

Abstract
Rate-dependent efficacy has been extensively documented in shock wave lithotripsy (SWL) stone comminution, with shock waves (SWs) delivered at a low rate producing more efficient fragmentation in comparison to those delivered at high rates. Cavitation is postulated to be the primary source underlying this rate phenomenon. Residual bubble nuclei that persist along the axis of SW propagation can drastically attenuate the waveform's negative phase, decreasing the energy which is ultimately delivered to the stone and compromising comminution. The effect is more pronounced at high rates, as residual nuclei have less time to passively dissolve between successive shocks. In this study, we investigate a means of actively removing such nuclei from the field using a low-amplitude acoustic pulse designed to stimulate their aggregation and subsequent coalescence. To test the efficacy of this bubble removal scheme, model kidney stones were treated in vitro using a research electrohydraulic lithotripter. SWL was applied at rates of 120, 60, or 30 SW/min with or without the incorporation of bubble removal pulses. Optical images displaying the extent of cavitation in the vicinity of the stone were also collected for each treatment. Results show that bubble removal pulses drastically enhance the efficacy of stone comminution at the higher rates tested (120 and 60 SW/min), while optical images show a corresponding reduction in bubble excitation along the SW axis when bubble removal pulses are incorporated. At the lower rate of 30 SW/min, no difference in stone comminution or bubble excitation was detected with the addition of bubble removal pulses, suggesting that remnant nuclei had sufficient time for more complete dissolution. These results corroborate previous work regarding the role of cavitation in rate-dependent SWL efficacy, and suggest that the effect can be mitigated via appropriate control of the cavitation environment surrounding the stone.
Introduction
The efficacy of stone comminution in shock wave lithotripsy (SWL) is highly influenced by the rate of shock wave (SW) delivery. Extensive testing, both in vitro1–5 and in vivo,6 has demonstrated that the efficiency of stone fragmentation decreases by increasing SW rate. This work is corroborated by numerous human studies,7–13 in which it was observed that slow rates (60–90 SW/min) yield more successful outcomes than high rates (120 SW/min).
Mechanistically, cavitation is postulated to be the primary source of rate-dependent efficacy in SWL. It is well documented that SWs can generate extensive cavitation activity along their propagation path, with the size and density of the bubble population increasing with an increase in shock rate.1,14–16 The lifespan of SW-induced bubbles has been reported to be on the order of 1 ms,17–20 implying that they will undergo inertial collapse well before the arrival of the subsequent SW. However, recent work has shown that collapse of these primary bubbles produces a large population of smaller daughter bubbles—that is, cavitation nuclei—which can persist on the order of 1 second.21,22
A SW that propagates through a medium containing residual cavitation nuclei will experience selective attenuation of its negative phase.1,16,23,24 Since the cavitation nuclei are very small (<10 μm),24 they do not affect the compressional portion of the waveform. However, the tensile component of the SW will cause bubble nuclei to grow—a process that removes energy from the negative tail of the SW and transfers it to the propagation medium in the form of kinetic and potential energy of the fluid surrounding the bubbles.16 As such, the negative phase of the SW that ultimately reaches the stone is attenuated in both time and amplitude, leading to decreased efficacy of stone comminution. This effect is more pronounced at high shock rates, as residual cavitation nuclei have less time to passively dissolve between successive SWs.
In the present study, we examine a strategy for the active removal of residual bubble nuclei that persist after an SW in an effort to mitigate rate-dependent efficacy in SWL stone comminution. Preliminary work indicates that sonicating such nuclei with a low-intensity acoustic field can remove them from a medium by stimulating their aggregation and subsequent coalescence.
