

Abstract
Stress fractures of the first rib in athletes are rare. A 14-year-old male, a baseball pitcher who changed from an overhand to a sidearm style, with a stress fracture of the first rib, was reported. Most Stress fractures in the first rib occur at the subclavian groove, between the attachments of the scalenus anterior and scalenus medius muscles, which is the thinnest and weakest portion of the rib. However, in this case the stress fracture occurred at the uncommon region, posterior to the insertion of the scalenus medius muscle, in the first rib. The motion analysis of the pitching in this case demonstrated that the sidearm style induced much more horizontal abduction in the shoulder at the top position than did the overhand style. The findings of electromyography in the serratus anterior muscle, one of the muscles which insert on the first rib, through the pitching motion did not demonstrate any significant differences between the two styles. In this case, the repetition of horizontal over-abduction of the shoulder when sidearm pitching appears to have been the cause of the unusual stress fracture of the first rib at this site.
Key Points.
Most Stress fractures in the first rib occur at the subclavian groove, between the attachments of the scalenus anterior and scalenus medius muscles, which is the thinnest and weakest portion of the rib.
We report the case of a young male baseball pitcher with a stress fracture of the first rib located uncommonly at the posterior portion of the rib.
In this case, the repetition of horizontal over-abduction of the shoulder when sidearm pitching appears to have been the cause of the unusual stress fracture of the first rib at this site.
Key words: Motion analysis, horizontal abduction, electromyography, serratus anterior muscle
Introduction
Stress fractures of the first ribs in athletes are rare; in baseball pitchers this injury has been reported in pitching arm (Edwards and Murphy, 2001; Gurtler et al., 1985) and non-pitching arm sides (Curran and Kelly, 1966; Tullos et al., 1972). Most stress fractures in the first ribs occur at the subclavian artery groove between the attachments of the scalenus anterior and scalenus medius muscles, which is the thinnest and weakest portion of the rib (Brooke, 1959; Curran and Kelly, 1966; Edwards and Murphy, 2001; Gurtler et al., 1985; Lankenner and Micheli, 1985; Matsumoto et al., 2003; Mintz et al., 1990; Proffer et al., 1991; Tullos et al., 1972). The serratus anterior also attaches at this level.
We report the case of a young male baseball pitcher with a stress fracture of the first rib located uncommonly at the posterior portion of the rib. To clarify the mechanisms, we performed motion analysis and electromyography (EMG) of the serratus anterior muscle in his pitching style.
Case History
A 14-year-old male, a right-handed pitcher with a sidearm style, heard a snap in his right shoulder followed by severe pain while pitching in the first inning of a game. He had changed from an overhand to a sidearm style 6 months before the onset of severe pain. He had experienced discomfort in his pitching side shoulder for several days before the onset. Prior to the injury, he had no history of direct trauma to the shoulder girdle, and he usually practiced pitching three times per week. On physical examination, the patient had no atrophy of his chest or upper extremity muscles, either anteriorly or posteriorly. Deep breath induced pain at the right upper chest. The ranges of motion of both shoulders were normal. Tenderness was elicited with deep palpation in regions of the right anterosuperior chest and the superomedial border of the right scapula. Initial radiographs demonstrated a radiolucent line without a displacement at the posterior portion of the first rib (Figure 1). The radiolucent line of the medial portion was wider than that of the lateral portion. Magnetic resonance imaging also showed a similar clear high- intensity line, posterior to the insertion of the scalenus medius muscle, on a T2-weighted image (Figure 2).
Figure 1.

An anteroposterior radiograph shows a radiolucent line without displacement at the posterior portion of the first rib (white arrows). The radiolucent line of the medial portion is wider than that of the lateral portion.
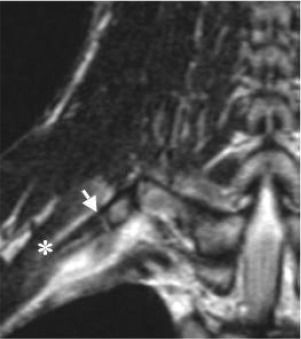
Figure 2.

T2-weighted magnetic resonance imaging shows a clear high-intensity line at the posterior portion of the first rib (white arrow), posterior to the insertion of the scalenus medius muscle (white asterisk).
