

Abstract
Although liver transplantation is theoretically the best treatment for hepatocellular carcinoma (HCC), it is limited by the realities of perioperative complications, and the shortage of donor organs. Furthermore, in many cases there are available alternative treatments such as resection or locoregional therapy. Deciding upon the best option for a patient with HCC is complicated, involving numerous ethical principles including: urgency, utility, intention-to-treat survival, transplant benefit, harm to candidates on waiting list, and harm to living donors. The potential contrast between different principles is particularly relevant for patients with HCC for several reasons: (1) HCC candidates to liver transplantation are increasing; (2) the great prognostic heterogeneity within the HCC population; (3) in HCC patients tumor progression before liver transplantation may significantly impair post transplant outcome; and (4) effective alternative therapies are often available for HCC candidates to liver transplantation. In this paper we suggest that allocating organs by transplant benefit could help balance these competing principles, and also introduce equity between patients with HCC and nonmalignant liver disease. We also propose a triangular equipoise model to help decide between deceased donor liver transplantation, living donor liver transplantation, or alternative therapies.
Keywords: Hepatocellular carcinoma, Deceased donor liver transplantation, Living donor liver transplantation, Transplant benefit, Utility, Urgency, Intention-to-treat survival, Harm
Core tip: Deciding upon the best option for a patient with hepatocellular carcinoma is complicated, involving numerous ethical principles including: urgency, utility, intention-to-treat survival, transplant benefit, harm to candidates on waiting list, and harm to living donors. In this paper we suggest that allocating organs by transplant benefit could help balance these competing principles, and also introduce equity between patients with hepatocellular carcinoma and those with nonmalignant liver disease. We also propose a triangular equipoise model to help decide between deceased donor liver transplantation, living donor liver transplantation, or alternative therapies.
GENERAL PRINCIPLES REGULATING PATIENT SELECTION AND ORGAN ALLOCATION IN LIVER TRANSPLANTATION
Urgency, utility, and equity
Liver transplantation (LT) is theoretically the best treatment for patients with end-stage liver disease but its effectiveness is limited by intrinsic characteristics with important ethical implications: (1) LT remains a technical demanding procedure with a well-established short-term mortality and morbidity[1]; (2) a persistent shortage of deceased donors corresponds to an increasing demand of deceased donor liver transplantation (DDLT)[2]; and (3) the application of living donor liver transplantation (LDLT) is limited by ethical and legal issues related to the risk of harming the living donor[3]. Specific selection policies have consequently been developed over the last two decades to identify good candidates for this complex therapeutic option[4,5].
For patients with non-malignant (NM) liver cirrhosis, scores have been developed to measure disease severity, such as the Child Pugh and the model for end-stage liver disease (MELD) scores[4], which support a selection policy based on the urgency principle. Under a medical urgency-based selection system, patients with worse outcomes while on the waiting list (WL) are given higher priority for transplantation[6]. Use of the MELD score, for example, has significantly reduced waiting list times and in the United States system in recent years[4,7]. If we consider the development of hepatocellular carcinoma (HCC) as a complication of liver cirrhosis, and therefore as a sign of disease severity, assigning a high priority to HCC patients would also comply with this principle of urgency. This viewpoint is reflected in the United Network for Organ Sharing (UNOS) allocation system, where an arbitrary high MELD score is assigned to patients with T2-HCC[7].
The limit of this approach is that it fails to consider the extremely relevant prognostic heterogeneity of patients with HCC and the potential effectiveness of alternative therapies[8]. It is also only reasonable to consider HCC as a complication of liver cirrhosis if this condition is maintained within certain proportions of candidates on the WL (e.g., < 20%), as in the US[9]. In some geographical LT settings, however, there has been a significant increase in the proportion of LT candidates on the WL with liver tumors in recent years and this has given rise to similar proportions of liver transplants for HCC and NM disease[10]. In these modern LT realities, it is probably more reasonable to consider HCC patients as a separate LT population and analyze the prognostic heterogeneity of this particular medical condition more deeply[11].