Materials and Methods
Model stones formulated to mimic the tensile fracture strength of naturally occurring cystine calculi were cast from a mixture of BegoStone plaster (BEGO, Smithfield, RI), albumin (Carolina Biological Supply Co., Burlington, NC), and tap water.25 A Delrin (DuPont, Wilmington, DE) plastic mold was used to create stone cylinders measuring 1 cm in diameter and having an initial hydrated mass of 1.02±0.03 g (mean±SD, n=30). During treatment, stone phantoms were held within a finger cot assembly (Fig. 1). The base of this structure is composed of Accura-60 (3D Systems, Inc., Rock Hill, SC) plastic fabricated on a stereolithography machine. It contains a concave basket with 2 mm holes on which the stone was placed for treatment; when stone debris was reduced to sub-2 mm size, it was able to pass through the basket and was considered treated. A vinyl finger cot (Wesco Enterprises, Inc., Santa Fe Springs, CA) measuring ∼2 cm in diameter and 3 cm in height was used to enclose the assembly and to ensure that both the stone and cavitation nuclei remained in the treatment zone. The finger cot assembly was filled with deionized water degassed to a dissolved oxygen level 80%±2% of saturation in order to mimic that of urine.26 It was subsequently placed into a larger treatment tank measuring 60×30×45 cm (L×W×H) that contained degassed water (dissolved oxygen level <15% of saturation) with a conductivity of 600 μS/cm (Fig. 2).
FIG. 1.

Finger cot assembly used to hold model kidney stones during shock wave lithotripsy (SWL) treatment. The base of the structure contains a concave basket with 2 mm holes onto which stones were placed. A vinyl finger cot was used to enclose the assembly and to ensure that both stone debris and cavitation nuclei remained in the treatment zone. Complete comminution was defined as the point at which all stone fragments had been reduced to <2 mm and passed through the basket.
FIG. 2.

Experimental setup used to assess SWL comminution efficacy. The finger cot assembly used to hold model stones was filled with deionized water degassed to a dissolved oxygen level 80% of saturation to mimic that of urine; it was subsequently placed into a larger treatment tank containing degassed water (dissolved oxygen level <15% of saturation) with a conductivity of 600 μS/cm. Shock waves (SWs) were delivered from a research electrohydraulic lithotripter patterned after the Dornier HM3, while bubble removal pulses were generated by a separate piezoelectric transducer oriented orthogonal to the axis of SW propagation.
SWL was delivered using an electrohydraulic research system designed to simulate the acoustic field generated by the Dornier HM3.27–29 A charging voltage of 20 kV was used for all treatments, which was calibrated to produce an acoustic SW having a peak positive pressure (p+) of 34 MPa and a peak negative pressure (p−) of 8 MPa. Electrohydraulic SWL electrodes were preconditioned using 200 SWs at 60 SW/min, and each electrode was replaced after the generation of 2000 SWs.
Bubble removal pulses were generated by a separate piezoelectric transducer (Steiner & Martins, Inc., Miami, FL) firing orthogonal to the SW propagation axis (Fig. 2). This transducer was composed of a flat disc with an active area measuring 5 cm in diameter, and generated a natural focal zone with −6-dB beamwidths measuring 2.5 cm in the lateral dimension and 14 cm in the axial; this natural focus was centered coincident with that of the electrohydraulic lithotripter. The bubble removal transducer was driven using an ENI AP400B controllable power amplifier (Electronic Navigation Industries, Inc., Rochester, NY) with 100 ms pulses at 370 kHz. A driving voltage of 470 Vpk−pk was utilized, which was calibrated to generate an acoustic output amplitude of 500 kPa. The timing scheme used for incorporating bubble removal pulses between successive SWs is displayed in Figure 3. After a given SW, a 500-μs delay was imposed before the arrival of the 100-ms bubble removal pulse. This allowed primary cavitation induced by the SW to undergo an unimpeded growth-collapse cycle before the sonication of remnant bubble nuclei.
FIG. 3.