The fracture site, posterior to the insertion of the scalenus medius muscle, of the first rib was considered an uncommon region for a fracture because most first rib fractures occur in the subclavian groove, the thinnest, weakest portion of the rib. We diagnosed this fracture of the first rib as a stress fracture and treated it conservatively. The patient was advised not to throw for 6 weeks but was allowed to exercise by running or through any activities that were without pain. After this period he gradually began to throw again; but he decided to change his sidearm style back to an overhand one. At 2 months post-injury, follow-up radiographs showed callus formation at the fracture site but with no displacement (Figure 3). The patient had no discomfort in his shoulder girdle during any physical activities and has completely returned to full pitching activities.
Figure 3.
An anteroposterior radiograph at 2 months post-injury shows callus formation at the fracture site but with no displacement (black arrows).
Biomechanics
To clarify the mechanism by which this uncommon first rib stress fracture occurred at the posterior portion of the rib, we performed motion analysis and the EMG of the serratus anterior muscle during pitching at 4 months post-injury. A pitching motion can be divided into five phases: windup, arm cocking, arm acceleration, arm deceleration, and follow-through (Fleisig et al., 1994). In arm cocking, the arm and trunk of the pitching side rotates back after foot contact. In this article, “top position ”is defined as the time at which the ball is held up at its highest position when the arm and trunk of the pitching side rotates back maximally after the foot contact. Six high-speed Falcon high-resolution cameras at 60 Hz (Motion Analysis Corp., Santa Rosa, California, USA) recorded the locations of reflective markers on the patient. The three-dimensional location of each marker, based on data from the cameras, was automatically digitized with the Eva RT 4.0 software (Motion Analysis Corp.). Surface electrodes (Blue Sensor, Medicotest A/S, lstykke, Denmark) with on-site preamplifiers (Myosystem 1200, Noraxon USA, Inc., Scottsdale, Arizona, USA) used to access EMG activity of the serratus anterior muscles. EMG data were recorded synchronously with the motion analysis data and analyzed using a Bio-Signal Analysis Software, BIMUTUS2 (Kissei Comtec, Nagano, Japan). Thirty reflective markers were placed on his trunk and extremities for the motion analysis, along with three pairs of electrodes on his right serratus anterior muscle (upper, middle and lower portions) for EMG data (Figure 4). In this article, the angle of horizontal abduction in the shoulder was defined as the angle between the line which connected right shoulder (marker No.1) with spinous process of C7 (marker No.29) and the line which connected right shoulder with right lateral elbow (marker No.3, Figure 5A). The angle of abduction in the shoulder was defined as the angle between the line which connected right shoulder with right hip (marker No.8) and the line which connected right shoulder with right lateral elbow (Figure 5B). In calibration process, the motion analysis system used a dynamic linearization technique. First, a small four-point calibration device is used for defining the XYZ axes. A 500mm wand (for large capture volumes) is then used for establishing camera linearization parameters. The error of measurement was by less than 0.164%. The EMG data were expressed as the integral values of voltages measured on surface electrodes during each phase in pitching. In the testing facility, pitches were thrown from a flat mound toward a target zone located 7 meters from the pitching line. The patient was given sufficient time for a warm-up (stretching and jogging), and each ten pitches of 70% and 90% efforts in his maximum effort to prepare the pitching style. He was asked to perform three full pitches either sidearm or overhand style for the motion analysis and the EMG data.
Figure 4.
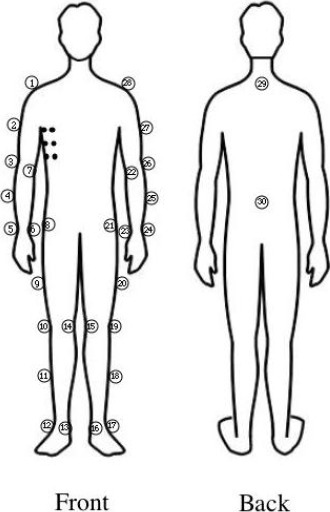
Schematic of the reflective markers and the surface electrodes. Six black circles on right chest show three pairs of the surface electrodes.
Figure 5.
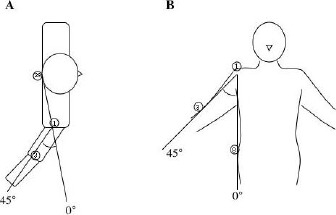
Definition of the angles of horizontal abduction and abduction in the shoulder. (A) The angle of horizontal abduction in the shoulder. (B) The angle of abduction in the shoulder.
