.V. Measurement of surface roughness in conventional and ultrasonically assisted bone drilling. Am J Biomed Sci. 2009;1:312–320. [Google Scholar]
- 83.Eshet Y., Mann R.R., Anaton A., Yacoby T., Gefen A., Jerby E. Microwave drilling of bones. IEEE Trans Biomed Eng. 2006;53(6) doi: 10.1109/TBME.2006.873562. [DOI] [PubMed] [Google Scholar]
- 84.Hsu Y.L., Lee S.T., Lin H.W. A modular mechatronic system for automatic bone drilling. Biomed Eng Appl Basis Commun. 2001;13:168–174. [Google Scholar]