If we observe the issues of patient selection and organ allocation from the HCC population point of view, therefore, current LT selection policies for HCC patients (e.g., the UNOS allocation system) appear to be based mainly on a utility principle for two main reasons. First, a utility-based system is one that gives priority according to expected post-transplant outcomes[6]. For patients with HCC, the poor results achieved in early experiences with patients transplanted for advanced tumors have favored the introduction of strict selection criteria focusing mainly on post-LT outcome[5]. Therefore, patients beyond Milan criteria have limited probability of receiving a transplant.
Second, in the current system all T2 HCC patients receive the same priority regardless of their likelihood of death on the waiting list.
If we consider LT candidates with and without cancer as two separate populations, therefore, apparently opposite allocation principles are currently used at the majority of LT centers around the world. This diversity in patient selection policy intrinsically creates an ethical paradox, in that donated organs are allocated to the “sickest patient first” among the candidates with NM hepatic disease, but to the “earliest patient first” among candidates for LT who have HCC, irrespective of their survival prospects with therapies other than transplantation.
Aristotle defined justice as “treating equal cases equally, and unequal cases unequally”. One of the fundamental challenges of organ allocation science is maintaining equity among the heterogeneous groups of patients on the waiting list. In the specific organ allocation context, equity means treating all patients according to a common endpoint. From this perspective, the principle of equity is hierarchically more important than all others, whether we decide to favour urgency, or utility or benefit as endpoints for our allocation system.
Based on these considerations (i.e., the increasing proportion of HCC patients enlisted, and an excess of priority for HCC patients with a low urgency for LT), recent proposals have tried to resolve the unbalance in the access to transplantation between HCC and non-HCC patients. One attempt involved developing risk models within the HCC population for 3-mo drop-out risk as common urgency endpoint[12,13]. However, this approach (i.e., to equate the drop-out risk of different patients) carries the risk of prioritizing HCC patients with higher biological aggressiveness in terms of nodule size and AFP levels, and consequently dramatically increasing the risk of post-LT tumour recurrence or death[14]. Thus, methods are needed which balance the principles of urgency and utility when attempting to reach equity between HCC and non-HCC patients.
Intention-to-treat survival
To describe the effect of long waiting times on the effectiveness of LT as curative therapy for HCC[15], some years ago the concept of intention-to-treat (ITT) survival was introduced. Interestingly, analyzing the survival figures of HCC patients from the day of enlisting and not from that of transplant, the overall results of LT for HCC became worse than resection[16] due to the high dropout rate of HCC patients from the WL for tumor progression.
However, ITT survival is strongly related to the specific local/regional WL characteristics and in particular to the patient median waiting time: assuming as a constant the post-LT outcome, the lower the pre- LT mortality, the higher the intention-to-treat survival. For this reason, in a clinical scenario where HCC patients receive high priority for LT (i.e., low waiting time and low risk of dropout) the intention-to-treat survival of LT for HCC patients may exceed that of liver resection[17].
For these reasons, survival analysis in LT should use the ITT principle because it accounts for all the complex LT processes from the day that LT is first considered.
Transplant benefit
The concept of transplant benefit expresses the survival gain offered by LT by comparison with the best alternative therapy. Transplant benefit can be calculated from the time of transplant, or from the time a patient is first evaluated for transplant-the latter would make it an ITT endpoint. On an individual basis, the main advantage of this principle is that it covers the overall LT process, simultaneously considering post- and pre-LT outcome. The transplant benefit principle applied to the individual LT candidate thus has the potential to create an ideal balance between the concepts of urgency and utility. As suggested by Schaubel et al[6], moreover, by prioritizing patients based on life-years gained thanks to transplantation, the transplant benefit principle performs better than urgency and utility schemes from a population perspective too. This is because an urgency-based system would assign donor organs to patients who are most likely to die while on the WL, but this approach may be to the detriment of utility because patients at the greatest risk of death while on the WL may also be patients with the highest post-LT mortality risk. A utility-based allocation system would ensure that transplanted organs go to patients with the lowest post-LT mortality risk, but patients with the best post-LT outcomes may also have the best outcomes while on the WL. The transplant benefit principle is consequently the one best able to maximize the total life-years gained by the patient population.