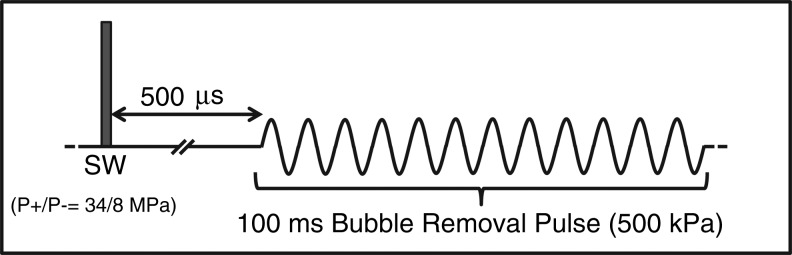
Pulse timing utilized for SWL treatments incorporating bubble removal pulses. A 500-μs delay was imposed between the SW and bubble removal pulse in order to allow SW-induced cavitation to undergo an uninhibited growth-collapse cycle. Bubble removal pulses had a frequency of 370 kHz, a duration of 100 ms, and an amplitude of 500 kPa.
To test the efficacy of active bubble removal in SWL, six different treatment schemes were applied to five model stones each. These included (1) SWL at 120 SW/min and (2) SWL at 120 SW/min with bubble removal; (3) SWL at 60 SW/min and (4) SWL at 60 SW/min with bubble removal; and (5) SWL at 30 SW/min and (6) SWL at 30 SW/min with bubble removal. Stones were treated until all debris had passed through the 2-mm holes of the basket in the finger cot assembly. The number of SWs required to achieve this complete comminution was recorded for each treatment.
In a separate set of experiments, the cavitation environment in the vicinity of the stone was optically monitored such as to correlate comminution efficacy to the extent of prefocal bubble excitation. An acrylic stone phantom, rather than BegoStone composites, was utilized for these imaging experiments in order to prevent stone debris from shielding our view of cavitation bubbles. In the same regard, the finger cot was removed from the stone holder assembly to provide an unobstructed imaging path. The entire treatment tank was maintained at a dissolved oxygen level 80% of saturation in this case, as the finger cot was no longer present to create a secluded treatment environment surrounding the stone. For each of the six treatment schemes, a sequence of 50 SWs was applied to the acrylic stone phantom. A single backlit image with 10 μs exposure was acquired 240 μs after the firing of each SW using a Point Grey Chameleon camera (Point Grey Research, Inc., Richmond, BC, Canada). This timing was empirically determined to correspond to the point of maximum SW-induced prefocal bubble excitation.
Results
Stone comminution resulting from each treatment scheme is summarized in Figure 4, while the corresponding level of prefocal bubble excitation is displayed in Figure 5. Consistent with previous studies, the number of SWs required to achieve complete stone comminution in conventional SWL was observed to decrease with a decrease in shock rate (t-test, p<0.0001), indicating that the “per-shock” efficiency is higher when a lower rate is used. Correspondingly, the extent of SW-induced bubble excitation was found to decrease as the shock rate was lowered from 120 to 30 SW/min (Fig. 5, top row).
FIG. 4.

Number of SWs required to achieve complete stone comminution (all debris <2 mm). The “per-shock” efficiency of conventional SWL was observed to increase as the shock rate was decreased. The incorporation of bubble removal pulses resulted in a drastic reduction in the number of SWs required for complete treatment at both 120 and 60 SW/min, while bubble removal produced no detectable difference in comminution efficacy at the lower rate of 30 SW/min.
FIG. 5.

Representative images capturing the degree of SW-induced prefocal bubble excitation for the six treatment schemes tested in this study. Each image corresponds to the 25th SW in a series of 50 SWs applied at the indicated rate. Cavitation along the SW axis was observed to decrease with a decrease in rate in conventional SWL (top row). The introduction of bubble removal (BR) pulses drastically reduced this cavitation at rates of 120 and 60 SW/min, whereas minimal bubble excitation was produced along the SW axis at the lower rate of 30 SW/min with or without bubble removal.
