

Abstract
The study of marital dissolution (i.e. divorce and separation) and mortality has long been a major topic of interest for social scientists. We conducted meta-analyses and meta-regressions on 625 mortality risk estimates from 104 studies, published between 1955 and 2011, covering 24 countries, and providing data on more than 600 million persons. The mean hazard ratio (HR) for mortality in our meta-analysis was 1.30 (95% confidence interval [CI], 1.23-1.37) among HRs adjusted for age and additional covariates. The mean HR was higher for men (HR, 1.37; 95% CI, 1.27-1.49) than for women (HR, 1.22; 95% CI: 1.13-1.32), but the difference between men and women decreases as the mean age increases. Other significant moderators of HR magnitude included sample size; being from Western Europe, Israel, the United Kingdom and former Commonwealth nations; and statistical adjustment for general health status.
Keywords: Meta-analysis, Meta-regression, Marital dissolution, Mortality, Gender, Age
Introduction
The association between marital status, health, and mortality was one of the first issues to be systematically studied by sociologists and demographers, dating back to Durkheim’s classic study on suicide (Durkheim, 1951 [1897]). Over the years, numerous studies have examined this relationship, with many of them focusing on the risk of death among divorced and separated persons. The vast majority of these studies reported an increased risk of death for divorced and separated people. However, a few studies found no significant association (Burgoa et al., 1998; Goldman et al., 1995) and the magnitude of the relative risk varied substantially. Specifically, the wide range of mortality risks often varies by socio-demographic variables such as gender (Burgoa et al., 1998; Kolip, 2005; Kravdal, 2003; Zajacova, 2006), age (Breeze et al., 1999; Helweg-Larsen et al., 2003), geographical location (Artnik et al., 2006; Keller, 1969), and how well the study controlled for covariates (Bagiella et al., 2005; Moos et al., 1994).
Three main streams of research emerge from the literature: research into possible confounding, examinations of possible mediating mechanisms, and studies of possible moderating factors. We begin with a brief review of research on confounding factors and on potential mediators. The current trend in the literature, however, is towards identifying the role of moderating factors in the marital dissolution-mortality association (Hughes & Waite, 2009; Williams & Umberson, 2004). Since meta-analysis and meta-regression techniques are well suited for investigating these moderating factors, we focus the present paper on this latter research stream.
Research on confounding factors
First, some scholars have suggested that the association between marital dissolution and mortality may in fact be at least partly spurious. According to this line of reasoning, this association is largely the result of physical health, psychological health, economic, and behavioral factors. For example, Mastekaasa (1994) argued that low psychological wellbeing of either one or both partners may in fact be present for many years before marital dissolution and serve as one of the main causes for this dissolution. Parlin and Johnson (1977) and Rushing (1979) also argued that those who are psychologically unstable may be less able to sustain marriages. Similarly, Gottman and Levenson (1992) showed that lower physical health may predict marital dissolution. People who suffer from physical health problems are not only less likely to get married, but are also more likely to suffer from marital stress, marital problems, and eventually marital dissolution
Preexisting economic difficulties may also increase the likelihood of marital dissolution rather than being its result. Hansen (2005) for example, who conducted an eight year panel data study of unemployment and marital dissolution, found that unemployment leads to an increased risk of martial dissolution. Yet, as many other studies have previously shown, unemployment and economic adversity are also clearly associated with health problems (Alavinia & Burdorf, 2008; Bambra & Eikemo, 2009; Hammarstrom, 1994; Janlert, 1997; Jin et al., 1995; Murphy & Athanasou, 1999) and a higher risk of mortality (Ahs & Westerling, 2006; Costa & Segnan, 1987; Iversen et al., 1987; Martikainen, 1990; Moser et al., 1987; Tsai et al., 2004). Finally, a variety of behaviors which may be damaging to a person’s health and increase the risk of mortality may also lead to marital tensions and higher marital dissolution rates. These include, among others, excessive substance abuse, alcoholism, smoking, reckless driving, inadequate diets, and eating disorders (Amato & Rogers, 1987; Mudar et al., 2001; Wyke & Ford, 2002; Yamaguchi & Kandel, 1997).
Research on mediation mechanisms
Previous studies suggested three predominant factors through which marital dissolution may lead to negative health consequences: social support, economic well-being, and physical and mental health. First, much of the sociological and public health literature has concluded that social support provides people with a variety of physical and mental health benefits that decrease mortality rates (e.g. Berkman, 1985; Blazer, 1982; Cornell, 1992; Litwak et al., 1989; Rosengren et al. 1993; Schaefer et al., 1981; Uchino et al., 1996). In her analysis of Japanese families, Cornell (1992) found that married women enjoy better relationships within the household and consequently lower mortality rates. Lye (1996) found that divorce weakens parent-child relations, and Kalmijn (2007) showed that when men divorce, they tend to receive reduced social support from their children. These studies suggest that marriage provides people with important resources in the form of social support, which may serve as a buffer against health problems and mortality risks. When the marriage ends, this support system often weakens, and with it also the emotional support and regulation of health behaviors associated with being married (Ross et al., 1990; Umberson et al., 1992)
A second mediating factor examined in the marital dissolution literature is economic well-being. Both Lillard and Waite (1995) and Rogers (1995) showed that divorced and separated people die at a higher rate than married people, and that the relationship is explained partly by economic factors. Smock’s (1993, 1994) findings suggested that financially women are more adversely affected by divorced. Duncan and Hoffman (1985) found that if women remarry, the negative effect of their previous economic loss is eliminated. McManus and DiPrete (2001), while acknowledging the economic disadvantages of women following divorce, showed that men also incurred a serious financial penalty from divorce due to the loss of a second income and the payment of child support. Such economic disadvantages may, with time, translate into diminished health coverage and cheaper and less healthy nutrition, which eventually lead to poorer health and higher mortality rates.
The third mediating factor emphasized in the marital dissolution literature relates to stress and mental health (Williams & Umberson, 2004). Some have argued for a marital resource model, suggesting that marriage increases people’s psychological well-being (Cherlin et al., 1998; Gove, 1973). Kessler and Essex (1982), for example, found that married people are less susceptible to stressful events, an advantage which is lost when the marriage ends. Others suggested that marital dissolution itself may have a negative effect on mental health (Parlin & Johnson, 1977; Williams et al., 2008), which may lead to higher mortality rates. According to this crisis model, the stress associated with marital dissolution directly undermines health (Booth & Amaro, 1991; Williams et al., 1992).
Moderating Factors in the Marital Dissolution-Mortality Association
The contribution of meta-analysis and meta-regression techniques to our understanding of confounding and mediation mechanisms is limited. However, these methods are especially helpful in investigating moderating factors in the relationship of marital dissolution and mortality. In a recent meta-analysis of marital status (including marital dissolution) and mortality among the elderly, Manzoli et al. (2007) found that divorced and separated persons had a 16% higher risk of mortality than the risk of married persons. The inclusion criteria they used, however, were quite restrictive and their analysis leaves many questions unanswered. Their study examined only the elderly (65 and older), was limited to studies published between 1994 and 2005, and included relative risks (RRs) only if the original studies adjusted for age, sex, and additional covariates.
Additional meta-analyses are therefore needed to determine the magnitude of the association for younger age groups and to determine whether gender or geographic region become significant factors once these younger age groups are included in the analysis (both gender and region were non-significant in the Manzoli et al. study). Furthermore, Manzoli et al. only examined the effects of statistical adjustment and follow-up duration on the risk of mortality of married vs. unmarried individuals, a category in which divorced/separated, widowed, and never married individuals were joined together. Therefore, no conclusion could be drawn regarding marital dissolution and trends in mortality risk over time were not investigated.
Perhaps the most interesting finding in the analysis of Manzoli et al. (2007) was the lack of a statistically significant difference in the risk of mortality between divorced men and divorced women. This finding is especially surprising given that a host of previous studies have established the existence of a gender difference in the risk; divorced men were often found to be at a higher risk for health problems and mortality than divorced women (e.g. Burgoa et al., 1998; Hajdu et al., 1995; Ikeda et al., 2007; Kolip, 2005; Lillard & Waite, 1995). This suggests a possible interaction effect between age and gender, where the gender differences in the risk for mortality following marital dissolution diminish at older ages. This supposition seems to be supported by the findings of a number of studies which showed that the risk of mortality following marital dissolution is higher at younger ages than it is at older ages (e.g. Hajdu et al., 1995; Kravdal, 2007). However, other researchers have suggested that because older adults often experience a pile-up effect of stressors, the negative health effects of marital dissolution should be greater for older compared to younger individuals (Ensel & Lin, 2000; Ensel et al., 1996; Williams & Umberson, 2004).
Another potentially important moderating factor is the recency of the marital dissolution. Williams and Umberson (2004) suggested that the health decline associated with marital dissolution should dissipate with time. Conversely, Hughes and Waite (2009) have found that those people who spent a greater portion of their lives divorced had more health problems. To date, very few studies have compared varying follow-up durations in order to empirically examine the moderating effects of marital dissolution recency on the risk of mortality. The few that have done so mostly found higher mortality rates when marital dissolution occurred more recently, but results were not consistent (Brockmann & Klein, 2002; Jenkinson et al., 1993). Furthermore, gender is potentially implicated with respect to the moderating effects of dissolution recency because men are more likely than women to remarry (Glick & Lin, 1987), and remarriage serves as a potential buffer against the long-term harmful effects of marital dissolution.
The potential role of cultural differences is also of interest as marital dissolution has been studied extensively across the globe. Some of the previous studies reported particularly high (two to five times higher) mortality hazard ratios following marital dissolution in Eastern European countries (Artnik et al., 2006; Dzurova, 2000; Malyutina et al., 2004), in Scandinavia (Rosengren et al., 1993; Rosengren et al., 1989; Villingshoj et al., 2006), and in Japan (Nagata et al., 2003). Yet other studies of Eastern European (Mollica et al., 2001) and Scandinavian (Nilsson et al., 2005; Nybo et al., 2003; Samuelsson & Dehlin, 1993) countries found either no association between marital dissolution and mortality, or even at times a negative association, where divorced people lived longer. While a pattern is difficult to discern, culture is clearly a potential moderator of the marital dissolution-mortality association. Theoretically, one may expect marital dissolution to have a more substantial negative impact in relatively conservative and traditional societies (such as East Asia or the Arab world), where divorce is looked upon unfavorably and the cultural stigma is stronger.
Hypotheses
The present meta-analysis contributes to the body of knowledge on marital dissolution by utilizing the heterogeneity of research settings found in the literature to assess the impact of potential moderators. Some, such as gender and age, are easier to evaluate within an individual study (although most previous studies still did not examine them). Others—such as marital dissolution recency and cultural differences—have rarely been addressed by individual studies and are much more easily examined by comparing across studies. Meta-analysis and meta-regression techniques are well-suited to this task, allowing more nuanced comparisons of various moderators. Following our theoretical discussion, we conduct tests of gender-age interactions, gender-recency interactions, geographic region, time period, and a number of specific study design characteristics. The research reviewed above suggests a number of hypotheses regarding potential moderating factors. We test five basic hypotheses:
H1: The overall mortality hazard ratio of those who experienced marital dissolution will be higher than the mortality hazard ratio of married people.
H2: The mortality hazard ratio associated with marital dissolution will be greater for younger age groups than for older ones.
H3: Divorced men will have a higher mortality hazard ratio than divorced women. However, this difference will be most pronounced in younger ages, and in older ages the difference in risk will decline.
H4: The harmful effects of marital dissolution will be most pronounced during the first few years following marital dissolution and will decrease thereafter. This decrease, however, will be more substantial for men than for women.
H5: The harmful effects of marital dissolution will be more strongly felt by individuals in relatively traditional and conservative cultures.
Methods
Search strategy and coding procedures
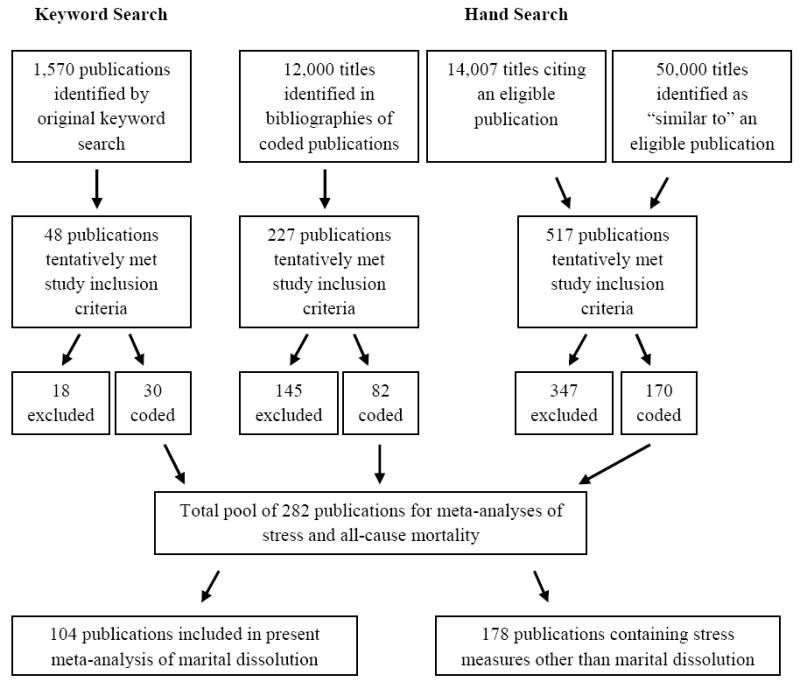
In June 2005, we conducted a search of electronic bibliographic databases to retrieve all publications combining the concepts of psychosocial stress and all-cause mortality. We used 100 search clauses for Medline, 97 for EMBASE, 81 for CINAHL, and 20 for Web of Science (see Section 1 of Appendix for the full search algorithm used for Medline; information on the remaining search algorithms is available from authors upon request). We identified 1570 unique publications. Using these results as a base, we iteratively searched the bibliographies of eligible publications; the lists of sources citing an eligible publication; and the sources identified as “similar to” an eligible publication. We exhausted the literature after 9 iterations (the full description of this iterative search protocol is available from the authors upon request). We re-ran the electronic keyword searches in these databases and completed the search and coding stages in January 2012.
The electronic database searches were performed by a research librarian. Two authors trained in meta-analysis coding procedures independently determined publication eligibility and extracted the data from the articles. Data was entered into and publications were tracked throughout the process using basic spreadsheets (See Section 2 of Appendix for full list of variables for which data were sought). Any unpublished work encountered was considered for study inclusion. Although our search was conducted in English, we were able to locate and translate the relevant portions of 35 publications written in German, Danish, French, Spanish, Dutch, Polish, or Japanese. The most frequent reasons for study exclusion include the lack of an eligible psychosocial stress or social isolation measure, failure to report a ratio measure of mortality risk, and confounding in the dependent variable such that the outcome was not strictly all-cause mortality. Figure 1 summarizes the number of publications considered at each step of the search process. The full database contains 282 publications examining the effects of various stressful events on all-cause mortality. To evaluate coding accuracy we randomly selected and recoded 40 of these publications (including 446 point estimates). No major errors were found.