In recent years, the transplant benefit principle has been proposed for LT candidates based on studies using data from the Scientific Registry of Transplant Recipients (SRTR)[2,6,18], but these studies did not consider the transplant benefit for the HCC population of LT candidates, because they either focused only on NM candidates[2,11] or they considered HCC as a complication[6] and not as a separate, prognostically heterogeneous medical condition.
The concept of transplant benefit has the intrinsic potential for being especially useful for HCC patients since a particular feature of the approach lies in that it is calculated by subtracting the area under the survival curve after alternative therapies from the area under the survival curve after transplantation[9], a definition that coincides with the gain in life expectancy (LE). This gives a relevant weight not only to the crude post-LT outcome, but also to the alternative therapies available and to the patient’s age, which are extremely important prognostic variables for HCC patients[19]. Figure 1 shows two different clinical scenarios. The first (Figure 1A) concerns the case of a young patient (40 years old) with a tumor beyond the Milan criteria (calculated 5-year post-transplant survival = 60%). The lack of any effective alternative therapies makes the benefit of LT extremely high (8 years). The second scenario (Figure 1B) considers an older patient (65-year-old) within the accepted indications for LT (5-year post-transplant survival = 70%), but with an effective alternative treatment option, i.e., liver resection, which makes the benefit of LT much lower (4 years) than in the first case, although the post-LT outcome would be better.
Figure 1.

Clinical examples of the transplant benefit principle applied to hepatocellular carcinoma patients. A: Man 40-year-old, HBV with 2 HCC nodules, the largest of 6 cm, Child B (Milan out, University of California San Francisco out); B: Man 65-year-old, HCV, with 1 HCC (diameter = 4 cm), Child A. HCC: Hepatocellular carcinoma; HBV: Hepatitis B virus; HCV: Hepatitis C virus.
The recent publication of important studies on the survival prospects of patients with more advanced tumors after LT[20] and other therapies[21,22] makes it potentially feasible now to evaluate transplant benefit across different stages of HCC disease. This could be extremely important because, from a utility perspective, adopting extended criteria for HCC patients would mean allocating more donated organs to HCC patients than to NM patients[16]; taking a transplant benefit perspective, on the other hand, would mean reallocating the same number of organs to different groups of patients with a greater benefit. In other words, the transplant benefit principle would be able to maximize the total life-years of both the HCC and NM population.
These concepts have been recently incorporated in three papers[23-25] evaluating the transplant benefit principle in the HCC population. These studies underline three main points: (1) Liver transplantation results in the highest survival benefit for HCC patients with advanced liver cirrhosis (BCLC stage D); (2) Patients with intermediate tumours (BCLC stages B-C) without effective alternative therapies receive a relevant benefit from LT, regardless of the nodule number-size criteria (i.e., Milan criteria), provided that macroscopic vascular invasion and extra-hepatic disease are absent; and (3) Patients with early tumors and compensated cirrhosis have the lowest benefit from LT when effective alternative therapies are available[23-25].
Harm-benefit to other patients on the waiting list
When patients on a given WL receive an organ, they harm the rest of the candidates on the WL because it is as if they were taking that organ away from other potential candidates. The entity of this harm depends on the extra time the other patients on the WL have to wait for another organ. We can also see this concept from the opposite point of view: if we find an alternative treatment for a patient on a WL for LT (e.g., if we perform a LDLT or a liver resection), we create a benefit for the people on said WL that can be calculated from the further waiting time they spare. Knowing the characteristics of a WL in detail (death probabilities according to disease severity, median waiting time for LT, mean number of organs per year, patient stratification according to MELD score and HCC stage), we can calculate this harm/benefit to candidates on the WL[9,26,27]. This is very important because it is the only allocation principle that takes the characteristics of a specific WL into account (WL size, donor resources and proportions of patients with severe disease).