The introduction of bubble removal pulses resulted in a statistically significant reduction in the number of SWs required to achieve complete comminution at both 120 and 60 SW/min (t-test, p≤0.003). The most pronounced effect was observed at the highest utilized rate of 120 SW/min. Here, conventional SWL required 4893±375 SW to achieve complete comminution, whereas incorporation of bubble removal pulses decreased the required number of SWs to 2482±239 (t-test p<0.0001). Imaging of the cavitation environment surrounding the stone at this rate shows a drastic reduction in bubble excitation along the SW axis with the addition of bubble removal pulses (Fig. 5, leftmost column). Incorporation of bubble removal pulses at 60 SW/min also produced a prominent effect, reducing the number of SWs required for complete comminution from 2652±482 to 1487±388 (t-test, p=0.003). Analogous to the case of 120 SW/min, a decrease in bubble excitation along the SW axis is apparent with the addition of bubble removal pulses (Fig. 5, middle column).
The addition of bubble removal pulses in SWL applied at a lower rate of 30 SW/min did not produce any detectable effect on treatment efficacy, with complete comminution requiring 1054±152 SW for conventional SWL and 1070±182 SW for SWL with bubble removal (t-test, p=0.88). Correspondingly, the degree of bubble excitation was minimal for these two cases (Fig. 5, rightmost column).
Discussion
The rate-dependent efficacy of SWL stone comminution has been extensively documented in previous work, both in vitro1–5 and in vivo.6 These studies have shown that low rates of SW application produce more effective stone fragmentation in comparison to high rates. Clinical reports support these findings,7–13 demonstrating that more successful treatment outcomes are achieved using shock rates of 60–90 SW/min vs 120 SW/min. The phenomenon underlying this rate effect is related to cavitation—specifically, residual cavitation nuclei that can persist on the order of 1 second after the collapse of primary SW-induced bubbles.22 When an SW propagates through a medium containing residual cavitation nuclei, the negative phase of the waveform is attenuated as it causes these preexisting nuclei to swell.1,16,23,24 That is, energy is extracted from the tensile component of the SW and “left behind” in the medium, where it is stored in the form of kinetic and potential energy of the fluid surrounding the bubbles.16 In this way, the energy that ultimately propagates to the stone is reduced, and the efficacy of comminution is hindered. A more pronounced effect is observed at high rates due to the fact that residual cavitation nuclei have less time to passively dissolve between successive SWs.
In this study, we explored a means of mitigating the rate-dependent efficacy associated with SWL: active bubble removal. If the high efficiency associated with SWs applied at low rates is, indeed, a result of remnant cavitation nuclei having sufficient time to passively dissolve between successive SWs, it should be possible to achieve similar efficacy at higher rates if one can actively clear the field of residual bubbles before the arrival of the subsequent SW. Here, we have developed a low-amplitude acoustic pulse that achieves this bubble removal by stimulating the aggregation and subsequent coalescence of remnant nuclei. Briefly, when a population of microscopic nuclei is sonicated with a low-amplitude pulse, the bubbles will undergo radial oscillations and two major sets of forces will develop. The first, the Primary Bjerknes force, will tend to cause bubbles to move up the pressure gradient to the maximum of the pressure field. The second, the Secondary Bjerknes force, will tend to cause individual bubble nuclei to be attracted to one another. The relative contributions of these forces manifest in the population of residual bubble nuclei aggregating together and, in our observations, coalescing into a minimal number of remnant bubbles. Our preliminary study regarding this phenomenon suggests that a population of hundreds or even thousands of cavitation nuclei can coalesce into a single microscopic remnant bubble. A full demonstration of this process and characterization of the physical phenomena involved is the subject of a separate manuscript that is currently under preparation.