Figure 1. Flow Chart for Literature Search.
The present analysis uses the subset of articles (n = 104) that reported the effect of marital dissolution on all-cause mortality. 98 of these publications appeared in peer-reviewed journals; four in a book chapter; and one in an unpublished dissertation. One publication was translated from Spanish, two from Danish, and one from German in consultation with native speakers; the remaining 100 publications were in English (see Table 1).
Table 1.
Studies Included in the Analyses
| Publication | Data Source | Country | Years | Sample Size | Mean HR | Number of HRs |
|---|---|---|---|---|---|---|
| Artnik et al. 2006 | Census, 1991 | Slovenia | 1991-1998 | 1,927,000 | 1.88 | 2 |
| Bagiella et al. 2005 | EPESE | United States | 1981-2002 | 14,456 | 1.19 | 6 |
| Ben-Shlomo et al. 1993 | Whitehall Study | United Kingdom | 1967-1990 | 18,403 | 1.40 | 3 |
| Berkson 1962 | Census, 1950 | United States | 1949-1951 | 150,520,798 | 1.77 | 4 |
| Berntsen 2011 | Central Popul. Register | Norway | 1971-2007 | 712,000 | 1.11 | 2 |
| Breeze et al. 1999 | OPCS-LS | United Kingdom | 1971-1992 | 93,931 | 1.09 | 8 |
| Brockman & Klein 2002 | GSOEP | Germany | 1984-1998 | 18,538 | 1.30 | 16 |
| Brockmann & Klein 2004 | GSOEP | Germany | 1984-1998 | 12,484 | 1.24 | 8 |
| Burgoa et al. 1998 | Census, 1991 | Spain | 1991-1991 | 38,939,050 | 0.97 | 4 |
| Cheung 2000 | HALS | United Kingdom | 1984-1997 | 3,378 | 1.19 | 2 |
| Choi & Marks 2011 | NSFH | United States | 1987-2002 | 5,937 | 1.49 | 2 |
| Comstock & Tonascia 1977 | HCWC | United States | 1963-1971 | 47,423 | 1.21 | 2 |
| Doblhammer 2000 | Census, 1981 | Austria | 1981-1997 | 1,254,153 | 1.35 | 1 |
| Dupre et al. 2009 | HRS | United States | 1992-2006 | 8,715 | 1.27 | 1 |
| Dzurova 2000 | Census, 1990, 1995 | Czech Republic | 1990-1995 | 10,306,000 | 3.02 | 4 |
| Ebrahim et al. 1995 | BRHS | United Kingdom | 1978-1990 | 7,735 | 1.46 | 6 |
| Goldman & Hu 1993 | Census, 1975 | Japan | 1975-1985 | 111,940,000 | 1.87 | 2 |
| Goldman et al. 1995 | NHIS-SOA | United States | 1984-1990 | 7,478 | 1.00 | 2 |
| Goodwin et al. 1987 | NMTR | United States | 1969-1982 | 25,706 | 1.27 | 1 |
| Granlund et al. 2010 | FilaBavi Field Laboratory | Vietnam | 1999-2008 | 22,085 | 1.70 | 2 |
| Grundy & Kravdal 2008 | Census, 1980 | Norway | 1980-2003 | 1,530,101 | 1.76 | 6 |
| Grundy & Tomassini 2010 | ONS-LS | United Kingdom | 1971-2001 | 41,341 | 1.25 | 2 |
| Hajdu et al. 1995 | Census, 1969-1991 | Hungary, UK | 1969-1991 | 61,786,277 | 1.72 | 40 |
| Hank 2010 | GSOEP | Germany | 1984-2006 | 7,231 | 1.42 | 2 |
| Hayward & Gorman 2004 | NLSOM | United States | 1966-1990 | 4,562 | 1.56 | 1 |
| Helweg-Larsen et al. 2003 | DANCOS | Denmark | 1987-1999 | 6,693 | 1.82 | 1 |
| Hemstrom 1996 | Census, 1980 | Sweden | 1980-1986 | 1,896,626 | 1.55 | 4 |
| Henretta 2007 | HRS | United States | 1994-2002 | 4,335 | 1.14 | 2 |
| Henretta 2010 | HRS | United States | 1994-2002 | 8,918 | 1.26 | 2 |
| Horwitz & Weber 1974 | Census, 1968 | Denmark | 1968-1968 | 1,710,800 | 2.11 | 14 |
| Horwitz & Weber 1974 | Census, 1968 | Denmark | 1968-1968 | 1,710,800 | 1.83 | 6 |
| Hurt et al. 2004 | HDSS | Bangladesh | 1982-1998 | 14,803 | 1.47 | 4 |
| Ikeda et al. 2007 | JCCSECR | Japan | 1988-1999 | 90,064 | 1.26 | 10 |
| Iribarren et al. 2005 | CARDIA Study | United States | 1985-2000 | 5,115 | 1.68 | 2 |
| Iwasaki et al. 2002 | Komo-Ise Study | Japan | 1993-2000 | 11,565 | 1.44 | 4 |
| Jenkinson et al. 1993 | ASSET | United Kingdom | 1986-1990 | 1,376 | 0.70 | 3 |
| Johansen et al. 1996 | Danish Cancer Registry | Denmark | 1968-1994 | 7,302 | 1.09 | 4 |
| Johnson et al. 2000 | NLMS | United States | 1978-1989 | 281,460 | 1.33 | 16 |
| Joung et al. 1996 | Census, 1986 | Netherlands | 1986-1990 | 14,572,000 | 1.56 | 2 |
| Kalediene et al. 2007 | Census, 1989, 2001 | Lithuania | 1989-2001 | 3,670,000 | 1.43 | 4 |
| Kaplan & Kronick 2006 | NHIS | United States | 1989-1997 | 80,018 | 1.25 | 1 |
| Keller 1969 | Original Data | United States | 1959-1966 | 706 | 0.92 | 2 |
| Kohler & Kohler (unpublished) | Danish Twin Registry | Denmark | 1968-2000 | 7,093 | 1.20 | 4 |
| Kohler & Preston 2011 | Census, 1992 | Bulgaria | 1993-1998 | 1,976,644 | 1.56 | 4 |
| Kolip 2005 | Census, 1999 | Germany | 1999-2000 | 45,500,000 | 2.08 | 2 |
| Kraus & Lilienfeld 1959 | Census, 1950 | United States | 1949-1951 | 150,520,798 | 1.81 | 32 |
| Kravdal 2003 | Census, 1960-1990 | Norway | 1960-1999 | 31,998 | 1.09 | 3 |
| Kravdal 2007 | Census, 1980, 1990 | Norway | 1980-1999 | 4,091,000 | 1.48 | 8 |
| Kroenke et al. 2006 | Nurses’ Health Study | United States | 1992-2004 | 2,835 | 0.93 | 2 |
| Kumle & Lund 2000 | Census, 1970 | Norway | 1970-1989 | 1,338,716 | 1.34 | 8 |
| Laaksonen et al. 2009 | Population Register | Finland | 1999-2004 | 506,000 | 1.51 | 1 |
| Lillard & Panis 1996 | PSID | United States | 1984-1990 | 4,092 | 1.09 | 4 |
| Liu 2009 | NHIS-LMF | United States | 1986-2002 | 517,314 | 1.13 | 2 |
| Liu & Sullivan 2003 | Original Data | United States | 1994-1998 | 646 | 1.52 | 2 |
| Makuc et al. 1990 | NHANES I | United States | 1971-1984 | 3,181 | 1.10 | 2 |
| Malyutina et al. 2004 | Novosibirsk MONICA | Russia | 1984-1998 | 11,404 | 2.35 | 6 |
| Manor et al. 1999 | ILMS | Israel | 1983-1992 | 72,527 | 1.16 | 5 |
| Manor et al. 2000 | ILMS | Israel | 1983-1992 | 79,623 | 1.17 | 4 |
| Martelin 1996 | Census, 1970 | Finland | 1970-1975 | 4,606,307 | 1.25 | 4 |
| Martelin et al. 1998 | Census, 1970, ’75, ’80, ’85 | Finland | 1970-1990 | 4,606,307 | 1.10 | 4 |
| Martikainen 1990 | Census, 1980 | Finland | 1980-1985 | 4,779,535 | 1.91 | 2 |
| Martikainen 1995 | Census, 1980 | Finland | 1980-1985 | 4,779,535 | 1.44 | 2 |
| Martikainen et al. 2005 | Census, 1975, 1995 | Finland | 1975-2000 | 3,165,000 | 1.40 | 24 |
| Matthews & Gump 2002 | MRFIT | United States | 1982-1990 | 12,336 | 1.30 | 2 |
| Mellstrom et al. 1982 | Census, 1968-1978 | Sweden | 1968-1978 | 7,914,000 | 1.34 | 2 |
| Mendes DeLeon et al 1992 | KRIS | Netherlands | 1972-1982 | 3,365 | 1.21 | 3 |
| Metayer et al. 1996 | WDCDCS | United States | 1990-1993 | 138 | 0.36 | 3 |
| Mollica et al. 2001 | Original Data | Croatia | 1996-1999 | 529 | 0.80 | 1 |
| Molloy et al. 2009 | Scottish Health Survey | United Kingdom | 1995-2006 | 7,788 | 1.62 | 4 |
| Moos et al. 1994 | DVAMC | United States | 1986-1991 | 21,139 | 1.36 | 1 |
| Nagata et al. 2003 | Takayama Study | Japan | 1992-1999 | 3,505 | 5.23 | 3 |
| Nilsson et al. 2005 | MPP | Sweden | 1974-1992 | 53,111 | 0.77 | 2 |
| Norekval et al. 2010 | Original Data | Norway | 1992-2008 | 145 | 3.20 | 1 |
| Nybo et al. 2003 | Census, 1998 | Denmark | 1998-2000 | 2,249 | 0.81 | 4 |
| Ortmeyer 1974 | Census, 1960 | United States | 1959-1961 | 180,671,000 | 1.72 | 4 |
| Patel et al. 2010 | SEER Program | United States | 1992-2004 | 7,997 | 1.41 | 1 |
| Rahman 1993 | Matlab DSS | Bangladesh | 1974-1982 | 64,263 | 1.75 | 14 |
| Rahman 1997 | Matlab DSS | Bangladesh | 1974-1982 | 24,889 | 1.93 | 16 |
| Regidor et al. 2001 | Census, 1996 | Spain | 1996-1998 | 3,110,121 | 1.71 | 12 |
| Rendall et al. 2011 | SIPP | United States | 1984-1999 | 175,007 | 1.33 | 4 |
| Rosengren et al. 1989 | GMPPT | Sweden | 1970-1983 | 9,869 | 2.02 | 5 |
| Rosengren et al. 1993 | Original Data | Sweden | 1983-1991 | 752 | 2.51 | 2 |
| Samuelsson & Dehlin 1993 | Original Data | Sweden | 1922-1990 | 392 | 0.57 | 2 |
| Sheps 1961 | Census, 1950 | United States | 1949-1951 | 112,354,034 | 1.81 | 36 |
| Shkolnikov et al. 2007 | Census, 2001 | Lithuania | 2001-2004 | 3,481,295 | 1.69 | 4 |
| Shurtleff 1955 | Census, 1940, 1950 | United States | 1940-1951 | 150,520,798 | 1.89 | 22 |
| Shurtleff 1956 | Census, 1950 | United States | 1950-1951 | 150,520,798 | 1.72 | 8 |
| Singh & Siahpush 2001 | NLMS | United States | 1979-1989 | 301,183 | 1.14 | 6 |
| Singh & Siahpush 2002 | NLMS | United States | 1979-1989 | 300,910 | 1.34 | 3 |
| Smith & Waitzman 1994 | NHANES I | United States | 1971-1984 | 20,729 | 1.41 | 8 |
| Smith & Zick 1994 | PSID | United States | 1968-1987 | 2,604 | 1.09 | 4 |
| Sorlie et al. 1995 | NLMS | United States | 1979-1989 | 530,507 | 1.38 | 24 |
| Spence 2006 | NLS-MW | United States | 1967-2001 | 3,258 | 1.26 | 1 |
| Tucker et al. 1996 | Terman Life-Cycle Study | United States | 1950-1991 | 1,077 | 1.72 | 8 |
| Tucker et al. 1997 | Terman Life-Cycle Study | United States | 1950-1991 | 1,101 | 1.65 | 2 |
| Va et al. 2011 | SMHS | China | 2002-2008 | 52,147 | 2.49 | 2 |
| SWHS | China | 1996-2009 | 74,857 | 1.11 | 2 | |
| Vallin & Nizard 1977 | Census, 1968 | France | 1968-1968 | 49,780,543 | 1.05 | 30 |
| Van Poppel & Joung 2001 | Census, 1860-1960 | Netherlands | 1860-1969 | 11,486,630 | 1.44 | 2 |
| Villingshoj et al. 2006 | Danish Cancer Registry | Denmark | 1991-2002 | 770 | 2.49 | 5 |
| Wang et al. 2011 | SEER Program | United States | 1992-2008 | 127,753 | 1.23 | 4 |
| Xavier et al. 2010 | Epidoso EES | Brazil | 1991-2003 | 1,533 | 1.26 | 1 |
| Zajacova 2006 | NHANES I | United States | 1971-1992 | 12,036 | 1.21 | 2 |
| Zajacova & Hummer 2009 | NHIS | United States | 1986-2002 | 619,320 | 1.38 | 2 |
| Zick & Smith 1991 | PSID | United States | 1971-1984 | 1,990 | 1.28 | 4 |
Statistical methods and inclusion criteria
For the present analyses, a study was included if the outcome variable was all-cause mortality and a clear comparison was made between a group of people who were divorced or separated at baseline and another group who were married at baseline. No studies that used the general population were included in the analyses. In total, the 104 publications provided 625 point estimates for analysis. Cross-sectional studies were included in the analysis provided that the design of the study closely followed that of a longitudinal study. An indicator variable was created in order to examine the possible effects of this inclusion decision.
