

Abstract
Tibial intercondylar eminence fractures that are displaced and non-reducible require open or arthroscopically assisted repair. Ideally, fracture reduction and fixation would be performed with a technique that has low morbidity, allows easy visualization and reduction, provides firm fixation, does not violate the proximal tibial physis, avoids metal hardware, and does not require a second procedure for implant removal. The suture bridge technique, used in the shoulder for rotator cuff tears and greater tuberosity fracture repair, has the ability to produce high contact pressures with rigid fixation. We describe an all-inside and all-epiphyseal arthroscopic suture bridge technique for tibial intercondylar eminence fracture repair performed with PushLock anchors (Arthrex, Naples, FL). One or 2 anchors preloaded with No. 2 FiberWire (Arthrex) are placed in the posterior fracture bed, followed by fracture reduction. The suture limbs are shuttled through and around the anterior cruciate ligament and over the fracture fragment in crossing fashion and are secured by use of additional anchors placed at the anteromedial and anterolateral fracture margin. The anchors are placed obliquely to avoid the proximal tibial physis in the pediatric population. Anatomic reduction and secure fixation allow more aggressive rehabilitation and faster restoration of joint function.
Tibial intercondylar eminence (spine) fractures occur most frequently in the pediatric and early adolescent ages but can also be seen in the adult population. In the pediatric population with open physes, this fracture is the equivalent of an anterior cruciate ligament (ACL) tear with the injury occurring at the relatively weak, incompletely ossified tibial epiphysis.1,2 This injury occurs from direct trauma associated with falls and accidents and also results from indirect, non-contact deceleration injury mechanisms in sports such as soccer and skiing.1
The original classification system described by Meyers and McKeever3 in 1959 establishes 3 types of fracture pattern. Type I is minimally displaced, type II has some proximal displacement of the anterior one-third of the spine but an intact posterior hinge, and type III is complete displacement of the fracture fragment from its bony bed. The type IV classification, later described by Zaricznyj,4 consists of a displaced and comminuted fracture.
Nondisplaced (type I) and mildly displaced type II fractures that are amenable to closed reduction are treated with cast immobilization. Displaced fractures frequently cannot achieve adequate closed reduction because of interposition of the intermeniscal ligament between the avulsed fragment and the tibial bony bed. Fracture displacement and disruption of the normal ACL tibial attachment block full knee extension and can cause symptoms of functional instability. Surgical fixation of tibial eminence fractures is indicated for type III and IV injuries, type II fractures that cannot be adequately reduced, and late displacement of type I injuries.1
The surgical treatment options have evolved from open techniques using wires, screws, or sutures to arthroscopic techniques, with the most common being arthroscopic screw or suture fixation.1 Previously described techniques for repair have drawbacks that include difficulty visualizing the fracture (open), difficulty visualizing the fracture reduction (open), drilling across the proximal tibial physis (open and arthroscopic), fixation placed across the proximal tibial physis (open and arthroscopic), use of a separate incision at the tibial metaphysis (open and arthroscopic), and an additional operation for hardware removal (open and arthroscopic).1
