

Abstract
An 18 year old male patient was hit by a car to his motorcycle causing a unicondylar Hoffa fracture and an ipsilateral patella fracture. Hoffa fracture is a rare lesion and this association of injury has not been reported before.
Keywords: Hoffa, Unicondylar, Femoral, Coronal fracture, Patella
1. Introduction
Isolated coronal plane fractures of the femoral condyles (Hoffa fracture) are unusual high velocity injuries. The injury may be missed on routine radiography in the undisplaced fracture. Open reduction, internal fixation and early mobilization are essential for good long-term results. Hoffa fracture can exceptionally occur with ipsilateral vertical patella fracture. We report a case of this rare association.
2. Case report
An 18 years old male was admitted to the emergency department after being involved in a car accident. He was hit by a car to his motorcycle. The impact was frontal, on his left knee. He reported a severe pain, a swelling in his left knee, and functional impotency in his left inferior limb. Local examination showed a significant swelling of the left knee. No open wounds were noted in that region. Standard radiographs in anterior-posterior (AP) incidence were performed after admittance; the X-rays revealed a displaced Hoffa fracture (coronal unicondylar medial femoral fracture) and vertical patella fracture (Fig. 1). This injury was not associated with peripheral nerve damage nor with vascular lesions and no other fractures were noted. In order to better assess the extent of the damage and to better plan the treatment, a computer tomography (CT) to the left knee was performed. CT examination, confirmed the diagnosis and the important displacement of the fracture (Fig. 2). Using a medial approach, and after reduction the fragments temporarily fixed with Kirschner wires, we fixed the Hoffa fracture with two 6.5 cannulated screws. Fluoroscopy was used to ensure there was no violation of the distal femoral physis and to verified reduction and screw position. We also reduced and stabilized the vertical patella fracture by tension band wiring (Fig. 3). We applied a cylindrical cast and allowed the patient to walk with crutches, non-weight bearing. Physical rehabilitation program was started after surgery to allow the patient to regain full range of movement. At follow-up 6 weeks postoperatively, the fracture was radiographically healed and the patient had no complaints or sensation of snapping. Full weight-bearing was allowed progressively after 8 weeks. At the last follow-up visit 20 months after the operation, the patient was pain free and able to achieve a normal range of movement, with 150° flexion of the knee and full extension (Fig. 4). Radiographs revealed a consolidated fracture (Fig. 5).
Fig. 1.
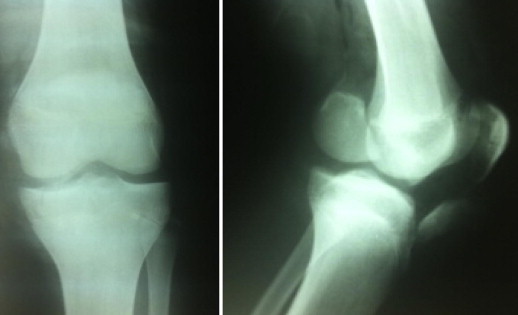
Anteroposterior and lateral radiograph of the left knee shows a displaced Hoffa fracture and fracture of the patella.
Fig. 2.
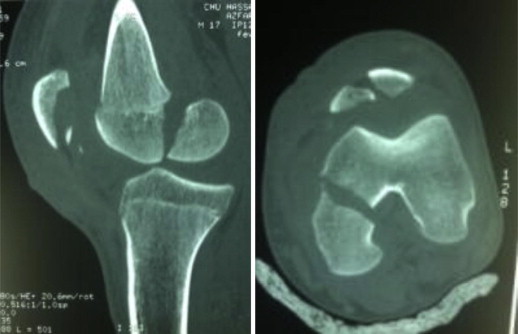
A computed tomography scan of the left knee shows coronally oriented fracture through medial femoral condyle.
Fig. 3.

Postoperative radiograph after open reduction and internal fixation of the Hoffa fracture and fracture of the patella.
Fig. 4.

Clinical photograph showing functional range of movement of the left knee.
Fig. 5.