The results of this study corroborate previous work regarding the role of cavitation in SWL rate-dependent efficacy. Consistent with earlier studies,1–6 we observed the efficiency of SWL stone comminution to decrease as the rate of SW application was increased (Fig. 4). As was also observed by others,1,14–16 optical monitoring of the cavitation environment in the vicinity of the stone showed that the size and density of the bubble population increased with an increase in shock rate (Fig. 5). The introduction of bubble removal pulses drastically increased “per-shock” efficiency at rates of 120 and 60 SW/min (Fig. 4), and corresponding images showed a pronounced reduction in bubble excitation along the SW propagation path (Fig. 5). This supports the idea that excitation of remnant bubble nuclei limits the efficacy of SWs,1,16,23,24 and indicates that removing them from the field between successive SWs can drastically improve stone comminution. A similar result has been documented by Lautz et al.,30 who used a jet of degassed water to remove cavitation nuclei from the coupling cushion of an electromagnetic lithotripter and improve stone fragmentation in vitro. In their study, it was demonstrated that incorporation of the water jet between successive SWs resulted in a reduction in prefocal cavitation; correspondingly, hydrophone measurements indicated that attenuation of the SW's negative phase was mitigated when the jet was present.
Other recent work exploring the role of cavitation in SWL has further characterized rate-dependent comminution as the result of bubble proliferation.21,22 It was found that inertial collapse and jetting of primary SW-induced bubbles produces a cloud of smaller daughter nuclei, with a single primary bubble giving rise to dozens of residual daughters. Furthermore, as bubbles proliferated from shot to shot, the amplitude of the negative phase of the SWs was observed to decline. At higher shock rates, this proliferation of bubbles was more substantial, presumably due to the fact that there is less time for bubble dissolution between successive shocks. The authors of the study went on to conclude that it may take very few bubbles to seed a substantial cavitation cloud—and as such, substantial reduction of the tensile component of the SW—at rates used in clinical SWL. In this regard, the bubble coalescing pulses used in this study can be viewed as a means of mitigating the bubble proliferation phenomenon. If we can prevent the build-up of substantial cavitation by coalescing the daughter nuclei after each SW, the overall efficacy of the treatment should be much improved.
The bubble removal strategy presented in this work offers a promising approach for enhancing the efficacy of SWL therapy. If “per-shock” efficiency can be maintained at high rates of SW application, treatments could be performed faster with more complete stone comminution. However, it should be noted that high shock rates are associated with increased collateral tissue damage, and an evaluation of the ability of bubble removal pulses to mitigate this damage remains for future work. In the present study, bubble removal was observed to decrease the time to complete comminution by 49% and 44% at shock rates of 120 and 60 SW/min, respectively. These results were acquired using a relatively hard stone model (cystine-mimicking), and we anticipate similar improvements in comminution for more typical stone compositions such as calcium oxalate. It should be noted that the bubble removal pulses utilized in this study have not yet been fully optimized, and we expect further increases in SW efficiency after a full investigation of the parameter space. Finally, while this study offers promising results in an in vitro setting, translation to an in vivo model is a crucial next step in demonstrating the viability of acoustic bubble removal as an adjunct to SWL therapy. For this reason, our future work will include an assessment of both stone comminution and collateral tissue effects resulting from the incorporation of bubble removal pulses in an in vivo setting.
Conclusions
Active removal of residual bubble nuclei after an SW pulse can dramatically improve the in vitro comminution efficacy of SWL at higher rates (120 and 60 SW/min). This supports the concept that remnant bubble nuclei that persist from shock to shock have deleterious effects on stone comminution, corroborating previous work regarding the role of cavitation in the rate-dependent efficacy of SWL. Further development of this approach for active bubble removal could translate to faster and more complete SWL therapy.
Abbreviations Used
- SW
shock wave
- SWL
shock wave lithotripsy
Acknowledgments
Research reported in this publication was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under award number R01DK091267. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
W.W.R., C.A.C., and T.L.H. have financial interests and/or other relationships with HistoSonics, Inc.