Harm to the living donor
The crucial element limiting the general applicability of LDLT is the risk of harming a healthy living donor. In the literature, the overall mortality attributed to living donor procedures is lower than 1%, but the risk of morbidity is significant, being around 38% in some experiences as a whole, and < 10% when severe complications are considered alone[28].
A recent worldwide survey[29] has brought more evidence about this field. Overall donor morbidity rate was 24%, but only 0.2% of them died, and 0.04% required transplantation. If harm to donors is only considered in terms of mortality, its impact on the therapeutic decision (between LDLT, DDLT, or no LT) would be minimal compared to the recipient’s risk of death on the WL[30]. Quantifying morbidity could be done by determining the impact of complications on quality of life, but limited data is currently available to derive such estimates.
Furthermore, it is controversial whether donor morbidity and mortality should be weighted equally to that of the recipient[31]. Currently the transplant community takes a protective approach (paternalist principle) to the living donor, and tends to assign greater ethical weight to the donor’s risk of death than to the recipient’s risk of death. This approach, however, comes at the expense of donor autonomy. Further thought is needed on this subject, including input from donors themselves.
One interesting proposal is to define a cut-off for acceptable morbidity and mortality from the perspective of the donor[32,33].
REPRESENTATION OF THE POTENTIAL EQUIPOISE BETWEEN BENEFITS AND HARMS OF TRANSPLANTATION FOR HCC PATIENTS
An ideal selection/allocation process for patients with HCC should consider all aspects of the benefits and harms of LT, and the aim of allocation systems should be to reach a balance between the different principles involved in the selection process.
We have represented this equipoise using a triangle containing vectors (Figure 2): the transplant benefit (life expectancy with LT minus life expectancy without LT) is at the top vertex and the potential harm to the rest of the WL and to the living donor at the bottom vertices. According to this model, transplantation is generally indicated when the transplant benefit exceeds the harm. Then, according to the relative weights of the harm to the WL and donor, the decision will be oriented towards LDLT or DDLT.
Figure 2.
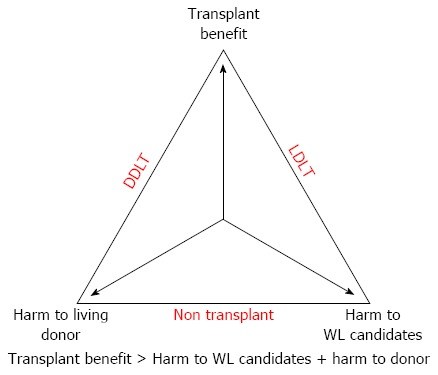
Ethical equipoise between benefit and harm of deceased-donor liver transplantation and living donor liver transplantation. WL: Waiting list; DDLT: Deceased donor liver transplantation; LDLT: Living donor liver transplantation.
The first advantage of this conceptual model is that it includes all ethical principles involved in the LT decision process. The use of transplant benefit satisfies both utility and urgency principles, while the relationship between benefit and harm to the waiting list satisfies equity-the first principle aims to maximize the need of the single patient, while the second maximizes population total life years[26].
The second advantage of this model is that it considers as different therapeutic procedures DDLT and LDLT. Whenever we used urgency, utility or benefit, these principles taken alone do not distinguish between LDLT and DDLT, so they cannot be used to decide between these different strategies. The indication for LDLT is therefore inevitably the same as for DDLT[32,33], so choosing between the two is difficult. This may partially explain why LDLT has had a limited development in Western countries, especially since the introduction of the MELD[33].
Some authors[32] have recently stressed the possibility to consider different indications between LDLT and DDLT based on the consideration that living donor recipients don’t compete with other patients on the WL. The same authors proposed a sort of double equipoise model specific for LDLT to balance the donor risk and the recipient benefit[32]. Our model has the advantage to be used for both DDLT and LDLT. LDLT has a potentially relevant advantage over DDLT because it only minimally harms the other candidates on the WL: this harm is limited to the risk of the patient needing re-LT after LDLT, which is estimated to be approximately 7%[34], while the risk of liver failure requiring transplantation of the donor is estimated to be 0.04%[29].