Statistical methods varied from study to study, necessitating the conversion of odds ratios, rate ratios, standardized mortality ratios, relative risks, and hazard ratios (HRs) into a common metric. All non-hazard-ratio point estimates were converted to hazard ratios—the most frequently reported type (See Section 3 of Appendix). As is standard practice, we used the standard errors reported in the publications to calculate the inverse variance weights. When not reported, standard errors were calculated using (1) confidence intervals, (2) t statistics, (3) χ2 statistics, or (4) p-values. When upper-limit p-values were the only estimate of statistical significance available (e.g. in cases where we knew only that the p-value lay somewhere between .01 and .05), the midpoint of the upper and lower limits was used to estimate the p-value. In 222 cases (out of the 625 point estimates) no measure of statistical significance was reported and standard errors were estimated using multiple regression (see section 4 of Appendix). An indicator variable was created so analyses could be conducted both with and without data points where the standard error was estimated.
Many meta-analysts prefer to use only the most general point estimates reported in a given publication. While this strategy makes it easier to maintain independence between point estimates and makes the calculations of the inverse variance weights straight-forward, it also results in a substantial loss of information. We sought instead to maximize the number of point estimates analyzed, capturing variability both between and within each publication rather than just the former (For a similar analytic strategy see Roelfs et al., 2010; 2011; Roelfs et al., 2011; Shor et al., 2012). In cases where a given set of person-years was represented more than once, we utilized a variance adjustment procedure (See Section 5 of Appendix).
To control for time- and location-specific marital dissolution norms, we gathered data on the number of divorces per 1,000 persons, matched to the remaining data by country and baseline start year. Data were obtained primarily from the United Nations Demographic Yearbook from 1958, 1976, 1982, 1990, 1991, 1993-2000, 2002, 2003, 2005, and 2006. Additional data were obtained from the 1869, 1879, 1889, 1899, 1909, and 1920 Netherlands Censuses and from the 1997 China Statistical Yearbook.
Two measures of study quality were adopted to assess study bias. First, the 2 authors who performed the coding assigned a 3-level subjective rating to each publication. Publications were rated as low quality if they contained obvious reporting errors or applied statistical methods incorrectly (in these cases, data were coded only when sufficient information was available to extract corrected relative risk estimates). Publications were rated as high quality if models were well-specified (i.e. the correct model was used relative to the state of the art at the time of publication) and discussions and reporting of study results were detailed. Second, based on the results of a principal components factor analysis, we constructed a scale measure (continuous, range = 0 to 10) using the following: (a) the 5-year impact factor (ISI Web of Knowledge, 2009) of the journal in which the article was published (an impact factor of 1 was assigned when the impact factor was not available); and (b) the number of citations received per year since publication according to ISI Web of Knowledge. See Section 6 of Appendix for additional information on the factor analysis. The Spearman correlation between the subjective rating and the factor-analysis-derived rating was low (rho = 0.173; p < 0.001). The factor analysis further indicated that these two measures tapped different dimensions of quality.
Both Q-tests and I2 measures were used to assess the presence and magnitude of heterogeneity in the data (Huedo-Medina, Sanchez-Meca, & Marin-Martinez, 2006). Q-test results from preliminary analyses revealed substantial heterogeneity across studies’ effect sizes. In light of this all meta-analyses and meta-regression analyses were calculated by maximum likelihood using a random effects model. Analysis was performed with SPSS 19.0 using matrix macros provided by Lipsey and Wilson (2001). The possibility of selection and publication bias was examined using a funnel plot of the log HRs against sample size. Due to heterogeneity in the data, funnel plot asymmetry was tested using both Egger’s test (Egger & Davey-Smith, 1998) and weighted least squares regressions of the log HRs on the inverse of the sample size (Moreno et al., 2009; Peters et al., 2006).
Analyses performed include meta-analyses of subgroups and multivariate meta-regression analyses. The following covariates were used in these analyses: (1) whether standard error was estimated (yes or no); (2) whether death rate was estimated (yes or no); (3) age of the publication, divided by 10; (4) age of the study, divided by 10; (5) age of the study, squared; (6) duration of the baseline period, in years; (7) years elapsed between the end of baseline and the beginning of follow-up; (8) maximum follow-up duration, in years; (9) whether a study used a longitudinal design; (10) whether study sample consisted of persons with previous stressful experiences or chronic health problems (yes or no); (11) proportion of respondents who were male; (12) mean age of sample at baseline, divided by 10; (13) age range of sample at baseline, divided by 10; (14) a series of interaction terms between gender, mean age, and follow-up duration; (15) a series of variables indicating whether gender, age, socioeconomic status, health, and other social characteristics were statistically controlled; (16) sample size, log transformed; (17) geographic region; (18) number of divorces per 1,000 population in corresponding nation-year; (19) subjective quality rating; and (20) the composite scale of study quality.
Results
Table 2 provides descriptive statistics on the 625 mortality risk estimates included in this study. Data were obtained from 104 studies published between 1955 and 2011, covering 24 countries, and representing more than 600 million people. Men and women are both well-represented in the dataset and 82.7% of the risk estimates came from study samples with mean ages greater than or equal to 40 years. The median of the maximum follow-up duration across all studies was 6.5 years. Of the HRs analyzed, Over 95% come from studies assigned a subjective quality rating of average or high; the mean 5-year impact factor was 3.59; and the mean number of citations received per year since publication was 2.07.
Table 2.
Distribution of mortality risk estimates (n = 625) in the analysis by selected variables
| Variable | Distribution | |
|---|---|---|
| Publication date | 1955-1959 | 9.9% |
| 1960-1969 | 6.7 | |
| 1970-1979 | 9.0 | |
| 1980-1989 | 1.3 | |
| 1990-1999 | 30.7 | |
| 2000-2011 | 42.4 | |
| Level of statistical adjustment | ||
| Unadjusted | 52.3% | |
| Adjusted for age only | 19.2 | |
| Adjusted for age and additional covariates | 28.5 | |
| Gender | Women only | 44.6% |
| Men only | 47.4 | |
| Both genders | 8.0 | |
| Mean age of study sample at baseline | < 20 | 0.8% |
| 20 – 29.9 | 5.8 | |
| 30 – 39.9 | 10.7 | |
| 40 – 49.9 | 23.3 | |
| 50 – 59.9 | 29.3 | |
| 60 – 69.9 | 9.6 | |
| 70 – 79.9 | 14.4 | |
| ≥ 80 | 6.1 | |
| Baseline start year | 1860 – 1939 | 2.9% |
| 1940 – 1949 | 12.1 | |
| 1950 – 1959 | 7.4 | |
| 1960 – 1969 | 13.9 | |
| 1970 – 1979 | 27.1 | |
| 1980 – 1989 | 20.0 | |
| 1990 – 2002 | 16.6 | |
| Stressed population? | Yes | 5.3% |
| No | 94.7 | |
| Longitudinal study design? | Yes | 61.9% |
| No | 38.1 | |
| Region | ||
| Scandinavia | 19.5% | |
| United States | 37.9 | |
| UK, Canada, Australia, and New Zealand | 7.7 | |
| East Europe | 7.5 | |
| West Continental Europe, Israel | 17.8 | |
| China, Japan, Taiwan, Vietnam | 4.0 | |
| Bangladesh, Brazil, Lebanon | 5.6 | |
| Follow-up duration | 1st Quartile | 2.5 years |
| Median | 6.5 | |
| 3rd Quartile | 11.25 | |
| Number of divorces per 1,000 population | 1st Quartile | 1.28 |
| Median | 2.39 | |
| 3rd Quartile | 2.75 | |
| Death rate estimated? | Yes | 35.5% |
| No | 64.5 | |
| Standard error estimated? | Yes | 40.5% |
| No | 59.5 | |
Table 3 presents the results of a number of meta-analyses. All analyses were stratified by the level of statistical adjustment of the risk estimate. Supporting our first hypothesis, persons who divorced or separated were significantly more likely to die than those who were married. The mean unadjusted HR was 1.51 (95% confidence interval [CI], 1.45-1.58; n = 327 HRs); age-adjusted HR, 1.49 (95% CI, 1.40-1.59; n = 120); and HR adjusted for age and additional covariates, 1.30 (95% CI, 1.23-1.37; n = 178). These results show that, in studies controlling for multiple covariates, marital dissolution is associated with a 30% higher risk of mortality. Table 3 also shows that the exclusion of HRs based on estimated death rates or the exclusion of HRs where the standard error was estimated does not substantively alter the mean HRs.
Table 3.
Meta-Analyses of the All-cause Mortality Risk for Divorced/Separated Persons Relative to Married Persons a
| Unadjusted | Adjusted for Age Only | Adjusted for Age and Additional Covariates b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P-value | NHR | Q-test P-value | HR (95% CI) | P-value | NHR | Q-test P-value | HR (95% CI) | P-value | NHR | Q-test P-value | |
| All available data | 1.51 (1.45, 1.58) | < 0.0001 | 327 | 0.2916 | 1.49 (1.40, 1.59) | < 0.0001 | 120 | 0.9214 | 1.30 (1.23, 1.37) | < 0.0001 | 178 | 0.9999 |
| Excluding point estimates converted to a HR using an estimated death rate | 1.47 (1.39, 1.56) | < 0.0001 | 219 | 0.1231 | 1.62 (1.45, 1.80) | < 0.0001 | 62 | 0.8821 | 1.32 (1.22, 1.43) | < 0.0001 | 122 | 0.9999 |
| Excluding HRs with estimated standard error | 1.51 (1.42, 1.60) | < 0.0001 | 141 | 0.0064 | 1.45 (1.36, 1.54) | < 0.0001 | 92 | 0.6927 | 1.33 (1.27, 1.40) | < 0.0001 | 139 | 0.5787 |
| Excluding cross-sectional studies | 1.35 (1.26, 1.44) | < 0.0001 | 125 | 0.0213 | 1.45 (1.36, 1.54) | < 0.0001 | 84 | 0.8193 | 1.30 (1.24, 1.36) | < 0.0001 | 178 | 0.7570 |
| Gender | ||||||||||||
| Women | 1.42 (1.33, 1.51) | < 0.0001 | 152 | 0.9999 | 1.26 (1.15, 1.39) | < 0.0001 | 52 | 0.9999 | 1.22 (1.13, 1.32) | < 0.0001 | 75 | 0.9999 |
| Men | 1.67 (1.57, 1.78) | < 0.0001 | 151 | < 0.0001 | 1.71 (1.57, 1.86) | < 0.0001 | 66 | 0.7347 | 1.37 (1.27, 1.49) | < 0.0001 | 79 | 0.9683 |
| Region | ||||||||||||
| Scandinavia | 1.60 (1.44, 1.77) | < 0.0001 | 46 | 0.5995 | 1.43 (1.25, 1.63) | < 0.0001 | 24 | 0.5773 | 1.35 (1.24, 1.47) | < 0.0001 | 52 | 0.9264 |
| United States | 1.56 (1.46, 1.66) | < 0.0001 | 139 | 0.9999 | 1.54 (1.34, 1.76) | < 0.0001 | 30 | 0.9991 | 1.27 (1.17, 1.39) | < 0.0001 | 68 | 0.9999 |
| UK, Canada, Australia, New Zealand | 1.52 (1.37, 1.70) | < 0.0001 | 32 | 0.9987 | 1.28 (1.04, 1.59) | 0.0229 | 8 | 0.9357 | 1.13 (0.91, 1.40) | 0.2643 | 8 | 0.9348 |
| East Europe | 1.86 (1.68, 2.06) | < 0.0001 | 35 | 0.0242 | 2.13 (1.77, 2.55) | < 0.0001 | 10 | 0.1376 | 1.59 (0.97, 2.62) | 0.0675 | 2 | 0.6112 |
| West Europe, Israel | 1.07 (0.96, 1.18) | 0.2129 | 35 | < 0.0001 | 1.39 (1.27, 1.53) | < 0.0001 | 44 | 0.5403 | 1.25 (1.10, 1.41) | 0.0005 | 32 | 0.4953 |
| China, Japan, Taiwan, Vietnam | 1.35 (0.95, 1.91) | 0.0969 | 9 | 0.9668 | 1.63 (1.10, 2.41) | 0.0150 | 3 | 0.0400 | 1.52 (1.24, 1.85) | 0.0001 | 13 | 0.2371 |
| Bangladesh, Brazil, Lebanon | 1.70 (1.30, 2.21) | 0.0001 | 31 | 0.9889 | … | … | 1 | … | 0.64 (0.36, 1.13) | 0.1213 | 3 | 0.0783 |
| Age | ||||||||||||
