

Abstract
The importance of the lateral meniscus in weight bearing, distribution of force, shock absorption, articular cartilage protection, proprioception, stabilization of the joint, and joint lubrication is well known. Surgeons currently agree on the importance of preserving the menisci. Different suture techniques have been standardized. These include outside-in, inside-out, and all-inside techniques. The all-inside technique can be used to repair lesions of the posterior horn of the lateral meniscus. However, this technique presents important disadvantages, such as the necessity for an accessory portal and a high risk of neurovascular damage. For these reasons, we have developed a technique in which a suture hook and a shuttle relay are used to pass the suture wire through the meniscal lesion of the posterior horn of the lateral meniscus with an all-inside technique, without the use of accessory portals and cannulas, with a standard 30° arthroscopic camera.
Degenerative changes in articular cartilage, as a consequence of altered load transmission of the menisci, after a meniscal lesion and meniscectomy, comprise a well-known problem.1,2 In fact, menisci function as load-bearing and shock-absorbing components of the knee joint by increasing the surface area for load transmission. The menisci also take part in anterior-posterior stabilization of the knee joint, aiding in proprioception. Last but not least, menisci contribute to lubrication and nutrition of the articular cartilage.3
Lateral meniscectomy produces a more devastating effect, reducing the contact area by 40% to 50% and increasing the stress contact by 200% to 300% compared with a normal knee.4,5 For these reasons, the demand for lateral meniscal repair is growing. There are several well-known techniques for repairing the meniscus: inside out, outside in, all-inside meniscus fixator, and sutures. Every technique in use has different disadvantages.6 More challenging is the repair of a lesion of the posterior horn of the lateral meniscus.7
The anatomic relation among the popliteus tendon, popliteal artery, and tibial nerve within the popliteal space must always be kept in mind when one is performing meniscal repair of the posterior horn of the lateral meniscus. No less important, the common peroneal nerve lies posterior to the common tendon of the biceps and distally winds around the head of the fibula. Because of the anatomy of the posterolateral corner of the knee and because of its narrow joint space, some authors prefer an open approach for lateral posterior horn meniscal repair.8
All-inside suture techniques are also described in the literature for these kind of lesions, but many techniques are difficult to perform and require a posterolateral portal.9-11 An all-inside suture technique that takes advantage of the capacious posterolateral recess when the knee is flexed and provides only the use of anterior portals is also described in the literature.12 At our institution, we strongly attempt to repair all meniscal lesions when reparable (Table 1). Thus we describe our technique for posterior lateral meniscal horn repair with suture wires, using the anteromedial portal. It is a simple, reproducible, and less invasive technique, with no iatrogenic damage to any structures.
Table 1.
Indications, Contraindications, and Risks of All-Inside Suture Technique for Lateral Meniscal Lesions Using ConMed Linvatec Suture Hook
| Indications | Contraindications | Risks |
|---|---|---|
| Age 15-40 yr | Age >40 yr | Entrapment of suture hook |
| Red/red zone | White zone | Rupture of suture hook |
| Red/white zone | Chronic lesions | |
| Acute lesions |
Surgical Technique
The patient is placed in the supine position. Generally, spinal anesthesia is used and a tourniquet is applied. The knee is bent to 90° in a leg holder. Anteromedial and anterolateral portals are created, and the operation begins by introducing the arthroscopic camera through the anterolateral portal. The diagnostic part is conducted, and with the camera pointing toward the posterior horn of the lateral meniscus, the anteromedial portal is made with the use of a spinal needle. The lateral meniscal lesion is identified and evaluated with a probe. If it is reparable, the second part of the arthroscopy begins. The camera is maintained in the anterolateral portal, accessing the posterior recess of the knee with the leg in the figure-4 position (Video 1). During the entire procedure, the leg is maintained in the figure-4 position and the camera is never moved from the anterolateral portal. It is important to visualize the entire course of the popliteal tendon, which becomes easy with the camera in the anterolateral portal. At this point, a suture hook (ConMed Linvatec, Largo, FL)—a 45° right suture hook for a right knee or a 45° left suture hook for a left knee—is introduced through the anteromedial portal. The tip of the suture hook pierces the articular meniscal border of the lesion (Fig 1), passes through the lesion, and then enters the capsular border of the lesion and the posterior capsule, accessing the posterior access of the knee (Fig 2). The surgeon performs all these procedures while viewing perfectly the course of the popliteus tendon, checking that the stitch does not pass through it, in total safety. The shuttle relay (ConMed Linvatec) is let out from the suture hook (Fig 2), which is then retracted through the anteromedial portal by a suture grasper (Fig 3). The shuttle relay carries a No. 1 polyester thread, which will be the thread used for the suture. At this point, a suture retriever is introduced through the anteromedial portal to recover the suture thread from the posterior recess of the knee (Fig 4). In this way no entrapment of the threads happens in the portal soft tissues, so use of cannulas is not necessary. The suturing is performed through the anteromedial portal because it is easier to avoid damage to the femoral cartilage with the knot pusher. Thus the surgeon completes the vertical suture (Fig 5) using 5 half-stitches, easily and rapidly, being very careful that the knot falls in the posterior recess (Fig 6) so as not to poke the articular cartilage during knee movements. More knots can be made if necessary. The number of knots is determined based on the stability of the lesion after each knot is made. Generally, 1, 2, or a maximum of 3 knots are sufficient.