This model helps the selection of HCC patients for LT and the choice of the more appropriate transplant procedure (DDLT vs LDLT). However, it can not consider some crucial aspects. First of all, in some countries religiosity or cultural aspects are barriers to DDLT[31]. As second point, in some recipients of a partial liver from a living donor insufficient liver volume can not be avoided to maintain an adequate donor safety. A small-for-size graft easily causes perioperative complications and results in poor outcomes[31]. In summary, although LT is theoretically the best treatment for HCC, it is limited by the realities of perioperative complications, and the shortage of donor organs. Furthermore, the benefit of transplantation is not uniform among patients with HCC; rather, it depends upon the severity of liver disease and the available alternative treatment options. Current systems allocate organs to HCC patients primarily based upon the utility principle, as opposed to the urgency principle which governs allocation to patients with nonmalignant liver disease. Allocating organs by transplant benefit could introduce equity between these patient groups. We propose a triangular equipoise model to help decide between DDLT, LDLT, or alternative therapies.
Footnotes
P- Reviewers: Boin I, Koike H, Tomohide H S- Editor: Qi Y L- Editor: A E- Editor: Zhang DN
References
- 1.Freeman RB, Steffick DE, Guidinger MK, Farmer DG, Berg CL, Merion RM. Liver and intestine transplantation in the United States, 1997-2006. Am J Transplant. 2008;8:958–976. doi: 10.1111/j.1600-6143.2008.02174.x. [DOI] [PubMed] [Google Scholar]
- 2.Merion RM, Schaubel DE, Dykstra DM, Freeman RB, Port FK, Wolfe RA. The survival benefit of liver transplantation. Am J Transplant. 2005;5:307–313. doi: 10.1111/j.1600-6143.2004.00703.x. [DOI] [PubMed] [Google Scholar]
- 3.Belghiti J. Will improved donor safety increase liver donations? Transplantation. 2009;88:19–20. doi: 10.1097/TP.0b013e3181a9ea53. [DOI] [PubMed] [Google Scholar]
- 4.Freeman RB. The model for end-stage liver disease comes of age. Clin Liver Dis. 2007;11:249–263. doi: 10.1016/j.cld.2007.04.005. [DOI] [PubMed] [Google Scholar]
- 5.Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, Montalto F, Ammatuna M, Morabito A, Gennari L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. doi: 10.1056/NEJM199603143341104. [DOI] [PubMed] [Google Scholar]
- 6.Schaubel DE, Guidinger MK, Biggins SW, Kalbfleisch JD, Pomfret EA, Sharma P, Merion RM. Survival benefit-based deceased-donor liver allocation. Am J Transplant. 2009;9:970–981. doi: 10.1111/j.1600-6143.2009.02571.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ioannou GN, Perkins JD, Carithers RL. Liver transplantation for hepatocellular carcinoma: impact of the MELD allocation system and predictors of survival. Gastroenterology. 2008;134:1342–1351. doi: 10.1053/j.gastro.2008.02.013. [DOI] [PubMed] [Google Scholar]
- 8.Goldring S, Edwards I, Harding GW, Bernardo KL. Results of anterior temporal lobectomy that spares the amygdala in patients with complex partial seizures. J Neurosurg. 1992;77:185–193. doi: 10.3171/jns.1992.77.2.0185. [DOI] [PubMed] [Google Scholar]
- 9.Volk ML, Vijan S, Marrero JA. A novel model measuring the harm of transplanting hepatocellular carcinoma exceeding Milan criteria. Am J Transplant. 2008;8:839–846. doi: 10.1111/j.1600-6143.2007.02138.x. [DOI] [PubMed] [Google Scholar]