| 20 – 29.9 | 1.88 (1.51, 2.33) | < 0.0001 | 22 | 0.9960 | … | … | 0 | … | … | … | 0 | … |
| 30 – 39.9 | 2.16 (1.78, 2.61) | < 0.0001 | 22 | 0.9988 | 3.39 (2.31, 4.98) | < 0.0001 | 2 | 0.9142 | … | … | 1 | … |
| 40 – 49.9 | 1.84 (1.67, 2.03) | < 0.0001 | 43 | 0.7092 | 2.21 (1.61, 3.03) | < 0.0001 | 6 | 0.2111 | 1.55 (1.27, 1.90) | < 0.0001 | 13 | 0.0075 |
| 50 – 59.9 | 1.59 (1.47, 1.73) | < 0.0001 | 61 | 0.9848 | 1.98 (1.63, 2.41) | < 0.0001 | 10 | 0.4287 | 1.59 (1.34, 1.89) | < 0.0001 | 13 | 0.9733 |
| 60 – 69.9 | 1.61 (1.46, 1.77) | < 0.0001 | 55 | 0.2319 | 1.44 (1.26, 1.66) | < 0.0001 | 24 | 0.8945 | 1.36 (1.24, 1.50) | < 0.0001 | 44 | 0.9999 |
| 70 – 79.9 | 1.33 (1.18, 1.50) | < 0.0001 | 33 | 0.6953 | 1.33 (1.09, 1.62) | 0.0043 | 10 | 0.9370 | 1.17 (1.01, 1.36) | 0.0320 | 17 | 0.9939 |
| ≥ 80 | 1.20 (1.11, 1.29) | < 0.0001 | 90 | < 0.0001 | 1.39 (1.30, 1.50) | < 0.0001 | 68 | 0.9177 | 1.22 (1.14, 1.31) | < 0.0001 | 90 | 0.9919 |
| Baseline start year | ||||||||||||
| 1860 – 1939 | 0.63 (0.21, 1.92) | 0.4159 | 2 | 0.3876 | 1.39 (1.19, 1.62) | < 0.0001 | 16 | 0.8573 | … | … | 0 | … |
| 1940 – 1949 | 1.74 (1.56, 1.94) | < 0.0001 | 74 | 0.9999 | 1.68 (1.09, 2.59) | 0.0182 | 2 | 0.4332 | … | … | 0 | … |
| 1950 – 1959 | 1.75 (1.53, 2.01) | < 0.0001 | 27 | 0.9955 | 1.64 (1.38, 1.95) | < 0.0001 | 15 | 0.9585 | 1.63 (1.13, 2.37) | 0.0095 | 4 | 0.8219 |
| 1960 – 1969 | 1.32 (1.22, 1.43) | < 0.0001 | 66 | < 0.0001 | 1.34 (1.04, 1.72) | 0.0220 | 7 | 0.7537 | 1.21 (1.00, 1.45) | 0.0485 | 14 | 0.9724 |
| 1970 – 1979 | 1.47 (1.34, 1.61) | < 0.0001 | 71 | 0.9797 | 1.36 (1.20, 1.54) | < 0.0001 | 36 | 0.9941 | 1.22 (1.12, 1.34) | < 0.0001 | 62 | 0.9999 |
| 1980 – 1989 | 1.61 (1.45, 1.78) | < 0.0001 | 46 | 0.1023 | 1.41 (1.21, 1.66) | < 0.0001 | 17 | 0.9902 | 1.33 (1.22, 1.45) | < 0.0001 | 35 | 0.9988 |
| 1990 – 1999 | 1.44 (1.24, 1.69) | < 0.0001 | 35 | 0.9977 | 1.71 (1.49, 1.97) | < 0.0001 | 23 | 0.0006 | 1.42 (1.24, 1.62) | < 0.0001 | 36 | 0.1681 |
| 2000 – 2002 | 1.80 (1.28, 2.55) | 0.0008 | 6 | 0.8764 | 1.69 (1.26, 2.27) | 0.0005 | 4 | 0.5760 | … | … | 0 | … |
| Follow-up duration | ||||||||||||
| 6 months or less | 1.84 (1.61, 2.09) | < 0.0001 | 25 | 0.9676 | 0.96 (0.71, 1.30) | 0.7992 | 4 | 0.4967 | … | … | 0 | … |
| 1 year | 1.40 (1.30, 1.49) | < 0.0001 | 73 | <0.0001 | 3.02 (2.27, 4.01) | < 0.0001 | 4 | 0.8744 | … | … | 1 | … |
| 2 years | 1.70 (1.50, 1.91) | < 0.0001 | 32 | 0.9630 | 1.71 (1.38, 2.10) | < 0.0001 | 8 | 0.0559 | 1.45 (1.17, 1.79) | 0.0008 | 8 | 0.0080 |
| 3 years | 1.67 (1.51, 1.85) | < 0.0001 | 78 | 0.9999 | 1.72 (1.29, 2.28) | 0.0002 | 4 | 0.4696 | 2.16 (0.72, 6.46) | 0.1685 | 2 | 0.1439 |
| 4 years | 2.45 (1.28, 4.67) | 0.0066 | 2 | 0.5955 | 1.62 (1.26, 2.09) | 0.0002 | 5 | 0.6290 | 0.37 (0.09, 1.56) | 0.1765 | 3 | 0.8380 |
| 5 years | 1.30 (1.05, 1.61) | 0.0165 | 12 | 0.9981 | 1.43 (0.99, 2.06) | 0.0541 | 3 | 0.5493 | 1.16 (0.90, 1.51) | 0.2459 | 5 | 0.9310 |
| 6 years | … | … | 1 | … | 1.45 (1.24, 1.71) | < 0.0001 | 16 | 0.9083 | 1.25 (1.09, 1.43) | 0.0014 | 21 | 0.9960 |
| 7 years | 1.93 (1.23, 3.02) | 0.0042) | 7 | 0.9075 | … | … | 1 | … | 1.44 (1.17, 1.77) | 0.0006 | 13 | 0.3467 |
| 8 years | 1.67 (1.36, 2.07) | < 0.0001 | 31 | 0.9846 | … | … | 1 | … | 0.83 (0.55, 1.26) | 0.3916 | 4 | 0.0781 |
| 9 years | 0.95 (0.68, 1.33) | 0.7728 | 3 | 0.9375 | 1.31 (0.82, 2.08) | 0.2577 | 3 | 0.1159 | 1.29 (1.10, 1.52) | 0.0020 | 17 | 0.9999 |
| 10 years | 1.27 (0.86, 1.85) | 0.2266 | 8 | 0.9998 | 1.40 (1.25, 1.57) | < 0.0001 | 27 | 0.9796 | 1.24 (1.02, 1.51) | 0.0312 | 9 | 0.5542 |
| 11 years | 1.44 (1.08, 1.91) | 0.0121 | 8 | 0.9394 | 1.34 (1.05, 1.70) | 0.0166 | 13 | 0.9999 | 1.33 (1.03, 1.70) | 0.0270 | 17 | 0.9222 |
| 12 years | … | … | 0 | … | 1.37 (0.89, 2.10) | 0.1503 | 2 | 0.3414 | 1.32 (1.08, 1.61) | 0.0066 | 11 | 0.9915 |
| 13 years | 1.29 (0.78, 2.14) | 0.3155 | 2 | 0.8107 | 1.46 (0.98, 2.19) | 0.0631 | 3 | 0.6348 | 1.43 (1.02, 2.01) | 0.0356 | 4 | 0.6137 |
| 14 years | 1.32 (1.04, 1.67) | 0.0225 | 10 | 0.8015 | 1.28 (0.96, 1.72) | 0.0939 | 7 | 0.7138 | 1.85 (1.36, 2.53) | 0.0001 | 6 | 0.7085 |
| 15 years | … | … | 0 | … | 1.19 (0.71, 1.98) | 0.5067 | 2 | 0.4932 | 1.07 (0.89, 1.30) | 0.4697 | 15 | 0.9278 |
| 16-20 years | 1.57 (1.33, 1.86) | < 0.0001 | 18 | 0.0003 | 1.41 (0.91, 2.18) | 0.1279 | 3 | 0.5705 | 1.51 (1.26, 1.81) | < 0.0001 | 11 | 0.9597 |
| 21-25 years | 1.40 (0.80, 2.44) | 0.2405 | 2 | 0.8241 | 1.22 (0.94, 1.58) | 0.1427 | 5 | 0.9341 | 1.39 (1.19, 1.62) | < 0.0001 | 14 | 0.7103 |
| More than 25 years | 1.06 (0.68, 1.67) | 0.7888 | 6 | 0.8550 | 1.41 (1.11, 1.79) | 0.0042 | 10 | 0.7444 | 1.37 (1.04, 1.80) | 0.0240 | 6 | 0.6711 |
All meta-analyses calculated by maximum likelihood using a random effects model. Numbers reported are the mean hazard ratio (HR), 95% confidence interval (CI), number of hazard ratios included in the mean HR calculation (NHR), and the P-value from Cochran’s Q-test for data heterogeneity. Ellipses indicated when n ≤ 1 and meaningful mean HR could not be calculated.
The number and type of covariates varies between studies
Subgroup Meta-analyses and Meta-regression Analyses
In the interest of presenting conservative results, from this point forward the discussion of Table 3 will focus only on HRs adjusted for age and additional covariates. Table 3 shows that marital dissolution was associated with decreased longevity for both genders. However, in accordance with our hypothesis, the magnitude of the association was greater for men (HR, 1.37; 95% CI, 1.27-1.49; n = 79 HRs) than for women (HR, 1.22; 95% CI, 1.13-1.32; n = 75). Table 4 presents the results of three meta-regression analyses, the first model consisting of all first order effects, the second model adding three interaction terms, and the third consisting of the final parsimonious model. All three models confirm that the risk of death for men who lost their spouse was substantially higher than the risk for women.
Table 4.
Multivariate Meta-Regression Analyses Predicting the Magnitude of the Effect of Marital Dissolution on Mortality a
| Variable | Model 1: All Predictors Except Interaction Terms | Model 2: All Predictors Including Interaction Terms | Model 3: Parsimonious Model b |
|---|---|---|---|
| Constant | 2.46 (1.59, 3.80) [p<0.001] | 1.77 (1.15, 2.70) [p=0.009] | 1.67 (1.36, 2.04) [p<0.001] |
| Standard error estimated (0 = No; 1 = Yes) | 0.90 (0.83, 0.97) [p=0.010] | 0.90 (0.83, 0.97) [p=0.005] | 0.91 (0.86, 0.96) [p=0.001] |
| Death rate estimated (0 = No; 1 = Yes) | 1.03 (0.96, 1.10) [p=0.384] | 1.04 (0.97, 1.10) [p=0.283] | … |
| Publication Age (in 10 year increments) | 1.01 (0.98, 1.05) [p=0.485] | 1.02 (0.98, 1.06) [p=0.334] | … |
| Study age (in 10 year increments) | 1.00 (0.98, 1.02) [p=0.744] | 0.98 (0.93, 1.03) [p=0.410] | … |
| Study age * Study age | … | 1.00 (1.00, 1.00) [p=0.418] | … |
| Baseline length (years) | 1.00 (0.99, 1.00) [p=0.231] | 1.00 (0.99, 1.00) [p=0.359] | … |
| Years between baseline and start of follow-up | 1.00 (0.96, 1.04) [p=0.958] | 1.00 (0.96, 1.03) [p=0.883] | … |
| Follow-up duration (years) | 1.00 (0.99, 1.00) [p=0.646] | 1.00 (0.99, 1.01) [p=0.747] | … |
| Longitudinal study design (0 = No; 1 = Yes) | 1.02 (0.89, 1.17) [p=0.792] | 1.02 (0.90, 1.17) [p=0.724] | … |
| Stressed population (0 = No; 1 = Yes) | 0.86 (0.73, 1.00) [p=0.056] | 0.86 (0.74, 1.00) [p=0.057] | 0.86 (0.76, 0.97) [p=0.016] |
| Gender (Proportion of sample that is male; Range: 0-1) | 1.17 (1.11, 1.24) [p<0.001] | 2.41 (2.00, 2.90) [p<0.001] | 2.43 (2.02, 2.91) [p<0.001] |
| Mean age (in 10 year increments) | 0.88 (0.86, 0.90) [p<0.001] | 0.93 (0.91, 0.96) [p<0.001] | 0.94 (0.92, 0.96) [p<0.001] |
| Age range (in 10 year increments) | 0.98 (0.96, 1.00) [p=0.021] | 0.98 (0.96, 1.00) [p=0.011] | 0.98 (0.97, 1.00) [p=0.007] |
| Interactions | |||
| Gender * Follow-up duration | … | 1.00 (0.99, 1.01) [p=0.790] | … |
| Gender * Mean age | … | 0.88 (0.85, 0.91) [p<0.001] | 0.88 (0.85, 0.91) [p<0.001] |
| Controls (0 = No; 1 = Yes) | |||
| Gender | 0.93 (0.81, 1.08) [p=0.353] | 0.93 (0.82, 1.07) [p=0.323] | … |
| Age | 1.03 (0.96, 1.12) [p=0.388] | 1.03 (0.96, 1.10) [p=0.487] | … |
| Other demographics | 1.01 (0.91, 1.13) [p=0.802] | 1.02 (0.92, 1.13) [p=0.755] | … |
| SES | 0.96 (0.85, 1.08) [p=0.470] | 0.96 (0.86, 1.07) [p=0.439] | … |
| General health status | 0.90 (0.79, 1.03) [p=0.121] | 0.91 (0.80, 1.03) [p=0.125] | 0.89 (0.81, 0.97) [p=0.010] |
| Smoking/Other health behaviors | 0.96 (0.80, 1.16) [p=0.691] | 0.94 (0.79, 1.12) [p=0.517] | … |
| Chronic condition | 1.11 (0.93, 1.34) [p=0.255] | 1.11 (0.94, 1.32) [p=0.230] | … |
| Psychiatric characteristics | 1.08 (0.66, 1.75) [p=0.768] | 1.12 (0.70, 1.78) [p=0.644] | … |
| Social ties | 0.96 (0.86, 1.07) [p=0.495] | 0.97 (0.88, 1.07) [p=0.558] | … |
| Previous stress | 1.01 (0.90, 1.15) [p=0.819] | 1.02 (0.91, 1.14) [p=0.782] | … |
| Log of sample size | 1.02 (1.00, 1.04) [p=0.022] | 1.02 (1.01, 1.04) [p=0.006] | 1.02 (1.01, 1.04) [p<0.001] |
| Regions | |||
| Scandinavia | Reference | Reference | Reference |
| United States | 1.03 (0.89, 1.18) [p=0.705] | 1.03 (0.91, 1.18) [p=0.618] | 1.02 (0.95, 1.09) [p=0.657] |
| UK, Canada, Australia, New Zealand | 0.88 (0.79, 0.98) [p=0.020] | 0.88 (0.79, 0.97) [p=0.009] | 0.85 (0.78, 0.93) [p<0.001] |
| East Europe | 1.08 (0.95, 1.23) [p=0.221] | 1.06 (0.94, 1.19) [p=0.376] | 1.04 (0.96, 1.14) [p=0.328] |
| West Europe, Israel | 0.78 (0.71, 0.85) [p<0.001] | 0.78 (0.71, 0.85) [p<0.001] | 0.79 (0.74, 0.85) [p<0.001] |
| China, Japan, Taiwan, Vietnam | 0.96 (0.79, 1.16) [p=0.674] | 0.97 (0.80, 1.16) [p=0.704] | 1.01 (0.86, 1.18) [p=0.946] |
| Bangladesh, Brazil, Lebanon | 1.05 (0.76, 1.45) [p=0.764] | 1.13 (0.83, 1.53) [p=0.444] | 1.16 (0.87, 1.55) [p=0.308] |
| Number of divorces per 1,000 population | 1.00 (0.95, 1.05) [p=0.994] | 1.00 (0.95, 1.05) [p=0.982] | … |
| Subjective quality assessment (Range: 1-3) | 1.02 (0.95, 1.10) [p=0.576] | 1.02 (0.95, 1.10) [p=0.573] | … |
| Scale measure of study quality (Range: 0-10) | 0.98 (0.95, 1.01) [p=0.125] | 0.97 (0.95, 1.00) [p=0.074] | … |
| R2 | .4714 | .5474 | .5301 |
| Variance Component | .0471 [p<.001] | .0374 [p<.001] | .0386 [p<.001] |
All meta-regressions calculated by maximum likelihood using a random effects model (n=625). Number reported is the exponentiated regression coefficient (95% confidence interval) [p-value]. Ellipses indicate when a variable was not entered into a model.
Obtained using backwards elimination, p>.10 to exit.
An interesting result comes from comparing groups by average age at baseline. There are no HRs adjusted for age and for additional variables for the age groups of 20-29 and 30-39. However, the unadjusted and age adjusted mean HRs for these two age groups suggest that the risk of mortality following marital dissolution in these younger age groups is higher than it is in older age groups. Indeed, in accordance with our hypothesis, marital dissolution is associated with increased mortality in almost all age groups, but there is a decrease in the magnitude of the association at older ages. In the 40 and 50 age group, divorced and separated persons had a 55% higher risk of death than married persons (HR, 1.55; 95% CI, 1.27-1.90; n = 13). The risk was still high for those aged 50 to 59 years (HR, 1.59; 95% CI, 1.34-1.89; n=13), but then decreased substantially for those aged 60 to 69 (HR, 1.36; 95% CI, 1.24-1.50; n=44), 70 to 79 (HR, 1.17; 95% CI, 1.01-1.36; n=17), and 80 or older (HR, 1.22; 95% CI, 1.14-1.31; n=90). The results of the meta-regression analysis (Model 3 of Table 4) reflect this downward trend among the latter four age groups (a 6% decrease for each additional 10 years; p < .001).