The motion analysis of the pitching in this case demonstrated that the sidearm style induced greater horizontal abduction (121% of the overhand style; Table 1 and Figures 6A and 6B) in the shoulder at the top position. The findings from EMG in the serratus anterior muscle during pitching showed no clear differences between the sidearm and overhand styles (Table 2).
Table 1.
Angles of horizontal abduction and abduction in shoulder during pitching.
| Horizontal Abduction | Abduction | ||||||
|---|---|---|---|---|---|---|---|
| Style | No. of pitch | Top position | Ball release | Top position | Ball release | ||
| Overhand | 1 | 89.6 | -41.0 | 98.7 | 109.1 | ||
| 2 | 87.1 | -35.4 | 93.9 | 121.5 | |||
| 3 | 88.7 | -46.1 | 108.0 | 115.0 | |||
| Sidearm | 1 | 107.2 | -38.5 | 85.9 | 124.0 | ||
| 2 | 104.5 | -39.3 | 90.2 | 116.1 | |||
| 3 | 109.3 | -46.1 | 102.0 | 120.3 | |||
Table 2.
Integral values of voltages in EMG during each phase in pitching.
| Integral values of voltages (Volt) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Style | No. of pitch* | Portion of serratus anterior | Windup - arm cocking | Arm acceleration | Arm deceleration - follow-through | |||
| Overhand | 1 | upper | 117.3 | 41.9 | 361.1 | |||
| 2 | upper | 110.2 | 46.2 | 263.2 | ||||
| 1 | middle | 217.6 | 108.1 | 69.7 | ||||
| 2 | middle | 231.3 | 96.7 | 113.8 | ||||
| 1 | lower | 157.6 | 135.5 | 66.9 | ||||
| 2 | lower | 155.9 | 134.9 | 78.2 | ||||
| Sidearm | 1 | upper | 103.9 | 36.7 | 327.1 | |||
| 2 | upper | 143.6 | 31.8 | 295.0 | ||||
| 1 | middle | 138.7 | 83.7 | 136.8 | ||||
| 2 | middle | 217.0 | 95.5 | 145.6 | ||||
| 1 | lower | 103.2 | 74.7 | 63.7 | ||||
| 2 | lower | 148.0 | 98.1 | 72.1 | ||||
*Two pitches in each style were available for the EMG study.
Discussion
Previous reports have fully described the anatomical features of the first rib and the causes of stress fractures of the rib (Curran and Kelly, 1966; Gurtler et al., 1985). The first rib itself is broad and flat with the tubercle located at the junction of the anterior third with the posterior two thirds. On either side of this tubercle is a groove for the subclavian artery posteriorly and the subclavian vein anteriorly. The groove is deeper for the artery than for the vein, forming the weakest point in the first rib. The groove in the bone also lies between forces pulling up (the scalenus anterior and medius muscles) and forces pulling down (the serratus anterior and intercostals muscles). Therefore, the groove for the subclavian artery is the most common location for stress fractures; including cases involving baseball pitchers (Curran and Kelly, 1966; Edwards and Murphy, 2001; Gurtler et al., 1985; Tullos et al., 1972) and other athletes (Lankenner and Micheli, 1985; Matsumoto et al., 2003; Proffer et al., 1991).
Our case demonstrated a stress fracture of the first rib that was uncommonly located at the posterior portion of the rib posterior to the insertion of the scalenus medius muscle. To our knowledge, there are just two reports, of a spontaneous (Chan et al., 1994) and a stress (Mamanee et al., 1999) fracture at the same site, the posterior portion of the first rib. However, the mechanism for the fractures of the first rib at this location is unclear. Training errors, such as overuse or a rapid increase in training contributes to a stress fracture of the first rib (Lankenner and Micheli, 1985). The case in this study changed from an overhand to a sidearm style 6 months before the onset of severe pain. Therefore, we considered that the change of the patients pitching style might have been the cause of this stress fracture. The motion analysis of the pitching here showed that horizontal abduction in the shoulder and the rotation of the trunk to the back was maximal at the top position in both of the two pitching styles (data not shown). The first rib has a rigid attachment both to the sternum anteriorly and to the first thoracic vertebrae posteriorly. Horizontal abduction in the shoulder induces adduction of the scapula. These findings and the anatomical features suggest that horizontal abduction in the shoulder, adduction of the scapula, and the rotation of the trunk to the back cause great stress to the posterior portion of the first rib at the top position during pitching. The motion analysis data demonstrated that the sidearm style induced much more horizontal abduction in the shoulder at the top position than did the overhand style. The findings of EMG in the serratus anterior muscle through the pitching motion did not demonstrate clear differences between the two styles. It appears that in this case the repetition of over abduction horizontally in the shoulder at the top position of his sidearm pitching caused the stress fracture of the first rib at this uncommon location (Figure 7).