References
- 1.Pishchalnikov YA, McAteer JA, Williams JC, Jr., Pishchalnikova IV, Vonderhaar RJ. Why stones break better at slow shockwave rates than at fast rates: In vitro study with a research electrohydraulic lithotripter. J Endourol 2006;20:537–541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vallancien G, Munoz R, Borghi M, Veillon B, Brisset JM, Daudon M. Relationship between the frequency of piezoelectric shock waves and the quality of renal stone fragmentation. In vitro study and clinical implications. Eur Urol 1989;16:41–44 [DOI] [PubMed] [Google Scholar]
- 3.Wiksell H, Kinn AC. Implications of cavitation phenomena for shot intervals in extracorporeal shock wave lithotripsy. Br J Urol 1995;75:720–723 [DOI] [PubMed] [Google Scholar]
- 4.Greenstein A, Matzkin H. Does the rate of extracorporeal shock wave delivery affect stone fragmentation? Urology 1999;54:430–432 [DOI] [PubMed] [Google Scholar]
- 5.Weir MJ, Tariq N, Honey RJ. Shockwave frequency affects fragmentation in a kidney stone model. J Endourol 2000;14:547–550 [DOI] [PubMed] [Google Scholar]
- 6.Paterson RF, Lifshitz DA, Lingeman JE, et al. Stone fragmentation during shock wave lithotripsy is improved by slowing the shock wave rate: studies with a new animal model. J Urol 2002;168:2211–2215 [DOI] [PubMed] [Google Scholar]
- 7.Madbouly K, El-Tiraifi AM, Seida M, El-Faqih SR, Atassi R, Talic RF. Slow versus fast shock wave lithotripsy rate for urolithiasis: A prospective randomized study. J Urol 2005;173:127–130 [DOI] [PubMed] [Google Scholar]
- 8.Yilmaz E, Batislam E, Basar M, Tuglu D, Mert C, Basar H. Optimal frequency in extracorporeal shock wave lithotripsy: Prospective randomized study. Urology 2005;66:1160–1164 [DOI] [PubMed] [Google Scholar]
- 9.Pace KT, Ghiculete D, Harju M. Shock wave lithotripsy at 60 or 120 shocks per minute: a randomized, double-blind trial. J Urol 2005;174:595–599 [DOI] [PubMed] [Google Scholar]
- 10.Chacko J, Moore M, Sankey N, Chandhoke PS. Does a slower treatment rate impact the efficacy of extracorporeal shock wave lithotripsy for solitary kidney or ureteral stones? J Urol 2006;175:1370–1373 [DOI] [PubMed] [Google Scholar]
- 11.Kato Y, Yamaguchi S, Hori J, Okuyama M, Kakizaki H. Improvement of stone comminution by slow delivery rate of shock waves in extracorporeal lithotripsy. Int J Urol 2006;13:1461–1465 [DOI] [PubMed] [Google Scholar]
- 12.Weiland D, Lee C, Ugarte R, Monga M. Impact of shockwave coupling on efficacy of extracorporeal shockwave lithotripsy. J Endourol 2007;21:137–140 [DOI] [PubMed] [Google Scholar]
- 13.Semins MJ, Trock BJ, Matlaga BR. The effect of shock wave rate on the outcome of shock wave lithotripsy: A meta-analysis. J Urol 2008;179:194–197; discussion 7. [DOI] [PubMed] [Google Scholar]
- 14.Sapozhnikov OA, Khokhlova VA, Bailey MR, et al. Effect of overpressure and pulse repetition frequency on cavitation in shock wave lithotripsy. J Acoust Soc Am 2002;112:1183–1195 [DOI] [PubMed] [Google Scholar]
- 15.Huber P, Jochle K, Debus J. Influence of shock wave pressure amplitude and pulse repetition frequency on the lifespan, size and number of transient cavities in the field of an electromagnetic lithotripter. Phys Med Biol 1998;43:3113–3128 [DOI] [PubMed] [Google Scholar]