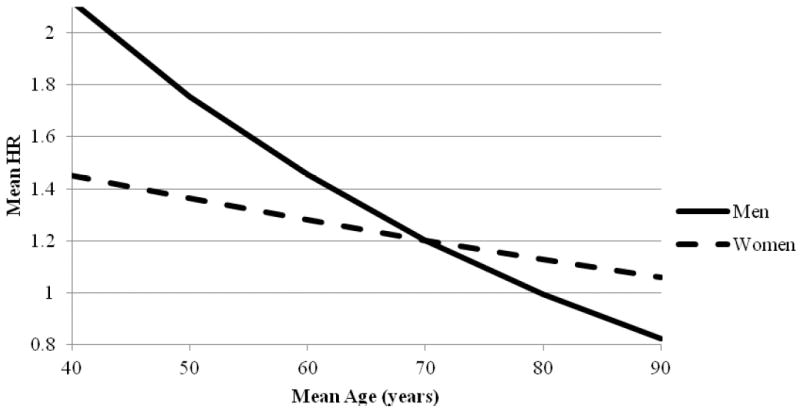
The impacts of gender and age on the magnitude of the HR are more complex than the meta-analyses can reveal. Models 2 (full model) and 3 (parsimonious model) of Table 4 both show a significant interaction effect between these two variables. In Model 3, the exponentiated regression coefficient for gender is 2.43 (95% CI, 2.02-2.91), 0.94 (95% CI, 0.92-0.96) for mean age, and 0.88 (95% CI, 0.85-0.91) for the interaction between gender and mean age. Taken together, these results tell us that the risk of death for men declines more rapidly with age than it does for women. By about 70 years of age, there is no longer a significant difference between men and women, with the mean HR for men falling below the mean HR for women at greater ages. However, by about 90 years of age there is little substantive difference remaining between persons who were divorced or separated and married persons. Figure 2 shows the gender-mean age interaction based on calculations from Model 3 of Table 4 (see Section 7 of Appendix for details).
Figure 2. Mean HR by Mean Age and Gender Based on Model 3 of Table 4.
The results reported in Table 3 show that there is no clear trend in HRs by follow-up duration. Model 2 of Table 4 confirms this pattern, as the exponentiated regression coefficients were not significant for follow-up duration (p = 0.7470) or for the gender-follow up interaction (p = 0.0790). The results in Table 3 show that marital dissolution was associated with substantially elevated mortality in studies conducted between 1950 and 1959 (HR, 1.62; CI, 1.18-2.22). The magnitude of the association declined in studies with a baseline year in subsequent decades. The mean HR was 1.21 (95% CI, 1.04-1.40) for studies with a baseline between 1960 and 1969, and 1.22 (95% CI, 1.14-1.31) for studies with a baseline between 1970 and 1979. However, beginning in 1980 the risk of mortality associated with marital dissolution began to increase again, with a mean HR of 1.35 (95% CI, 1.25-1.44) for studies with a baseline between 1980 and 1989 and to 1.42 (1.26-1.58) in studies with a baseline between 1990 and 1999. While these results suggest that the association between marital dissolution and mortality may be curvilinear across baseline years (i.e. the age of the study), the results from Model 2 of Table 4 show no significant linear (p = 0.4100) or curvilinear (p = 0.4180) relationship.
With only two exceptions, the magnitude of the association between marital dissolution and mortality did not differ between regions of the world. The lack of statistical significance for most regions in Model 3 of Table 4 indicates that the magnitude of the mean HR was approximately the same in Scandinavia (the reference group); in the United States (p = 0.6570); in the Eastern European nations (p = 0.3280); in China, Japan, Taiwan, and Vietnam (p = 0.9460); and in Bangladesh, Brazil, and Lebanon (p = 0.3080). The mean HR was 15% lower in the United Kingdom, Canada, Australia, and New Zealand (p < 0.0001) and 21% lower in the Western European nations and Israel (p < 0.0001) when compared to the mean HR in Scandinavia. The results from Model 2 of Table 4 show that the number of divorces per 1,000 persons in a given nation-year also did not predict HR magnitude (p = 0.9820).
Table 4 shows that other significant predictors of HR magnitude include the indicator for whether the study sample consisted of persons with pre-existing health or stress conditions (a 14% decrease in the mean HR if so; p=.0160), the age range of the study sample (a 2% decrease in the mean HR for each additional 10 years of age range; p = 0.0070), and the log of the sample size (p < 0.0001). Table 4 also shows that HRs in studies where the standard error was estimated were somewhat lower when compared with studies where it was not estimated (a 9% decrease; p = .0010).
Analysis of Data Heterogeneity
The between-groups Cochrane’s Q for the meta-analysis of all 625 HRs was statistically significant (p < 0.0001) and the I2 statistic was high ( I, = 89.8; 95% CI, 72.7-96.2), indicating that important moderating variables exist and supporting the decisions to use random effects models and conduct sub-group meta-analyses. Since the discussion of the meta-analyses focused on HRs adjusted for age and additional covariates, the corresponding heterogeneity test results were carefully examined. As shown in Table 3, the Q-tests for these sub-group meta-analyses were statistically significant for only two cases, the HRs from the 40-49.9 age group (p = 0.0075) and from the 2-year follow-up group (p = 0.0080). I2 tests for these subgroups indicate heterogeneity was high for the 40-49.9 age group (I2 = 55.7; 95% CI, 17.5-76.2) and the 2-year follow-up group (I2 = 63.2; 95% CI, 21.1-82.9). The results from these three sub-group meta-analyses should be treated conservatively. However, all remaining subgroup analysis Q-tests and I2 tests were non-significant, indicating that heterogeneity was adequately accounted for by the use of a random effects model.
Meta-regressions were also used to examine possible sources of heterogeneity in the data. The model fit statistics for Model 3 of Table 4 (R2 = 0.5301; p < 0.0001 for Cochrane’s Q of the model) indicate that this model captured a very substantial portion of the heterogeneity in the data. Nevertheless, the unexplained heterogeneity variance component for this and the other models shown in Table 4 remained highly significant (each p < 0.001), confirming the need to use a random effects model for all analyses.
Discussion
The results of the meta-analyses and meta-regressions show that the association between marital dissolution and mortality was not uniform across all subgroups and important moderators must be considered. In accordance with our hypothesis, among HRs adjusted for age and additional covariates, the risk of death for those who were divorced or separated was 30% higher than the risk among married persons. The association was greater for men (an increased risk of 37%) than for women (an increase in risk of only 22%). These findings both expand and revisit the analysis of Manzoli et al. (2007), who conducted a meta-analysis of marital status and mortality among the elderly (65 and older) using studies published between 1994 and 2005. While Manzoli et al. found a 16% increase in mortality for elderly people who experienced marital dissolution, the current study found a more substantial increase in the risk (17% to 36% increase in risk, depending on the specific age group) for the elderly and an even higher risk (almost 60% increase in risk) for younger age groups. Furthermore, while Manzoli et al. found no differences across genders, our study shows that at least in younger age groups divorced and separated men have a higher risk of mortality than divorced or separated women.
Manzoli et al. argued that the typology of interpersonal ties has changed over the years, reflecting the cultural and socio-economic modifications that occurred in rapidly evolving societies (See also Henrard, 1996). By including in their analysis only studies that were published after 1994, Manzoli et al. were able to use only those studies conducted using longitudinal data but they could not evaluate the effect of these social trends on the magnitude of the risk. Our study, on the other hand, included study findings from earlier periods and found that the risk of mortality among divorced and separated persons has been relatively stable over time. Model 2 of Table 4 shows that the mean HRs did not significantly decline (p = 0.4100) with each additional 10 years that passed since baseline data collection.
Consistent with our theoretical suppositions, we found an interaction effect between gender and mean age. The mean HRs for both men and women declined as mean age increased, but more so for men than for women. Figure 2 shows a mean HR of 2.12 among samples of men with a mean age of 40 years. At the same mean age, the mean HR among women was 1.45. Among samples with a mean age of 70, the mean HR is 1.20 for both men and women. Among samples with a mean age of 90, the mean HR is not significantly different from 1.00 for women and is below 1.00 for men (calculated HR = 0.82). Some caution must be exercised when interpreting this finding. When the underlying death rates are very high in both the case and control groups (as is the case at older ages) ratio statistics such as the HR often lack statistical power to detect group differences. Given the magnitude of the age-effect, however, it is still likely that the observed age effects are substantively meaningful rather than merely a statistical artifact. Therefore, possible explanations for this finding need to be considered.
The pronounced gender difference in hazard ratios in the younger age groups may seem somewhat surprising given what we know about the disproportionate economic consequences of marital dissolution for men and women. A large body of research has established that women experience much larger reductions in income and standard of living following divorce than do men (e.g. Holden & Smock, 1991; McManus & DiPrete, 2001; Smock, 1994; Smock et al., 1999). Therefore one could have expected women’s health, and their subsequent mortality risk, to be more adversely affected. However, consistent with previous research findings, our findings show that the mean mortality risk for middle-aged men was substantively higher than the risk for women.
One plausible explanation for the findings presented in Figure 2 might be that men experience a more dramatic decline in supportive social ties following divorce while women are better able to maintain their ties. Previous research has shown that in married couples women perform the majority of the work for maintaining parent-child relationships (Kaufman & Uhlenberg, 1998; Lye, 1996; Lye et al., 1995). Furthermore, in a recent study Kalmijn (2007) found that, in comparison to women, men experienced greater declines in social support from their children following marital dissolution. This effect was especially strong if the marital dissolution occurred at an early stage. This finding may explain the interaction effect in Figure 2, where the difference in mean hazard ratios between men and women was much more pronounced at middle-age than at older ages. Social support appears to be a possible moderating factor in the gender differences in mortality following marital dissolution, but our data do not allow for a direct test of this hypothesis.
Another possible explanation for the findings presented in Figure 2 is that the deleterious effects of marital dissolution wane over time. Most marital dissolutions occur at a younger age, when the familial cell is relatively vulnerable (Fergusson, Horwood, & Shannon, 1984; Thornton & Rodgers, 1987). The relative instability of non-elderly couples may be the result of the pressures associated with child rearing, changes in the nuclear family structure when children leave the household, and the greater availability of alternate partners. One may thus argue that the lower excess risk of mortality following marital dissolution at older ages may simply reflect the effects of remarriage or habituation. According to this logic individuals who have lived without a partner for a long time may have adjusted to their status and found ways to compensate for the loss of social and economic support. This habituation hypothesis, however, is refuted by lack of significance for the interaction between gender and follow-up duration. In contrast to our hypothesis, the adverse effects of marital dissolution did not diminish over time for either men or women.
Finally, the analysis of differences in the risk of mortality by region failed to uncover differences in the effects of marital dissolution between most of the regions of the developed world. Mean HRs were approximately equal (ranging from 1.13 to 1.59; see Table 3) in Scandinavia; the United States; the United Kingdom, Canada, Australia, and New Zealand; East Europe; West Europe and Israel; and in China, Japan, Taiwan, and Vietnam. The magnitude of the effect only differed for the grouping of Bangladesh, Brazil, and Lebanon, though this apparent difference is not significant once other possible confounders are taken into consideration (see Table 4). Though the results from Table 4 show a significant reduction in the mean HR for the United Kingdom, Canada, Australia, and New Zealand and for West Europe and Israel, these results should be treated with caution. The lack of significance associated with the number of divorces per 1,000 people suggests that broad cultural differences are not strong predictors of differences in the relative mortality rate associated with marital dissolution.
Limitations
A major limitation of our study is one that is shared by many meta-analyses: reporting bias, or more specifically the non-reporting of non-significant findings, also known as the file-drawer effect (Berman & Parker, 2002; Egger & Davey-Smith, 1998). This tendency may lead to an over estimation of the mean HRs. Therefore, one should be especially careful in interpreting mean HRs which are relatively close to 1, even when these are significant (as is the case with some of the results in the current meta-analysis). A funnel plot of the log HRs against sample size appears somewhat asymmetric around the mean HR, suggesting the possibility of publication bias (Figure 3). Using Egger’s test (Egger & Davey-Smith, 1998), there was significant evidence of publication bias (p < 0.001). Using Peters et al.’s test (Moreno et al., 2009; Peters et al., 2006) there was also evidence of publication bias among the unadjusted HRs (p < 0.001) and among HRs adjusted for age and additional covariates (p = 0.006), but not among HRs adjusted for age only (p = 0.274). The significant negative regression coefficients for the inverse of the sample size indicate that small studies with large HRs are missing from the analysis. Due to ongoing concerns with formal methods to correct for publication bias, such as the “trim and fill” method (Terrin, Schmid, Lau, & Olkin, 2003), we have not performed additional analyses using adjusted data. However, the nature of the bias is such that our results would tend to underestimate the mean HR rather than overestimate it. The direction of the regression coefficients indicates that it is unlikely that publication bias caused an overestimation of the risk associated with marital dissolution.
Figure 3. Funnel plot of hazard ratios (logged) versus sample size: hazard ratios statistically adjusted for age and additional covariates.
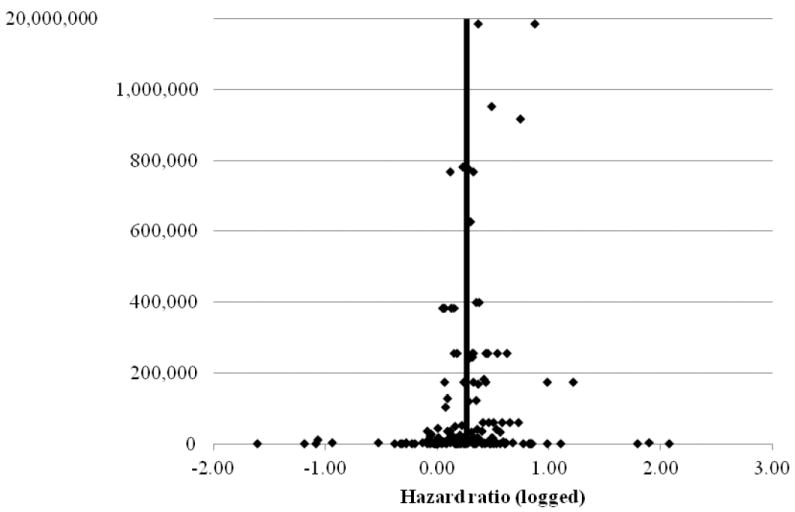
Vertical line denotes the mean hazard ratio (logged) of 0.2619. Scale changes for samples ≥ 1,000,000 persons to provide greater resolution.