- 10.Angelico M, Cillo U, Fagiuoli S, Gasbarrini A, Gavrila C, Marianelli T, Costa AN, Nardi A, Strazzabosco M, Burra P, et al. Liver Match, a prospective observational cohort study on liver transplantation in Italy: study design and current practice of donor-recipient matching. Dig Liver Dis. 2011;43:155–164. doi: 10.1016/j.dld.2010.11.002. [DOI] [PubMed] [Google Scholar]
- 11.Navasa M, Bruix J. Multifaceted perspective of the waiting list for liver transplantation: the value of pharmacokinetic models. Hepatology. 2010;51:12–15. doi: 10.1002/hep.23332. [DOI] [PubMed] [Google Scholar]
- 12.Washburn K, Edwards E, Harper A, Freeman R. Hepatocellular carcinoma patients are advantaged in the current liver transplant allocation system. Am J Transplant. 2010;10:1643–1648. doi: 10.1111/j.1600-6143.2010.03127.x. [DOI] [PubMed] [Google Scholar]
- 13.Toso C, Dupuis-Lozeron E, Majno P, Berney T, Kneteman NM, Perneger T, Morel P, Mentha G, Combescure C. A model for dropout assessment of candidates with or without hepatocellular carcinoma on a common liver transplant waiting list. Hepatology. 2012;56:149–156. doi: 10.1002/hep.25603. [DOI] [PubMed] [Google Scholar]
- 14.Cucchetti A, Cescon M, Bertuzzo V, Bigonzi E, Ercolani G, Morelli MC, Ravaioli M, Pinna AD. Can the dropout risk of candidates with hepatocellular carcinoma predict survival after liver transplantation? Am J Transplant. 2011;11:1696–1704. doi: 10.1111/j.1600-6143.2011.03570.x. [DOI] [PubMed] [Google Scholar]
- 15.Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999;30:1434–1440. doi: 10.1002/hep.510300629. [DOI] [PubMed] [Google Scholar]
- 16.Koniaris LG, Levi DM, Pedroso FE, Franceschi D, Tzakis AG, Santamaria-Barria JA, Tang J, Anderson M, Misra S, Solomon NL, et al. Is surgical resection superior to transplantation in the treatment of hepatocellular carcinoma? Ann Surg. 2011;254:527–37; discussion 537-8. doi: 10.1097/SLA.0b013e31822ca66f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Adam R, Bhangui P, Vibert E, Azoulay D, Pelletier G, Duclos-Vallée JC, Samuel D, Guettier C, Castaing D. Resection or transplantation for early hepatocellular carcinoma in a cirrhotic liver: does size define the best oncological strategy? Ann Surg. 2012;256:883–891. doi: 10.1097/SLA.0b013e318273bad0. [DOI] [PubMed] [Google Scholar]
- 18.Schaubel DE, Sima CS, Goodrich NP, Feng S, Merion RM. The survival benefit of deceased donor liver transplantation as a function of candidate disease severity and donor quality. Am J Transplant. 2008;8:419–425. doi: 10.1111/j.1600-6143.2007.02086.x. [DOI] [PubMed] [Google Scholar]
- 19.Lee HS. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria: the controversies continue. Dig Dis. 2007;25:296–298. doi: 10.1159/000106907. [DOI] [PubMed] [Google Scholar]
- 20.Mazzaferro V, Llovet JM, Miceli R, Bhoori S, Schiavo M, Mariani L, Camerini T, Roayaie S, Schwartz ME, Grazi GL, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10:35–43. doi: 10.1016/S1470-2045(08)70284-5. [DOI] [PubMed] [Google Scholar]
- 21.Bruix J, Llovet JM. Major achievements in hepatocellular carcinoma. Lancet. 2009;373:614–616. doi: 10.1016/S0140-6736(09)60381-0. [DOI] [PubMed] [Google Scholar]
- 22.Toso C, Kneteman NM, James Shapiro AM, Bigam DL. The estimated number of patients with hepatocellular carcinoma selected for liver transplantation using expanded selection criteria. Transpl Int. 2009;22:869–875. doi: 10.1111/j.1432-2277.2009.00882.x. [DOI] [PubMed] [Google Scholar]