Fig 1.
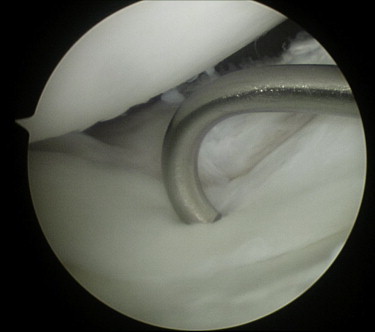
Lesion of the posterior horn of the lateral meniscus viewed from the camera positioned in the anterolateral portal of a right knee bent at 90° in a leg holder, with the leg in the figure-4 position. A 45° right suture hook pierces the meniscal border of the lesion, passes through the lesion, and then enters the capsular border of the lesion and the posterior capsule.
Fig 2.

Lesion of the posterior horn of the lateral meniscus viewed from the camera positioned in the anterolateral portal of a right knee bent at 90° in a leg holder with the leg in the figure-4 position. The shuttle relay is let out from the suture hook.
Fig 3.

Lesion of the posterior horn of the lateral meniscus viewed from the camera positioned in the anteromedial portal of a right knee bent at 90° in a leg holder, with the leg in the figure-4 position. The shuttle relay wire is grasped and recovered from the anterolateral portal after it has been carried out with a 45° suture hook through the lateral meniscal lesion.
Fig 4.

Lesion of the posterior horn of the lateral meniscus viewed from the camera positioned in the anteromedial portal of a right knee bent at 90° in a leg holder, with the leg in the figure-4 position. A suture retriever is introduced through the anterolateral portal to recover the suture thread (No. 1 polyester) from the posterior recess of the knee.
Fig 5.
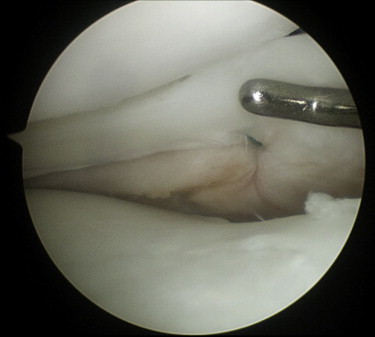
The inferior border of the lateral meniscus, showing a perfect vertical suture of lesion placed with an easy and safe all-inside technique. The view is from the camera positioned in the anteromedial portal of a right knee bent at 90° in a leg holder, with the leg in the figure-4 position.
Fig 6.

The final suture with the knot lying in the posterior recess of a lesion sutured with an easy and safe all-inside technique. The view is from the camera positioned in the anteromedial portal of a right knee bent at 90° in a leg holder, with the leg in the figure-4 position.