A second limitation of the present study lies in the incomplete nature of the possible confounding and moderating variables included in the analysis. While the heterogeneity test results support the conclusion that a substantial portion of data variability has been accounted for, the continued need for random effects models indicates that important confounding and/or moderating factors were excluded from the models. A major goal of this research was to evaluate such factors, but additional research is clearly needed to further identify the sources of the data heterogeneity we observed.
A third limitation stems from the nature of the data. Most of the research on marital dissolution and mortality was conducted in the developed world. Relatively few publications used data from East Asia, the Middle East, and South America, and none used data from Africa. This limitation has two important consequences. First, the sample sizes in the developing world are small and any conclusions about the difference between the developed and the developing world should be made with caution. Second, since most of the results come from the developed countries they should not be extrapolated to populations in developing countries.
Conclusion
In conclusion, this study shows that marital dissolution is associated with a substantially increased risk of death among broad segments of the population. However, important moderators of this association – such as gender, age, and general health status – must be carefully considered in order to better understand this association. Future research should focus on understanding the health, socio-economic and behavioral factors through which this association is manifested, especially for younger men and women. Further research in developing countries is also needed to determine the magnitude of the risk. Since the majority of the world’s population resides in developing nations, much work remains to be done.
Supplementary Material
Research Highlights.
The risk of early mortality among the divorced and separated is 30% higher than the risk among the married
Divorced men are more at risk than divorced women, but the differences between men and women decrease with age
The harmful effects of marital dissolution are most pronounced during the first few years following the dissolution.
Acknowledgments
The authors are grateful for the support provided by Grant HL-76857 from the National Institutes of Health. The funding source had no involvement in the collection, analysis and interpretation of the data, in the writing of the report, and in the decision to submit the paper for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Eran Shor, Department of Sociology, McGill University, Montreal.
David J. Roelfs, Department of Sociology, University of Louisville, Kentucky.
Paul Bugyi, Department of Sociology, Stony Brook University, New York.
Joseph E. Schwartz, Department of Psychiatry and Behavioral Science, Stony Brook University, New York.
References
- Ahs AMH, Westerling R. Mortality in Relation to Employment Status during Different Levels of Unemployment. Scandinavian Journal of Public Health. 2006;34(2):159–167. doi: 10.1080/14034940510032374. [DOI] [PubMed] [Google Scholar]
- Alavinia SM, Burdorf A. Unemployment and Retirement and Ill-Health: A Cross-Sectional Analysis Across European Countries. International Archives of Occupational and Environmental Health. 2008;82(1):39–45. doi: 10.1007/s00420-008-0304-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amato PR, Rogers SJ. A Longitudinal Study of Marital Problems and Subsequent Divorce. Journal of Marriage and the Family. 1987;59:612–624. [Google Scholar]
- Artnik B, Vidmar G, Javornik J, Laaser U. Premature Mortality in Slovenia in Relation to Selected Biological, Socioeconomic, and Geographical Determinants. Croatian Medical Journal. 2006;47(1):103–113. [PMC free article] [PubMed] [Google Scholar]
- Bagiella E, Hong V, Sloan RP. Religious Attendance as a Predictor of Survival in the EPESE Cohorts. International Journal of Epidemiology. 2005;34(2):443–451. doi: 10.1093/ije/dyh396. [DOI] [PubMed] [Google Scholar]
- Bambra C, Eikemo T. Welfare State Regimes, Unemployment and Health: A Comparative Study of the Relationship Between Unemployment and Self-Reported Health in 23 European Countries. Journal of Epidemiology and Community Health. 2009;63(2):92–98. doi: 10.1136/jech.2008.077354. [DOI] [PubMed] [Google Scholar]
- Ben-Shlomo Y, Smith GD, Shipley M, Marmot MG. Magnitude and Causes of Mortality Differences between Married and Unmarried Men. Journal of Epidemiology and Community Health. 1993;47(3):200–205. doi: 10.1136/jech.47.3.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkman LF. The Relationship of Social Networks and Social Support to Morbidity and Mortality. In: Cohen S, Syme SL, editors. Social Support and Health. New York: Academic Press; 1985. pp. 240–259. [Google Scholar]
- Berkson J. Mortality and Marital Status: Reflections on the Derivation of Etiology from Statistics. American Journal of Epidemiology. 1962;52(8):1318–1329. doi: 10.2105/ajph.52.8.1318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berman NG, Parker RA. Meta-Analysis: Neither Quick nor Easy. BMC Medical Research Methodology. 2002;2:10–18. doi: 10.1186/1471-2288-2-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berntsen KN. Trends in total and cause-specific mortality by marital status among elderly Norwegian men and women. BMC Public Health. 2011;11 doi: 10.1186/1471-2458-11-537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blazer DG. Social Support and Mortality in an Elderly Community Population. American Journal of Epidemiology. 1982;115(5):684–694. doi: 10.1093/oxfordjournals.aje.a113351. [DOI] [PubMed] [Google Scholar]
- Booth A, Amaro PR. Divorce and Psychological Stress. Journal of Health and Social Behavior. 1991;32:396–407. [PubMed] [Google Scholar]
- Breeze E, Sloggett A, Fletcher A. Socioeconomic and Demographic Predictors of Mortality and Institutional Residence among Middle Aged and Older People: Results from the Longitudinal Study. Journal of Epidemiology and Community Health. 1999;53(12):765–774. doi: 10.1136/jech.53.12.765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brockmann H, Klein T. Family Biography and Mortality in East and West Germany. Zeitschrift Fur Gerontologie Und Geriatrie. 2002;35(5):430–440. doi: 10.1007/s00391-002-0123-4. [DOI] [PubMed] [Google Scholar]
- Brockmann H, Klein T. Love and Death in Germany: The Marital Biography and its Effect on Mortality. Journal of Marriage and the Family. 2004;66(3):567–581. [Google Scholar]
- Burgoa M, Regidor E, Rodriguez C, Gutierrez-Fisac JL. Mortality by Cause of Death and Marital Status in Spain. European Journal of Public Health. 1998;8(1):37–42. [Google Scholar]
- Cherlin AJ, Chase-Landsdale PL, McRae C. Effects of Parental Divorce on Mental Health Throughout the Life Course. American Sociological Review. 1998;63:239–249. [Google Scholar]
- Cheung YB. Marital Status and Mortality in British Women: A Longitudinal Study. International Journal of Epidemiology. 2000;29(1):93–99. doi: 10.1093/ije/29.1.93. [DOI] [PubMed] [Google Scholar]
- Choi H, Marks NF. Socioeconomic Status, Marital Status Continuity and Change, Marital Conflict, and Mortality. Journal of Aging and Health. 2011;23(4):714–742. doi: 10.1177/0898264310393339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Comstock GW, Tonascia JA. Education and Mortality in Washington County, Maryland. Journal of Health and Social Behavior. 1977 Mar;18:54–61. [PubMed] [Google Scholar]
- Cornell LL. Intergenerational Relationships, Social Support, and Mortality. Social Forces. 1992;71(1):53–62. [Google Scholar]
- Costa G, Segnan N. Unemployment and Mortality. British Medical Journal. 1987 Jun;294:1550–1551. doi: 10.1136/bmj.294.6586.1550-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doblhammer G. Reproductive History and Mortality Later in Life: A Comparative Study of England and Wales and Austria. Population Studies - A Journal of Demography. 2000;54(2):169–176. doi: 10.1080/713779087. [DOI] [PubMed] [Google Scholar]
- Duncan GJ, Hoffman SD. A Reconsideration of the Economic Consequences of Marital Dissolution. Demography. 1985;22(4):485–497. [PubMed] [Google Scholar]
- Dupre ME, Beck AN, Meadows SO. Marital Trajectories and Mortality Among US Adults. American Journal of Epidemiology. 2009;170(5):546–555. doi: 10.1093/aje/kwp194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durkheim E. Suicide. Glencoe: IL: Free Press; 1951 [1897]. [Google Scholar]
- Dzurova D. Mortality Differentials in the Czech Republic during the Post-1989 Socio-political Transformation. Health and Place. 2000;6(4):351–362. doi: 10.1016/s1353-8292(00)00016-2. [DOI] [PubMed] [Google Scholar]
- Ebrahim S, Wannamethee G, McCallum A, Walker M, Shaper AG. Marital Status, Change in Marital Status, and Mortality in Middle-aged British Men. American Journal of Epidemiology. 1995;142(8):834–842. doi: 10.1093/oxfordjournals.aje.a117723. [DOI] [PubMed] [Google Scholar]
- Egger M, Davey-Smith G. Meta-analysis: Bias in Location and Selection of Studies. British Medical Journal. 1998;316:61–66. doi: 10.1136/bmj.316.7124.61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ensel WM, Lin N. Age, the Stress Process, and Physical Disease. Journal of Aging and Health. 2000;12(2):139–168. doi: 10.1177/089826430001200201. [DOI] [PubMed] [Google Scholar]
- Ensel WM, Peek KM, Lin N, Lai G. Stress in the Life Course: A Life History Approach. Journal of Aging and Health. 1996;8(3):389–416. doi: 10.1177/089826439600800305. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Shannon FT. A Proportional Hazards Model of Family Breakdown. Journal of Marriage and Family. 1984;46:539–549. [Google Scholar]
- Glick PC, Lin SL. Remarriage After Divorce: Recent Changes and Demographic Variations. Sociological Perspectives. 1987;30(2):162–179. [PubMed] [Google Scholar]
- Goldman N, Hu YR. Excess Mortality among the Unmarried: A Case Study of Japan. Social Science & Medicine. 1993;36(4):533–546. doi: 10.1016/0277-9536(93)90414-y. [DOI] [PubMed] [Google Scholar]
- Goldman N, Korenman S, Weinstein R. Marital Status and Health among the Elderly. Social Science & Medicine. 1995;40(12):1717–1730. doi: 10.1016/0277-9536(94)00281-w. [DOI] [PubMed] [Google Scholar]
- Goodwin JS, Hunt WC, Key CR, Samet JM. The Effect of Marital Status on Stage, Treatment, and Survival of Cancer Patients. Journal of the American Medical Association. 1987;258(21):3125–3130. [PubMed] [Google Scholar]
- Gottman JM, Levenson RM. Marital Processes Predictive of Later Dissolution: Behavior, Phsiology, and Health. Journal of Personality and Social Psychology. 1992;63(2):221–223. doi: 10.1037//0022-3514.63.2.221. [DOI] [PubMed] [Google Scholar]
- Gove WR. Sex, Marital Status, and Mortality. American Journal of Sociology. 1973;79(1):45–67. doi: 10.1086/225505. [DOI] [PubMed] [Google Scholar]
- Granlund D, Chuc NT, Phuc HD, Lindholm L. Inequality in mortality in Vietnam during a period of rapid transition. Social Science & Medicine. 2010;70(2):232–239. doi: 10.1016/j.socscimed.2009.10.019. [DOI] [PubMed] [Google Scholar]
- Grundy E, Kravdal O. Reproductive History and Mortality in Late Middle Age among Norwegian Men and Women. American Journal of Epidemiology. 2008;167(3):271–279. doi: 10.1093/aje/kwm295. [DOI] [PubMed] [Google Scholar]
- Grundy EMD, Tomassini C. Marital history, health and mortality among older men and women in England and Wales. BMC Public Health. 2010;10 doi: 10.1186/1471-2458-10-554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hajdu P, McKee M, Bojan F. Changes in Premature Mortality Differentials by Marital Status in Hungary and in England and Wales. European Journal of Public Health. 1995;5(4):259–264. [Google Scholar]
- Hammarstrom A. Health Consequences of Youth Unemployment: Review from a Gender Perspective. Social Science and Medicine. 1994;38(5):699–709. doi: 10.1016/0277-9536(94)90460-x. [DOI] [PubMed] [Google Scholar]
- Hank K. Childbearing history, later-life health, and mortality in Germany. Population Studies-a Journal of Demography. 2010;64(3):275–291. doi: 10.1080/00324728.2010.506243. [DOI] [PubMed] [Google Scholar]
- Hansen HT. Unemployment and Marital Dissolution. European Sociological Review. 2005;21(2):135–148. [Google Scholar]
- Hayward MD, Gorman BK. The Long Arm of Childhood: The Influence of Early-life Social Conditions on Men’s Mortality. Demography. 2004;41(1):87–107. doi: 10.1353/dem.2004.0005. [DOI] [PubMed] [Google Scholar]
- Helweg-Larsen M, Kjoller M, Thoning H. Do Age and Social Relations Moderate the Relationship between Self-rated Health and Mortality among Adult Danes? Social Science & Medicine. 2003;57(7):1237–1247. doi: 10.1016/s0277-9536(02)00504-x. [DOI] [PubMed] [Google Scholar]
- Hemstrom O. Is Marriage Dissolution Linked to Differences in Mortality Risks for Men and Women? Journal of Marriage and the Family. 1996;58(2):366–378. [Google Scholar]
- Henrard JC. Cultural Problems of Aging Especially Regarding Gender and Intergenerational Equity. Social Science & Medicine. 1996;43:667–680. doi: 10.1016/0277-9536(96)00113-x. [DOI] [PubMed] [Google Scholar]
- Henretta JC. Early Childbearing, Marital Status, and Women’s Health and Mortality after Age 50. Journal of Health & Social Behavior. 2007;48(3):254–266. doi: 10.1177/002214650704800304. [DOI] [PubMed] [Google Scholar]