- 23.Cillo U, Vitale A, Volk ML, Frigo AC, Grigoletto F, Brolese A, Zanus G, D’Amico F, Farinati F, Burra P, et al. The survival benefit of liver transplantation in hepatocellular carcinoma patients. Dig Liver Dis. 2010;42:642–649. doi: 10.1016/j.dld.2010.02.010. [DOI] [PubMed] [Google Scholar]
- 24.Vitale A, Morales RR, Zanus G, Farinati F, Burra P, Angeli P, Frigo AC, Del Poggio P, Rapaccini G, Di Nolfo MA, et al. Barcelona Clinic Liver Cancer staging and transplant survival benefit for patients with hepatocellular carcinoma: a multicentre, cohort study. Lancet Oncol. 2011;12:654–662. doi: 10.1016/S1470-2045(11)70144-9. [DOI] [PubMed] [Google Scholar]
- 25.Berry K, Ioannou GN. Are patients with Child’s A cirrhosis and hepatocellular carcinoma appropriate candidates for liver transplantation? Am J Transplant. 2012;12:706–717. doi: 10.1111/j.1600-6143.2011.03853.x. [DOI] [PubMed] [Google Scholar]
- 26.Volk ML, Lok AS, Ubel PA, Vijan S. Beyond utilitarianism: a method for analyzing competing ethical principles in a decision analysis of liver transplantation. Med Decis Making. 2008;28:763–772. doi: 10.1177/0272989X08316999. [DOI] [PubMed] [Google Scholar]
- 27.Cucchetti A, Vitale A, Gaudio MD, Ravaioli M, Ercolani G, Cescon M, Zanello M, Morelli MC, Cillo U, Grazi GL, et al. Harm and benefits of primary liver resection and salvage transplantation for hepatocellular carcinoma. Am J Transplant. 2010;10:619–627. doi: 10.1111/j.1600-6143.2009.02984.x. [DOI] [PubMed] [Google Scholar]
- 28.Ghobrial RM, Freise CE, Trotter JF, Tong L, Ojo AO, Fair JH, Fisher RA, Emond JC, Koffron AJ, Pruett TL, et al. Donor morbidity after living donation for liver transplantation. Gastroenterology. 2008;135:468–476. doi: 10.1053/j.gastro.2008.04.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cheah YL, Simpson MA, Pomposelli JJ, Pomfret EA. Incidence of death and potentially life-threatening near-miss events in living donor hepatic lobectomy: a world-wide survey. Liver Transpl. 2013;19:499–506. doi: 10.1002/lt.23575. [DOI] [PubMed] [Google Scholar]
- 30.Sarasin FP, Majno PE, Llovet JM, Bruix J, Mentha G, Hadengue A. Living donor liver transplantation for early hepatocellular carcinoma: A life-expectancy and cost-effectiveness perspective. Hepatology. 2001;33:1073–1079. doi: 10.1053/jhep.2001.23311. [DOI] [PubMed] [Google Scholar]
- 31.Miller CM. Ethical dimensions of living donation: experience with living liver donation. Transplant Rev (Orlando) 2008;22:206–209. doi: 10.1016/j.trre.2008.02.001. [DOI] [PubMed] [Google Scholar]
- 32.Pomfret EA, Lodge JP, Villamil FG, Siegler M. Should we use living donor grafts for patients with hepatocellular carcinoma? Ethical considerations. Liver Transpl. 2011;17 Suppl 2:S128–S132. doi: 10.1002/lt.22356. [DOI] [PubMed] [Google Scholar]
- 33.Brown RS. Live donors in liver transplantation. Gastroenterology. 2008;134:1802–1813. doi: 10.1053/j.gastro.2008.02.092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Olthoff KM, Merion RM, Ghobrial RM, Abecassis MM, Fair JH, Fisher RA, Freise CE, Kam I, Pruett TL, Everhart JE, et al. Outcomes of 385 adult-to-adult living donor liver transplant recipients: a report from the A2ALL Consortium. Ann Surg. 2005;242:314–323, discussion 323-325. doi: 10.1097/01.sla.0000179646.37145.ef. [DOI] [PMC free article] [PubMed] [Google Scholar]