Discussion
Surgeons currently agree on the importance of preserving the menisci. The importance of the lateral meniscus in weight bearing, distribution of force, shock absorption, articular cartilage protection, proprioception, stabilization of the joint, and joint lubrication is well known.13 Different sutures techniques have been standardized. These include outside-in, inside-out, and all-inside techniques.6,7
The outside-in technique results are optimal for lesions of the body of the medial and lateral meniscus, whereas it is not appropriate for suture of the posterior horn of the lateral meniscus and medial meniscus.6,7 The inside-out technique can be used to repair these lesions of the posterior horn of the lateral meniscus. However, this technique presents important disadvantages, such as the necessity for an accessory portal and a high risk of neurovascular damage. The posterior horn of the lateral meniscus emits expansion to the Wrisberg ligament and popliteus tendon. Therefore painful tenodesis of the popliteus tendon frequently occurs during suturing of the posterior horn of the lateral meniscus. The strict relation with the popliteal artery and tibial nerve makes the inside-out technique quite difficult to perform. For these reasons, the all-inside technique has been developed and is more often used to repair lesions of the posterior horn of the lateral meniscus. Moreover, in this case, an accessory portal through the patellar tendon is necessary.9-12
Hence our technique has clear advantages (Table 2). First, no accessory portal is needed. It is interesting that during the operation, the camera is never moved from the anterolateral portal, which facilitates the suture steps. In addition, during the entire surgical procedure, it is possible to visualize the track of the suture hook to the posterior recess of the knee to ensure that it does not entrap the popliteus tendon; thus suturing can be performed in total safety. With the use of the suture hook and the shuttle relay, no cannulas are needed.
Table 2.
Tips, Pearls, and Pitfalls of All-Inside Suture Technique for Lateral Meniscal Lesions Using ConMed Linvatec Suture Hook
| Tips | Pearls | Pitfalls |
|---|---|---|
| Pass a 45° suture hook through the anterolateral portal. | No accessory portal is needed. | The small suture hook might not pass through the lesion to the posterior recess when dealing with a large meniscus. |
| Perfectly view the posterior recess and the popliteus tendon with the camera in the anteromedial portal. | The camera is never moved from the anteromedial portal. | Entrapment of the suture hook in the meniscal tissue can occur. |
| Use a suture retriever to recover the thread. | No cannulas are needed. | Rupture of the suture hook can occur. |
| Make knots in the posterior recess using a knot pusher. | No iatrogenic cartilage damage occurs. | |
| Standard 30° equipment is sufficient. |
Another important aspect is that vertical sutures are very easy to place with our technique. Vertical sutures are the gold standard for meniscal repair; these sutures sustain higher loading forces, lying as they do perpendicular to the longitudinal peripheral fibers of the menisci. The knot is in the posterior recess, and no damage to the articular cartilage occurs.
Last but not least, this technique can be carried out with standard arthroscopic equipment and with a 30° camera. It can be performed by most surgeons, even though good experience with shoulder suture technique is useful. It is not always easy to make the knot posteriorly so as not to damage the articular cartilage. This is definitely easier for an expert surgeon. In our opinion the technique is reliable, easy to reproduce, fast, less invasive, and not burdened by the complications of the other techniques.
One of the limitations of our technique is that the suture hooks used are sometimes too small and this makes access to the posterior recess difficult when the lesion occurs in a large meniscus. In all our cases we were able to place the suture. Moreover, it is important to use a sharp suture hook. In fact, because of the texture of the meniscus, if a sharp suture hook is not used, passing through the lesion can become troublesome. The only risk of this technique is that if it is not performed with shrewdness, the point of the suture hook can become entrapped in the meniscus and break. In no case did this occur in our patients.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
A lesion of the posterior horn of the lateral meniscus sutured with an easy and safe all-inside technique in the right knee of a 16-year-old boy. With the knee bent at 90° in a leg holder and with the leg in the figure-4 position, the technique is carried out with the surgeon viewing the posterior horn of the lateral meniscus through the anterolateral portal. A 45° right suture hook is then used to carry the shuttle relay and thus the Ethibond wire (Ethicon, Somerville, NJ) through the meniscal lesion to the posterior recess of the knee, where the knot is carefully tied, never moving the camera from the anterolateral portal.