- Henretta JC. Lifetime Marital History and Mortality After Age 50. Journal of Aging and Health. 2010;22(8):1198–1212. doi: 10.1177/0898264310374354. [DOI] [PubMed] [Google Scholar]
- Holden KC, Smock PJ. The Economic Costs of Marital Dissolution: Why Do Women Bear a Disproportionate Cost? Annual Review of Sociology. 1991;17:51–78. doi: 10.1146/annurev.so.17.080191.000411. [DOI] [PubMed] [Google Scholar]
- Horwitz O, Weber J. Marital Status and Mortality. I. Sygeplejersken. 1974a;74(10):10–14. [PubMed] [Google Scholar]
- Horwitz O, Weber J. Marital Status and Mortality. II. Sygeplejersken. 1974b;74(11):20–25. [PubMed] [Google Scholar]
- Huedo-Medina TB, Sanchez-Meca J, Marin-Martinez F. Assessing Heterogeneity in Meta-analysis: Q Statistic or I2 Index? Psychological Methods. 2006;11(2):193–206. doi: 10.1037/1082-989X.11.2.193. [DOI] [PubMed] [Google Scholar]
- Hughes ME, Waite LJ. Marital Biography and Health at Mid-Life. Journal of Health and Social Behavior. 2009;50(3):344–358. doi: 10.1177/002214650905000307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurt LS, Ronsmans C, Saha S. Effects of Education and Other Socioeconomic Factors on Middle Age Mortality in Rural Bangladesh. Journal of Epidemiology and Community Health. 2004;58:315–320. doi: 10.1136/jech.2003.007351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ikeda A, Iso H, Toyoshima H, Fujino Y, Mizoue T, Yoshimura T, et al. Marital Status and Mortality among Japanese Men and Women: The Japan Collaborative Cohort Study. BMC Public Health. 2007;7:73. doi: 10.1186/1471-2458-7-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iribarren C, Jacobs DR, Kiefe CI, Lewis CE, Matthews KA, Roseman JM, et al. Causes and Demographic, Medical, Lifestyle and Psychosocial Predictors of Premature Mortality: The CARDIA Study. Social Science & Medicine. 2005;60(3):471–482. doi: 10.1016/j.socscimed.2004.06.007. [DOI] [PubMed] [Google Scholar]
- ISI Web of Knowledge. Journal Citation Reports. 2009 http://wokinfo.com/products_tools/analytical/jcr/
- Iversen L, Andersen O, Andersen PK, Christoffersen K, Keiding N. Unemployment and Mortality in Denmark, 1970-80. British Medical Journal. 1987;295(6603):879–884. doi: 10.1136/bmj.295.6603.879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwasaki M, Otani T, Sunaga R, Miyazaki H, Xiao L, Wang N, et al. Social Networks and Mortality Based on the Komo-Ise Cohort Study in Japan. International Journal of Epidemiology. 2002;31(6):1208–1218. doi: 10.1093/ije/31.6.1208. [DOI] [PubMed] [Google Scholar]
- Janlert U. Unemployment as a Disease and Diseases of the Unemployed. Scandinavian Journal of Work and Environmental Health. 1997;23(Supplement 3):79–83. [PubMed] [Google Scholar]
- Jenkinson CM, Madeley RJ, Mitchell JRA, Turner ID. The Influence of Psychosocial Factors on Survival after Myocardial Infarction. Public Health. 1993;107(5):305–317. doi: 10.1016/s0033-3506(05)80122-2. [DOI] [PubMed] [Google Scholar]
- Jin RL, Shah CP, Svoboda TJ. The Impact of Unemployment on Health: A Review of the Evidence. Canadian Medical Association Journal. 1995;153(5):529–540. [PMC free article] [PubMed] [Google Scholar]
- Johansen C, Schou G, Soll-Johanning H, Mellemgaard A, Lynge E. Influence of Marital Status on Survival from Colon and Rectal Cancer in Denmark. British Journal of Cancer. 1996;74(6):985–988. doi: 10.1038/bjc.1996.470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson NJ, Backlund E, Sorlie PD, Loveless CA. Marital Status and Mortality: The National Longitudinal Mortality Study. Annals of Epidemiology. 2000;10(4):224–238. doi: 10.1016/s1047-2797(99)00052-6. [DOI] [PubMed] [Google Scholar]
- Joung IMA, Glerum JJ, van Poppel JWPF, Mackenbach JP. The Contribution of Specific Causes of Death to Mortality Differences by Marital Status in the Netherlands. European Journal of Public Health. 1996;6(2):142–149. [Google Scholar]
- Kalediene R, Petrauskiene J, Starkuviene S. Inequalities in Mortality by Marital Status during Socio-economic Transition in Lithuania. Public Health. 2007 May;121:385–392. doi: 10.1016/j.puhe.2006.09.026. [DOI] [PubMed] [Google Scholar]
- Kalmijn M. Gender Differences in the Effects of Divorce, Widowhood and Remarriage on Intergenerational Support: Does Marriage Protect Fathers? Social Forces. 2007;85(3):1079–1104. [Google Scholar]
- Kaplan RM, Kronick RG. Marital Status and Longevity in the United States Population. Journal of Epidemiology and Community Health. 2006;60(9):760–765. doi: 10.1136/jech.2005.037606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman G, Uhlenberg P. Effects of Life Course Transitions on the Quality of Relationships Between Adult Children and their Parents. Journal of Marriage and Family. 1998;60:924–938. [Google Scholar]
- Keller AZ. Survivorship with Mouth and Pharynx Cancer and their Association with Cirrhosis of the Liver, Marital Status, and Residence. American Journal of Public Health Nations Health. 1969;59(7):1139–1153. doi: 10.2105/ajph.59.7.1139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Essex M. Marital Status and Depression: The Importance of Coping Resources. Social Forces. 1982;61(2):484–507. [Google Scholar]
- Kohler I, Kohler HP. The Effect of Marriage on Mortality: Selection or Protection? Evidence from Danish Twins using Fixed-Effect Survival Models. Unpublished. [Google Scholar]
- Kohler IV, Preston SH. Ethnic and religious differentials in Bulgarian mortality, 1993-98. Population Studies-a Journal of Demography. 2011;65(1):91–113. doi: 10.1080/00324728.2010.535554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kolip P. The Association between Gender, Family Status and Mortality. Journal of Public Health. 2005 Nov;13:309–312. [Google Scholar]
- Kraus A, Lilienfeld A. Some Epidemiological Aspects of the High Mortality Rate in the Young Widowed Group. Journal of Chronic Diseases. 1959;10(3):207–217. doi: 10.1016/0021-9681(59)90003-7. [DOI] [PubMed] [Google Scholar]
- Kravdal O. Children, Family and Cancer Survival in Norway. International Journal of Cancer. 2003;105(2):261–266. doi: 10.1002/ijc.11071. [DOI] [PubMed] [Google Scholar]
- Kravdal O. A Fixed-effects Multilevel Analysis of how Community Family Structure Affects Individual Mortality in Norway. Demography. 2007;44(3):519–537. doi: 10.1353/dem.2007.0029. [DOI] [PubMed] [Google Scholar]
- Kroenke CH, Kubzansky LD, Schernhammer ES, Holmes MD, Kawachi I. Social Networks, Social Support, and Survival after Breast Cancer Diagnosis. Journal of Clinical Oncology. 2006;24(7):1105–1111. doi: 10.1200/JCO.2005.04.2846. [DOI] [PubMed] [Google Scholar]
- Kumle M, Lund E. Patterns of Childbearing and Mortality in Norwegian Women. A 20-year Follow-up of Women Aged 40-96 in the 1970 Norwegian Census. In: Robine J-M, Kirkwood TBL, Allard M, editors. Sex and Longevity: Sexuality, Gender, Reproduction, Parenthood. Berlin: Springer; 2000. pp. 117–128. [Google Scholar]
- Laaksonen M, Tarkiainen L, Martikainen P. Housing wealth and mortality: A register linkage study of the Finnish population. Social Science & Medicine. 2009;69(5):754–760. doi: 10.1016/j.socscimed.2009.06.035. [DOI] [PubMed] [Google Scholar]
- Lillard LA, Panis CWA. Marital Status and Mortality: The Role of Health. Demography. 1996;33(3):313–327. [PubMed] [Google Scholar]
- Lillard LA, Waite LJ. Til Death Do Us Part - Marital Disruption and Mortality. American Journal of Sociology. 1995;100(5):1131–1156. MANUSCRIPT. [Google Scholar]
- Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: Sage; 2001. [Google Scholar]
- Litwak E, Messeri P, Wolfe S, Gorman S, Silverstein M, Guilarte M. Organizational Theory, Social Supports, and Mortality-Rates - a Theoretical Convergence. American Sociological Review. 1989;54(1):49–66. [Google Scholar]
- Liu H. Till Death Do Us Part: Marital Status and US Mortality Trends, 1986-2000. Journal of Marriage and Family. 2009;71(5):1158–1173. [Google Scholar]
- Liu LJ, Sullivan DH. Relationship between Social Demographic Factors and Survival Within One Year of Hospital Discharge in a Cohort of Elderly Male Patients. Journal of Epidemiology. 2003;13(4):203–210. doi: 10.2188/jea.13.203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lye DN. Adult Child-Parent Relationships. Annual Review of Sociology. 1996;22:79. [Google Scholar]
- Lye DN, Klepinger DH, Hyle PD, Nelson A. Childhood Living Arrangements and Adult Children’s Relations with their Parents. Demography. 1995;32:261–280. [PubMed] [Google Scholar]
- Makuc DM, Feldman JJ, Kleinman JC, Pierre MBJ. Sociodemographic Differentials in Mortality. In: Cornoni-Huntley J, Huntley RR, Feldman JJ, editors. Health Status and Well-being of the Elderly: National Health and Nutrition Examination Survey-I Epidemiologic Follow-up Study. New York: Oxford University Press; 1990. pp. 155–171. [Google Scholar]
- Malyutina S, Bobak M, Simonova G, Gafarov V, Nikitin Y, Marmot M. Education, Marital Status, and Total and Cardiovascular Mortality in Novosibirsk, Russia: A Prospective Cohort Study. Annals of Epidemiology. 2004;14(4):244–249. doi: 10.1016/S1047-2797(03)00133-9. [DOI] [PubMed] [Google Scholar]
- Manor O, Eisenbach Z, Israeli A, Friedlander Y. Mortality Differentials among Women: The Israel Longitudinal Mortality Study. Social Science & Medicine. 2000;51(8):1175–1188. doi: 10.1016/s0277-9536(00)00024-1. [DOI] [PubMed] [Google Scholar]
- Manor O, Eisenbach Z, Peritz E, Friedlander Y. Mortality Differentials among Israeli Men. American Journal of Public Health. 1999;89(12):1807–1813. doi: 10.2105/ajph.89.12.1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manzoli L, Villari P, Pirone GM, Boccia A. Marital Status and Mortality in the Elderly: A Systematic Review and Meta-Analysis. Social Science and Medicine. 2007;64(1):77–94. doi: 10.1016/j.socscimed.2006.08.031. [DOI] [PubMed] [Google Scholar]
- Martelin T. Socio-demographic Differentials in Mortality at Older Ages in Finland. In: Caselli G, Lopez AD, editors. Health and Mortality among Elderly Population. New York: Clarendon Press; 1996. pp. 112–134. [Google Scholar]
- Martelin T, Koskinen S, Valkonen T. Sociodemographic Mortality Differences among the Oldest Old in Finland. Journals of Gerontology Series B-Psychological Sciences and Social Sciences. 1998;53(2):S83–S90. doi: 10.1093/geronb/53b.2.s83. [DOI] [PubMed] [Google Scholar]
- Martikainen PT. Unemployment and Mortality among Finnish Men 1981-85. British Medical Journal. 1990;301(6749):407–411. doi: 10.1136/bmj.301.6749.407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martikainen PT. Womens Employment, Marriage, Motherhood and Mortality - a Test of the Multiple Role and Role Accumulation Hypotheses. Social Science and Medicine. 1995;40(2):199–212. doi: 10.1016/0277-9536(94)e0065-z. [DOI] [PubMed] [Google Scholar]
- Martikainen PT, Martelin T, Nihtila E, Majamaa K, Koskinen S. Differences in Mortality by Marital Status in Finland from 1976 to 2000: Analyses of Changes in Marital-status Distribution, Socio-demographic and Household Composition, and Cause of Death. Population Studies - A Journal of Demography. 2005;59(1):99–115. doi: 10.1080/0032472052000332737. [DOI] [PubMed] [Google Scholar]
- Mastekaasa A. Psychological Well-Being and Marital Dissolution. Journal of Family Issues. 1994;15(2):208–228. [Google Scholar]
- Matthews KA, Gump BB. Chronic Work Stress and Marital Dissolution Increase Risk of Posttrial Mortality in Men from the Multiple Risk Factor Intervention Trial. Archives of Internal Medicine. 2002;162(3):309–315. doi: 10.1001/archinte.162.3.309. [DOI] [PubMed] [Google Scholar]
- McManus PA, DiPrete TA. Losers and Winners: The Financial Consequences of Separation and Divorce for Men. American Sociological Review. 2001;66:246–268. [Google Scholar]
- Mellstrom D, Nilsson A, Oden A, Rundgren A, Svanborg A. Mortality among the Widowed in Sweden. Scandinavian Journal of Social Medicine. 1982;10(2):33–41. doi: 10.1177/140349488201000201. [DOI] [PubMed] [Google Scholar]
- Mendes De Leon CF, Appels WPMA, Otten FWJ, Schouten EGW. Risk of Mortality and Coronary Heart Disease by Marital Status in Middle-aged Men in the Netherlands. International Journal of Epidemiology. 1992;21(3):460–466. doi: 10.1093/ije/21.3.460. [DOI] [PubMed] [Google Scholar]
- Metayer C, Coughlin SS, McCarthy EP. Marital Status as a Predictor of Survival in Idiopathic Dilated Cardiomyopathy: The Washington, DC Dilated Cardiomyopathy Study. European Journal of Epidemiology. 1996;12(6):573–582. doi: 10.1007/BF00499455. [DOI] [PubMed] [Google Scholar]
- Mollica RF, Srajlic N, Chernoff M, Lavelle J, Vukovic IS, Massagli MP. Longitudinal Study of Psychiatric Symptoms, Disability, Mortality, and Emigration among Bosnian Refugees. Journal of the American Medical Association. 2001;286(5):546–554. doi: 10.1001/jama.286.5.546. [DOI] [PubMed] [Google Scholar]
- Molloy GJ, Stamatakis E, Randall G, Hamer M. Marital Status, Gender and Cardiovascular Mortality: Behavioural, Psychological Distress and Metabolic Explanations. Social Science & Medicine. 2009;69:223–228. doi: 10.1016/j.socscimed.2009.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moos RH, Brennan PL, Mertens JR. Mortality Rates and Predictors of Mortality among Late Middle-aged and Older Substance-abuse Patients. Alcoholism - Clinical and Experimental Research. 1994;18(1):187–195. doi: 10.1111/j.1530-0277.1994.tb00902.x. [DOI] [PubMed] [Google Scholar]