Figure 7.
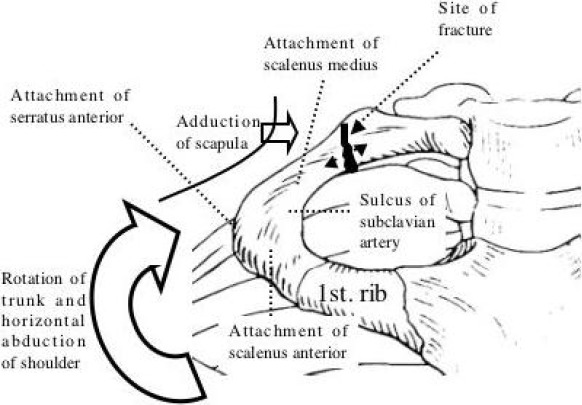
The mechanism by which this uncommonly occurring, at the posterior portion of the rib, first rib stress fracture is proposed. The first rib has a rigid attachment to both the sternum anteriorly and to the first thoracic verteblae posteriorly. Horizontal abduction in the shoulder, adduction of the scapula, and the rotation of the trunk to the back cause great stress to the posterior portion of the first rib at the top position during pitching. In this case, the repetition of over horizontal abduction in the shoulder at the top position of the patient’s sidearm pitching appears to have caused the stress fracture of the first rib at this uncommon location.
Gregory et al. well reviewed the clinical aspects of stress fractures of the first rib (Gregory et al., 2002). The onset is usually insidious, although it can often start with a pop and acute pain. There may be tenderness medial to the superior angle of the scapula, at the root of the neck, supraclavicular triangle or deep in the axilla. Shoulder movements may be painful or restricted. Plain chest radiographs are usually initially negative and diagnosis requires computed tomography or magnetic resonance imaging. The recommended treatment of a first rib stress fracture involves immobilization of the shoulder girdle on the affected side with a sling with adequate analgesia offered. Long-term follow-up, with serial radiographs for 6 months, is advised to assess late developing complications. Our case did not need any immobilization of the shoulder girdle because there was only mild motion pain in the shoulder and shoulder girdle. The critical issue for athletes is when they can return to competitive levels. Two papers have reported first rib stress fractures on the pitching side in baseball pitchers (Edwards and Murphy, 2001; Gurtler et al., 1985). A 17-year-old male, left-handed pitcher, because of delayed union, returned to full pitching at 9 months post-injury (Gurtler et al., 1985). A 15-year-old male, right-handed pitcher, returned to full pitching at 6 months post-injury with non-union of the fracture, but without any symptoms (Edwards and Murphy, 2001). The period of return to full pitching in our case (2 months post-injury) was much shorter than in previous cases. In the initial phase of training post-injury, the patient decided to change from the sidearm style back to his previous overhand one. This change to the former pitching style, avoiding over horizontal abduction in the shoulder, might have quickened the return to full pitching.
There are several limitations to this study. The number of samples (pitches) is too small to identify the significant differences between the two pitching styles. The data speed (60 Hz) of motion analysis might be insufficient to analyze the pitching motion. The analysis of motion was retrospective and the movement might not represent the pre-injury technique. Scalenus anterior and scalenus medius muscles, which are considered to mainly cause the stress fracture in the first ribs, were not studied in EMG because of technical difficulties in the EMG study with the surface electrodes.
In summary, we detailed the case of a young male baseball pitcher with a stress fracture of the first rib that was uncommonly located at the posterior portion of the rib. In this case, the repetition of horizontal over-abduction of the shoulder when sidearm pitching appears to have been the cause of the unusual stress fracture of the first rib at this site. First rib stress fractures can be considered a rare cause of shoulder or shoulder girdle pain in a baseball pitcher.
Figure 6.