References
- 1.Paxton E.S., Stock M.V., Brophy R.H. Meniscal repair versus partial meniscectomy: A systematic review comparing reoperation rates and clinical outcomes. Arthroscopy. 2011;27:1275–1288. doi: 10.1016/j.arthro.2011.03.088. [DOI] [PubMed] [Google Scholar]
- 2.Andersson-Molina H., Karlsson H., Rockborn P. Arthroscopic partial and total meniscectomy: A long-term follow-up study with matched controls. Arthroscopy. 2002;18:183–189. doi: 10.1053/jars.2002.30435. [DOI] [PubMed] [Google Scholar]
- 3.Buckwalter J.A., Amendola A., Clark C.R. Articular cartilage and meniscus: Biology, biomechanics and healing response. In: Scott W.N., editor. Surgery of the knee. Ed 4. Churchill Livingstone Elsevier; Philadelphia: 2006. pp. 307–328. [Google Scholar]
- 4.Fukubayashi T., Kurusawa H. The contact area and pressure distribution pattern of the knee. A study of normal and osteoarthritic knee joints. Acta Orthop Scand. 1980;51:871–879. doi: 10.3109/17453678008990887. [DOI] [PubMed] [Google Scholar]
- 5.Chatain F., Adeleine P., Neyret P. Societe Francaise d'Arthroscopie. A comparative study of medial versus lateral arthroscopic partial meniscectomy on stable knees: 10-year minimum follow-up. Arthroscopy. 2003;19:842–849. doi: 10.1016/s0749-8063(03)00735-7. [DOI] [PubMed] [Google Scholar]
- 6.Papalia R., Vasta S., Franceschi F., D'Adamio S., Maffulli N., Denaro V. Meniscal root tears: From basic science to ultimate surgery. Br Med Bull. 2013;106:91–115. doi: 10.1093/bmb/ldt002. [DOI] [PubMed] [Google Scholar]
- 7.Ayeni O., Peterson D., Chan K., Javidan A., Gandhi R. Suture repair versus arrow repair for symptomatic meniscus tears of the knee: A systematic review. J Knee Surg. 2012;25:397–402. doi: 10.1055/s-0032-1313752. [DOI] [PubMed] [Google Scholar]
- 8.Bach B.R., Jr., Bush-Joseph C. The surgical approach to lateral meniscal repair. Arthroscopy. 1992;8:269–273. doi: 10.1016/0749-8063(92)90050-l. [DOI] [PubMed] [Google Scholar]
- 9.Ahn J.H., Kim S.H., Yoo J.C., Wang J.H. All-inside suture technique using two posteromedial portals in a medial meniscus posterior horn tear. Arthroscopy. 2004;20:101–108. doi: 10.1016/j.arthro.2003.11.008. [DOI] [PubMed] [Google Scholar]
- 10.Ahn J.H., Oh I. Arthroscopic all-inside lateral meniscus suture using posterolateral portal. Arthroscopy. 2006;22:572.e1–572.e4. doi: 10.1016/j.arthro.2005.07.031. [DOI] [PubMed] [Google Scholar]
- 11.Morgan C.D. The all-inside meniscus repair. Arthroscopy. 1991;7:120–125. doi: 10.1016/0749-8063(91)90093-d. [DOI] [PubMed] [Google Scholar]
- 12.Espejo-Baena A., Figueroa-Mata A., Serrano-Fernández J., de la Torre-Solís F. All-inside suture technique using anterior portals in posterior horn tears of lateral meniscus. Arthroscopy. 2008;24:369.e1–369.e4. doi: 10.1016/j.arthro.2007.06.017. [DOI] [PubMed] [Google Scholar]
- 13.Renström P., Johnson R.J. Anatomy and biomechanics of the menisci. Clin Sports Med. 1990;9:523–538. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
A lesion of the posterior horn of the lateral meniscus sutured with an easy and safe all-inside technique in the right knee of a 16-year-old boy. With the knee bent at 90° in a leg holder and with the leg in the figure-4 position, the technique is carried out with the surgeon viewing the posterior horn of the lateral meniscus through the anterolateral portal. A 45° right suture hook is then used to carry the shuttle relay and thus the Ethibond wire (Ethicon, Somerville, NJ) through the meniscal lesion to the posterior recess of the knee, where the knot is carefully tied, never moving the camera from the anterolateral portal.