- Moreno SG, Sutton AJ, Ades AE, Stanley TD, Abrams KR, Peters JL, et al. Assessment of Regression-based Methods to Adjust for Publication Bias through a Comprehensive Study. BMC Medical Research Methodology. 2009;9(2) doi: 10.1186/1471-2288-9-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moser KA, Goldblatt PO, Fox AJ, Jones DR. Unemployment and Mortality: Comparison of the 1971 and 1981 Longitudinal Study Census Samples. British Medical Journal. 1987;294(6564):86–90. doi: 10.1136/bmj.294.6564.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mudar P, Leonard KE, Soltysinski K. Discrepant Substance Use and Marital Functioning in Newlywed Couples. Journal of Consulting and Clinical Psychology. 2001;69(1):130–134. doi: 10.1037//0022-006x.69.1.130. [DOI] [PubMed] [Google Scholar]
- Murphy G, Athanasou JA. The Effect of Unemployment on Mental Health. Journal of Occupational and Organizational Psychology. 1999;72:83–99. [Google Scholar]
- Nagata C, Takatsuka N, Shimizu H. The Impact of Changes in Marital Status on the Mortality of Elderly Japanese. Annals of Epidemiology. 2003;13(4):218–222. doi: 10.1016/s1047-2797(02)00409-x. [DOI] [PubMed] [Google Scholar]
- Nilsson PM, Nilsson JA, Ostergren PO, Berglund G. Social Mobility, Marital Status, and Mortality Risk in an Adult Life Course Perspective: The Malmo Preventive Project. Scandinavian Journal of Public Health. 2005;33(6):412–423. doi: 10.1080/14034940510005905. [DOI] [PubMed] [Google Scholar]
- Norekval TM, Fridlund B, Rokne B, Segadal L, Wentzel-Larsen T, Nordrehaug JE. Patient-reported outcomes as predictors of 10-year survival in women after acute myocardial infarction. Health and Quality of Life Outcomes. 2010;8 doi: 10.1186/1477-7525-8-140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nybo H, Petersen HC, Gaist D, Jeune B, Andersen K, McGue M, et al. Predictors of Mortality in 2,249 Nonagenarians - The Danish 1905-cohort Survey. Journal of the American Geriatrics Society. 2003;51(10):1365–1373. doi: 10.1046/j.1532-5415.2003.51453.x. [DOI] [PubMed] [Google Scholar]
- Ortmeyer CE. Variation in Mortality, Morbidity, and Health Care by Marital Status. In: Erhardt CL, Berlin JE, editors. Mortality and Morbidity in the United States. Cambridge, MA: Harvard University Press; 1974. pp. 159–188. [Google Scholar]
- Parlin LI, Johnson JS. Marital Status, Life-strains and Depression. American Sociological Review. 1977;42(5):704–715. [PubMed] [Google Scholar]
- Patel MK, Patel DA, Lu M, Elshaikh MA, Munkarah A, Movsas B. Impact of Marital Status on Survival Among Women With Invasive Cervical Cancer: Analysis of Population-Based Surveillance, Epidemiology, and End Results Data. Journal of Lower Genital Tract Disease. 2010;14(4):329–338. doi: 10.1097/LGT.0b013e3181ddfa68. [DOI] [PubMed] [Google Scholar]
- Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Comparison of Two Methods to Detect Publication Bias in Meta-analysis. Journal of the American Medical Association. 2006;295(6):676–680. doi: 10.1001/jama.295.6.676. [DOI] [PubMed] [Google Scholar]
- Rahman MO. Excess Mortality for the Unmarried in Rural Bangladesh. International Journal of Epidemiology. 1993;22(3):445–456. doi: 10.1093/ije/22.3.445. [DOI] [PubMed] [Google Scholar]
- Rahman MO. The Effects of Spouses on the Mortality of Older People in Rural Bangladesh. Health Transition Review. 1997;7:1–12. [Google Scholar]
- Regidor E, Calle ME, Dominguez V, Navarro P. [Mortality by Social and Economic Characteristics: The Mortality Study of the Autonomous Community of Madrid, Spain] Medicina Clinica (Barcelona) 2001;116(19):726–731. doi: 10.1016/s0025-7753(01)71966-5. [DOI] [PubMed] [Google Scholar]
- Rendall MS, Weden MM, Favreault MM, Waldron H. The Protective Effect of Marriage for Survival: A Review and Update. Demography. 2011;48(2):481–506. doi: 10.1007/s13524-011-0032-5. [DOI] [PubMed] [Google Scholar]
- Roelfs DJ, Shor E, Davidson KW, Schwartz JE. War-Related Stress Exposure and Mortality: A Meta-Analysis. The International Journal of Epidemiology. 2010;39:1499–1509. doi: 10.1093/ije/dyq132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roelfs DJ, Shor E, Davidson KW, Schwartz JE. Losing Life and Livelihood: A Systematic Review and Meta-Analysis of Unemployment and All-Cause Mortality. Social Science & Medicine. 2011;72(6):840–854. doi: 10.1016/j.socscimed.2011.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roelfs DJ, Shor E, Kalish R, Yogev T. The Rising Relative Risk of Mortality among Singles: Meta-analysis and Meta-regression. American Journal of Epidemiology. 2011;74(4):379–389. doi: 10.1093/aje/kwr111. [DOI] [PubMed] [Google Scholar]
- Rogers RG. Marriage, Sex, and Mortality. Journal of Marriage and the Family. 1995;57(2):515–526. [Google Scholar]
- Rosengren A, Orthgomer K, Wedel H, Wilhelmsen L. Stressful Life Events, Social Support, and Mortality in Men Born in 1933. British Medical Journal. 1993;307(6912):1102–1105. doi: 10.1136/bmj.307.6912.1102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosengren A, Wedel H, Wilhelmsen L. Marital Status and Mortality in Middle-Aged Swedish Men. American Journal of Epidemiology. 1989;129(1):54–64. doi: 10.1093/oxfordjournals.aje.a115124. [DOI] [PubMed] [Google Scholar]
- Ross CE, Mirowsky J, Goldsteen K. The Impact of the Family on Health:Decade in Review. Journal of Marriage and the Family. 1990;52:1059–1078. [Google Scholar]
- Rushing WA. Marital Status and Mental Disorder: Evidence on Favor of a Behavioral Model. Social Forces. 1979;58(2):540–556. [Google Scholar]
- Samuelsson G, Dehlin O. Family Network and Mortality - Survival Chances Through the Life-Span of an Entire Age Cohort. International Journal of Aging and Human Development. 1993;37(4):277–295. doi: 10.2190/FRRH-UR9D-3FF9-UDXP. [DOI] [PubMed] [Google Scholar]
- Schaefer C, Coyne JC, Lazarus RS. The Health-Related Functions of Social Support. Journal of Behavioral Medicine. 1981;4(4):381–406. doi: 10.1007/BF00846149. [DOI] [PubMed] [Google Scholar]
- Sheps MC. Marriage and Mortality. American Journal of Public Health. 1961;51(4):547–555. doi: 10.2105/ajph.51.4.547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shkolnikov VM, Jasilionis D, Andreev EM, Jdanov DA, Stankuniene V, Ambrozaltiene D. Linked versus Unlinked Estimates of Mortality and Length of Life by Education and Marital Status: Evidence from the First Record Linkage Study in Lithuania. Social Science & Medicine. 2007;64(7):1392–1406. doi: 10.1016/j.socscimed.2006.11.014. [DOI] [PubMed] [Google Scholar]
- Shor E, Roelfs DJ, Curreli M, Clemow L, Burg M, Schwartz JE. Widowhood and Mortality: A Meta-analysis and Meta-regression. Demography. 2012 doi: 10.1007/s13524-012-0096-x. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shurtleff D. Mortality and Marital Status. Public Health Reports. 1955;70(3):248–252. [PMC free article] [PubMed] [Google Scholar]
- Shurtleff D. Mortality among the Married. Journal of the American Geriatrics Society. 1956;4(7):654–666. doi: 10.1111/j.1532-5415.1956.tb00849.x. [DOI] [PubMed] [Google Scholar]
- Singh GK, Siahpush M. All-Cause and Cause-Specific Mortality of Immigrants and Native Born in the United States. American Journal of Public Health. 2001;91(3):392–399. doi: 10.2105/ajph.91.3.392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh GK, Siahpush M. Ethnic-immigrant Differentials in Health Behaviors, Morbidity, and Cause-specific Mortality in the United States: An Analysis of Two National Data Bases. Human Biology. 2002;74(1):83–109. doi: 10.1353/hub.2002.0011. [DOI] [PubMed] [Google Scholar]
- Smith KR, Waitzman NJ. Double Jeopardy - Interaction Effects of Marital and Poverty Status on the Risk of Mortality. Demography. 1994;31(3):487–507. [PubMed] [Google Scholar]
- Smith KR, Zick CD. Linked Lives, Dependent Demise - Survival Analysis of Husbands and Wives. Demography. 1994;31(1):81–93. [PubMed] [Google Scholar]
- Smock PJ. The Economic Costs of Marital Disruption for Young Women Over the Past Two Decades. Demography. 1993;30(3):353–371. [PubMed] [Google Scholar]
- Smock PJ. Gender and the Short-Run Economic Consequences of Marital Disruption. Social Forces. 1994;73(1):243–262. [Google Scholar]
- Smock PJ, Manning WD, Gupta S. The Effect of Marriage and Divorce on Women’s Economic Well-being. American Sociological Review. 1999;64:794–812. [Google Scholar]
- Sorlie PD, Backlund E, Keller JB. U.S. Mortality by Economic, Demographic, and Social Characteristics - The National Longitudinal Mortality Study. American Journal of Public Health. 1995;85(7):949–956. doi: 10.2105/ajph.85.7.949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence NJ. Sociology. Tallahassee: Florida State University; 2006. Reproductive Patterns and Women’s Later Life Health. [Google Scholar]
- Terrin N, Schmid CH, Lau J, Olkin I. Adjusting for Bias in the Presence of Heterogeneity. Statistics in Medicine. 2003;22:2113–2126. doi: 10.1002/sim.1461. [DOI] [PubMed] [Google Scholar]
- Thornton A, Rodgers W. The Influence of Individual and Historical Time on Marital Dissolution. Demography. 1987;24:1–22. [PubMed] [Google Scholar]
- Tsai SL, Lan CF, Lee CH, Huang N, Chou YJ. Involuntary Unemployment and Mortality in Taiwan. Journal of the Formosan Medical Association. 2004;103:900–907. [PubMed] [Google Scholar]
- Tucker JS, Friedman HS, Schwartz JE, Criqui MH, Tomlinson-Keasey C, Wingard DL, et al. Parental Divorce: Effects on Individual Behavior and Longevity. Journal of Personality and Social Psychology. 1997;73(2):381–391. doi: 10.1037//0022-3514.73.2.381. [DOI] [PubMed] [Google Scholar]
- Tucker JS, Friedman HS, Wingard DL, Schwartz JE. Marital History at Midlife as a Predictor of Longevity: Alternative Explanations to the Protective Effect of Marriage. Health Psychology. 1996;15(2):94–101. doi: 10.1037//0278-6133.15.2.94. [DOI] [PubMed] [Google Scholar]
- Uchino BN, Cacioppo JT, Kiecolt-Glaser JK. The Relationship between Social Support and Psychological Processes: A Review with Emphasis on Underlying Mechanisms and Implications for Health. Psychological Bulletin. 1996;119(3):488–531. doi: 10.1037/0033-2909.119.3.488. [DOI] [PubMed] [Google Scholar]
- Umberson D, Wortman CB, Kessler RC. Widowhood and Depression: Explaining Long-Term Gender Differences in Volunerability. Journal of Health and Social Behavior. 1992;33(1):10–24. [PubMed] [Google Scholar]
- Va P, Yang WS, Nechuta S, Chow WH, Cai H, Yang G, et al. Marital Status and Mortality among Middle Age and Elderly Men and Women in Urban Shanghai. PloS one. 2011;6(11):e26600. doi: 10.1371/journal.pone.0026600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vallin J, Nizard A. Mortality by Marital Status: Marriage Selection or Marriage Protection. Population (French Edition) 1977 Sep;32:95–125. [Google Scholar]
- van Poppel FWA, Joung IMA. Long-term Trends in Marital Status Mortality Differences in the Netherlands 1850-1970. Journal of Biosocial Science. 2001;33(2):279–303. doi: 10.1017/s0021932001002796. [DOI] [PubMed] [Google Scholar]
- Villingshoj M, Ross L, Thomsen BL, Johansen C. Does Marital Status and Altered Contact with the Social Network Predict Colorectal Cancer Survival? European Journal of Cancer. 2006;42(17):3022–3027. doi: 10.1016/j.ejca.2006.04.027. [DOI] [PubMed] [Google Scholar]
- Wang L, Wilson SE, Stewart DB, Hollenbeak CS. Marital status and colon cancer outcomes in US Surveillance, Epidemiology and End Results registries: Does marriage affect cancer survival by gender and stage? Cancer Epidemiology. 2011;35(5):417–422. doi: 10.1016/j.canep.2011.02.004. [DOI] [PubMed] [Google Scholar]
- Williams DR, Takeuchi DT, Adair RK. Marital Status and Psychiatric Disorders among Blacks and Whites. Journal of Health and Social Behavior. 1992;33(140-157) [PubMed] [Google Scholar]
- Williams K, Sassier S, Nicholson LM. For Better or for Worse: The Consequences of Marriage and Cohabitation for Single Mothers. Social Forces. 2008;86:1481–1512. [Google Scholar]
- Williams K, Umberson D. Marital Status, Marital Transitions, and Health: A Gendered Life Course Perspective. Journal of Health and Social Behavior. 2004;45:81–98. doi: 10.1177/002214650404500106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wyke S, Ford G. Competing Explanation for Associations between Marital Status and Health. Social Science and Medicine. 2002;34(5):523–532. doi: 10.1016/0277-9536(92)90208-8. [DOI] [PubMed] [Google Scholar]
- Xavier AJ, d’Orsi E, Sigulem D, Ramos LR. Time orientation and executive functions in the prediction of mortality in the elderly: Epidoso study. Revista de Saude Publica. 2010;44(1):148–158. doi: 10.1590/s0034-89102010000100016. [DOI] [PubMed] [Google Scholar]
- Yamaguchi K, Kandel DB. The Influence of Spuses’ Behavior and Marital Dissolution on Marijuana Use: Causation or Selection. Journal of Marriage and the Family. 1997;59:22–36. [Google Scholar]
- Zajacova A. Education, Gender, and Mortality: Does Schooling have the Same Effect on Mortality for Men and Women in the US? Social Science & Medicine. 2006;63(8):2176–2190. doi: 10.1016/j.socscimed.2006.04.031. [DOI] [PubMed] [Google Scholar]
- Zajacova A, Hummer RA. Gender differences in education effects on all-cause mortality for white and black adults in the United States. Social Science & Medicine. 2009;69(4):529–537. doi: 10.1016/j.socscimed.2009.06.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang J, Yu KF. What’s the Relative Risk? A Method of Correcting the Odds Ratio in Cohort Studies of Common Outcomes. Journal of the American Medical Association. 1998;280:1690–1691. doi: 10.1001/jama.280.19.1690. [DOI] [PubMed] [Google Scholar]
- Zick CD, Smith KR. Marital Transitions, Poverty, and Gender Differences in Mortality. Journal of Marriage and the Family. 1991;53(2):327–336. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.