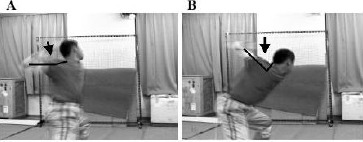
The sidearm style induces greater horizontal abduction in the shoulder at the top position than does the overhand style. (A) The overhand style at the top position. (B) The sidearm style at the top position. The black arrows and bars indicate the angle of horizontal abduction in the shoulder at the top position.
Biographies

Takeshi SAKATA
Employment
Chief in Department of Orthopedic Surgery and Sports Medicine, Kitade Hospital, Gobo, Wakayama, Japan.
Degree
MD, PhD
Research interests
Biomechanics of throwing and throwing injury, osteoporosis induced by unloading.
E-mail: sakatatakeshi@hotmail.com

Yasunobu KIMURA
Employment
Ass. researcher in Department of Sports Studies, Kitade Hospital, Gobo, Wakayama, Japan.
Degree
BSc
Research interests
Motion analysis in throwing athletes.
E-mail: soudan@tiara.ocn.ne.jp

Toshiko HIDA
Employment
Physical therapist in Department of Rehab. Medicine, Kitade Hospital, Gobo, Wakayama, Japan.
Degree
PT
Research interests
Athletic injuries and rehab-ilitation
References
- Brooke R. (1959) Jive fracture of the first rib. Journal of Bone and Joint Surgery (Br) 41-B, 370-371 [DOI] [PubMed] [Google Scholar]
- Chan M.C., Fenton P., Conlan A.A. (1994) Unusual site of spontaneous first-rib fracture: case report. Canadian Journal of Surgery 37, 425-427 [PubMed] [Google Scholar]
- Curran J.P., Kelly D.A. (1966) Stress fracture of the first rib. American Journal of Orthopedics 8, 16-18 [PubMed] [Google Scholar]
- Edwards T.B., Murphy C. (2001) Nonunion of a dominant side first rib fracture in a baseball pitcher. Orthopedics 24, 599-600 [DOI] [PubMed] [Google Scholar]
- Fleisig G.S., Dillman C.J., Andrews J.R. (1994) Biomechanics of the shoulder during throwing In: The Athlete’s Shoulder. Andrews J.R.Wilk K.E.. New York, NY: Churchill Livingstone; 355-368 [Google Scholar]
- Gregory P.L., Biswas A.C., Batt M.E. (2002) Musculoskeletal problems of the chest wall in athletes. Sports Medicine 32, 235-250 [DOI] [PubMed] [Google Scholar]
- Gurtler R., Pavlov H., Torg J.S. (1985) Stress fracture of the ipsilateral first rib in a pitcher. American Journal of Sports Medicine 13, 277-279 [DOI] [PubMed] [Google Scholar]
- Lankenner P.A., Jr, Micheli L.J. (1985) Stress fracture of the first rib. A case report. Journal of Bone and Joint Surgery (Am) 67, 159-160 [PubMed] [Google Scholar]
- Mamanee P., Weinberg J., Curl L.A., McFarland E.G. (1999) Bilateral first rib and unilateral second rib stress fractures in a female athlete. Clinical Journal of Sport Medicine 9, 177-183 [DOI] [PubMed] [Google Scholar]
- Matsumoto T., Fujita K., Fujioka H., Tsunoda M., Yoshiya S., Kurosaka M., Mizuno K. (2003) Stress fracture of the first rib in a soccer player: a rare etiology of shoulder pain. Journal of Shoulder and Elbow Surgery 12, 197-199 [DOI] [PubMed] [Google Scholar]
- Mintz A.C., Albano A., Reisdorff E.J., Choe K.A., Lillegard W. (1990) Stress fracture of the first rib from serratus anterior tension: an unusual mechanism of injury. Annals of Emergency Medicine 19, 411-414 [DOI] [PubMed] [Google Scholar]
- Proffer D.S., Patton J.J., Jackson D.W. (1991) Nonunion of a first rib fracture in a gymnast. American Journal of Sports Medicine 19, 198-201 [DOI] [PubMed] [Google Scholar]
- Tullos H.S., Erwin W.D., Woods G.W., Wukasch D.C., Cooley D.A., King J.W. (1972) Unusual lesions of the pitching arm. Clinical Orthopaedics and Related Research 88, 169-182 [DOI] [PubMed] [Google Scholar]