- 16.Pishchalnikov YA, Sapozhnikov OA, Bailey MR, Pishchalnikova IV, Williams JC, McAteer JA. Cavitation selectively reduces the negative-pressure phase of lithotripter shock pulses. Acoust Res Lett Online 2005;6:280–286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sass W, Dreyer HP, Kettermann S, Seifert J. The role of cavitational activity in fragmentation processes by lithotripters. J Stone Dis 1992;4:193–207 [PubMed] [Google Scholar]
- 18.Zhong P, Cioanta I, Cocks FH, Preminger GM. Inertial cavitation and associated acoustic emission produced during electrohydraulic shock wave lithotripsy. J Acoust Soc Am 1997;101:2940–2950 [DOI] [PubMed] [Google Scholar]
- 19.Zhong P, Tong HL, Cocks FH, Preminger GM. Transient oscillation of cavitation bubbles near stone surface during electrohydraulic lithotripsy. J Endourol 1997;11:55–61 [DOI] [PubMed] [Google Scholar]
- 20.Cleveland RO, Sapozhnikov OA, Bailey MR, Crum LA. A dual passive cavitation detector for localized detection of lithotripsy-induced cavitation in vitro. J Acoust Soc Am 2000;107:1745–1758 [DOI] [PubMed] [Google Scholar]
- 21.Pishchalnikov YA, McAteer JA, Pishchalnikova IV, Williams JC, Bailey MR, Sapozhnikov OA. (Eds.). Bubble proliferation in shock wave lithotripsy occurs during inertial collapse. In: 18th International Symposium on Nonlinear Acoustics, Stockholm, Sweden, AIP Conf. Proc., 2008, pp 460–463 [Google Scholar]
- 22.Pishchalnikov YA, Williams JC, McAteer JA. Bubble proliferation in the cavitation field of a shock wave lithotripter. J Acoust Soc Am 2011;130:EL87–EL93 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pishchalnikov YA, McAteer JA, Bailey MR, Pishchalnikova IV, Williams JC, Evan AP. (Eds.). Acoustic shielding by cavitation bubbles in shock wave lithotripsy (SWL). In: 17th International Symposium on Nonlinear Acoustics 2005: American Institute of Physics, AIP Conf Proc., 2006, pp 319–322 [Google Scholar]
- 24.Pishchalnikov YA, McAteer JA, Williams JC, Jr., Effect of firing rate on the performance of shock wave lithotriptors. BJU Int 2008;102:1681–1686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Simmons WN, Cocks FH, Zhong P, Preminger G. A composite kidney stone phantom with mechanical properties controllable over the range of human kidney stones. J Mech Behav Biomed Mater 2010;3:130–133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gardner EA, Fowlkes JB, Carson PL, Ivey JA, Ohl DA. (Eds.). Bubble generation in excised canine urinary bladders using an electrohydraulic lithotripter. In: 1993 Ultrasonics Symposium Proceedings, Levy M, McAvoy BR, eds., Institute for Electrical and Electronics Engineers, Piscataway, NJ, IEEE Cat. #93CH3301-9, 1993, pp 905–908 [Google Scholar]
- 27.Coleman AJ, Saunders JE, Choi MJ. An experimental shock wave generator for lithotripsy studies. Phys Med Biol 1989;34:1733–1742 [DOI] [PubMed] [Google Scholar]
- 28.Cleveland RO, Bailey MR, Fineberg N, et al. Design and characterization of a research electrohydraulic lithotripter patterned after the Dornier HM3. Rev Sci Instrum 2000;71:2514–2525 [Google Scholar]
- 29.Duryea AP, Roberts WW, Cain CA, Hall TL. (Eds.). Optically triggered solid state driver for shock wave therapy. In: 11th International Symposium on Therapeutic Ultrasound, New York, NY, AIP Conf. Proc. 1481, 2011, pp 76–80 [Google Scholar]
- 30.Lautz J, Sankin G, Zhong P. Turbulent water coupling in shock wave lithotripsy. Phys Med Biol 2013;58:735–748 [DOI] [PMC free article] [PubMed] [Google Scholar]