Lateral view of the knee shows at follow-up 20 months postoperatively, the fracture was completely healed.
3. Discussion
Coronal fractures of the femoral condyle, first described by Hoffa in 1904, are an unusual injury. It is usually caused by high energy trauma.1 This type of injury is very rare and misdiagnosis is common. It can be especially in motorcycle accident.2,3 It most commonly affects the lateral femoral condyle.2 Unicondylar Hoffa fractures have been reported in isolation,2–4 or with ipsilateral femoral supracondylar and intercondylar fractures,5,6 of the femoral neck or shaft7 and patellar dislocation.8 A case of ipsilateral Hoffa fracture and patella fracture is extremely rare. To our acquaintance, such a fracture pattern has not yet been reported in the literature so far. Holmes et al3 reported that the mechanism of injury in Hoffa fracture implies a direct force resulting from the impaction of the upper part of the tibia on the femoral condyles, with the knee flexed more than 90°. In our case, the association of fracture results from a combination of forces: direct trauma causing Hoffa fracture and possibly indirect injuries from sudden contraction of the quadriceps muscle causing vertical patella fracture. Physical examinations usually reveal edema, effusion, or skin lesions in the knee region after injury.2,4 Neurovascular examination of the whole extremity should be carefully performed. The diagnosis may be missed.8 Careful radiographic evaluation, including anteroposterior, lateral, tangential patellar, and tunnel views, is necessary to accurately diagnose knee related injuries and coronal fractures of the condyle.9 A computed tomography scan is necessary to more accurately describe the fracture, as coronal fractures may be easily overlooked.3,5,10
Surgical fixation is the recommended method of treatment for a Hoffa fracture.3,5,11–13 The operative approach was lateral for unicondylar lateral Hoffa fracture8,10 and it was medial for unicondylar medial Hoffa fracture like our case. The joint was carefully inspected for associated injuries. After reduction the fragments of unicondylar fracture were temporarily fixed with Kirschner wires. A minimum of two screws is mandatory to provide rotational stability.8 Fluoroscopy was used to verify reduction and screw position. We preferred to use two 6.5 cannulated screws to permit an early postoperative range of motion of the knee with very good long-term results.8,14 In this case, the operative approach was medial. We began by reduction of the fragments of unicondylar fracture and we fixed temporally with Kirschner wires and we fixed the Hoffa fracture with two 6.5 cannulated screws. We also reduced and stabilized the vertical patella fracture by tension band wiring. We found a tear in the medial retinaculum, which was repaired in the end.
A solitary Hoffa fracture is a rare occurrence, but the fracture is not uncommon when associated with patella fracture like our case. The mechanism of injury is usually high energy, often associated with multiple injuries so can easily be overlooked. These fractures should be treated with open reduction and internal fixation to achieve anatomic reduction with stable fixation. We believe this optimizes the chance for good long-term functional results.
Conflicts of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1.Hoffa A. 4th ed. Ferdinand Enke-Verlag; Stuttgart: 1904. Lehrbuch der Frakturen und Luxationen. 453. [Google Scholar]
- 2.Kumar R., Malhotra R. The Hoffa fracture: three case reports. J Orthop Surg (Hong Kong) 2001 Dec;9(2):47–51. [Google Scholar]
- 3.Holmes S.M., Bomback D., Baumgaertner M.R. Coronal fractures of the femoral condyle: a brief report of five cases. J Orthop Trauma. 2004;18:316–319. doi: 10.1097/00005131-200405000-00010. [DOI] [PubMed] [Google Scholar]
- 4.Yücel I., Dĕgirmenci E., Özturan K. Hoffa fracture—a case report. Düzce Tıp Fakültesi Dergisi. 2008;2:37–40. [Google Scholar]
- 5.Baker B.J., Escobedo E.M., Nork S.E., Henley M.B. Hoffa fracture: a common association with high-energy supracondylar fractures of the distal femur. AJR Am J Roentgenol. 2002;178:994. doi: 10.2214/ajr.178.4.1780994. [DOI] [PubMed] [Google Scholar]
- 6.Nork S.E., Segina D.N., Aflatoon K. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005;87:564–569. doi: 10.2106/JBJS.D.01751. [DOI] [PubMed] [Google Scholar]
- 7.Miyamoto R., Fornari E., Tejwani N.C. Hoffa fragment associated with a femoral shaft fracture – a case report. J Bone Joint Surg Am. 2006;88:2270–2274. doi: 10.2106/JBJS.E.01003. [DOI] [PubMed] [Google Scholar]
- 8.Vaishya R., Singh A.P., Dar I.T., Singh A.P., Mittal V. Hoffa fracture with ipsilateral patellar dislocation resulting from household trauma. Can J Surg. 2009 Feb;52(1) [PMC free article] [PubMed] [Google Scholar]
- 9.Allman K.H., Altehoefer C., Wildanger G. Hoffa fracture – a radiologic diagnostic approach. J Belge Radiol. 1996;79:201–202. [PubMed] [Google Scholar]
- 10.Lewis S.L., Pozo J.L., Muirhead-Allwood W.F. Coronal fractures of the lateral femoral condyle. J Bone Joint Surg Br. 1989;71:118–120. doi: 10.1302/0301-620X.71B1.2914979. [DOI] [PubMed] [Google Scholar]
- 11.Papadopoulos A.X., Panagopoulos A., Karageorgos A., Tyllianakis M. Operative treatment of unilateral bicondylar Hoffa fractures. J Orthop Trauma. 2004;18:119–122. doi: 10.1097/00005131-200402000-00012. [DOI] [PubMed] [Google Scholar]
- 12.Zeebregts C.J., Zimmerman K.W., ten Duis H.J. Operative treatment of a unilateral bicondylar fracture of the femur. Acta Chir Belg. 2000;100:104–106. [PubMed] [Google Scholar]
- 13.Fang W.S., Zhang Y.C., Shi G.C. Surgical treatment of Hoffa fractures. Zhongguo Gu Shang. 2008 Jan;21(1):63. [PubMed] [Google Scholar]
- 14.Jarit G.J., Kummer F.J., Gibber M.J., Egol K.A. A mechanical evaluation of two fixation methods using cancellous screws for coronal fractures of the lateral condyle of the distal femur (OTA type 33B) J Orthop Trauma. 2006;20:273–276. doi: 10.1097/00005131-200604000-00007. [DOI] [PubMed] [Google Scholar]