The use of suture bridge fixation for the repair of both bony and soft-tissue pathology has been extensively studied, primarily in the shoulder for repair of the rotator cuff and greater tuberosity fractures.5-8 This technique has also been described in knee surgery for fixation of femoral osteochondral defects.9,10 We describe an arthroscopic technique used since 2006 creating suture bridge fixation for treatment of displaced tibial spine fractures using PushLock anchors (Arthrex, Naples, FL). This technique can easily be modified depending on the specific fracture pattern, with variation in the number of anchors, the position of anchors, the number of suture limbs, and whether the suture limbs are passed through or adjacent to the ACL. Mann et al.11 have recently published a similar surgical technique using a suture mattress with 2 suture anchors and 2 knotless anchors, using a transpatellar portal. Our technique uses the accessory high medial and lateral portals, avoiding the transpatellar portal, which can be associated with tendon scarring, tendonitis, and rarely, tendon rupture.12,13
Surgical Technique
Arthroscopic tibial intercondylar eminence fracture repair is performed for patients with indicated fractures—types III and IV, non-reducible type II, and late displacement of type I injuries—after informed consent is received (Video 1). The surgery is performed as an outpatient procedure with the patient under general anesthesia. The patient is placed in the supine position. A standard setup with a lateral post or arthroscopic leg holder that allows for knee flexion is used. Use of lower limb exsanguination and a pneumatic tourniquet is useful but is left to the discretion of the surgeon. Standard anterolateral and anteromedial working portals are established, hemarthrosis is evacuated, and a complete diagnostic arthroscopy is performed. Treatment for associated meniscus tears or articular cartilage injury is addressed before the intercondylar eminence fracture. The ACL is carefully inspected because associated partial intrasubstance tears are not atypical and may result in plastic deformation with ligament laxity. The fracture fragment is probed and elevated, with the surgeon inspecting for comminution that might influence reduction or fixation. The tibia fracture bed is cleared of hematoma and fracture debris. If necessary, partial synovectomy, limited fat pad debridement, and placement of a traction suture around the intermeniscal ligament are performed to allow adequate visualization and facilitate reduction of the avulsed bone fragment into its bed (Fig 1).
Fig 1.
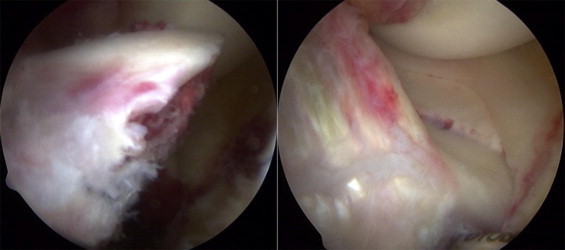
Intraoperative arthroscopic views from anterior portals of displaced tibial eminence fracture (left) and subsequent reduction (right).
Fracture fixation is performed with a polyetheretherketone or bioabsorbable 3.5-mm PushLock anchor (Arthrex) preloaded with 1 or 2 strands of No. 2 FiberWire (Arthrex). Accessory high anteromedial and anterolateral portals are created and positioned to allow access to the entire tibia fracture bed at a sufficient angle to keep the awl and anchors within the epiphysis, while avoiding scuffing of the femoral condyle articular cartilage. Disposable cannulas are used. For type III and IV fractures, the 3.5-mm PushLock awl is used to create a pilot hole at the edge of the posterior fracture bed and 1 double-loaded anchor or 2 single-loaded anchors are placed. A suture retriever is then used to shuttle the sutures in a crossing pattern through and around the ACL adjacent to the fracture fragment. The awl is again used to create pilot holes in the anteromedial and anterolateral tibia fracture bed. The fracture fragment is reduced and held in position with a probe. The 3.5-mm PushLock anchors are loaded with the free ends of the suture and inserted to create the suture bridge. If the fracture has an intact posterior hinge (type II), the posterior anchor step is omitted. Instead, a suture shuttle device is used to pass 2 No. 2 FiberWire sutures, placed in a locked cinch-knot loop, through the anterior ACL adjacent to the fracture fragment. The sutures are tensioned and anterior anchors are placed in the previously described fashion (Fig 2). The fracture reduction and fixation are re-examined arthroscopically, including inspection during flexion and extension of the knee. Fluoroscopic images or radiographs are obtained to confirm reduction of the fracture site (Fig 3). Table 1 shows surgical pearls for this technique.
Fig 2.
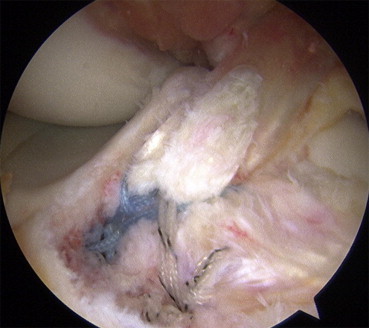
Intraoperative arthroscopic view from anterolateral portal of final suture bridge construct with suture limbs passing over surface of reduced tibial spine fracture.
Fig 3.
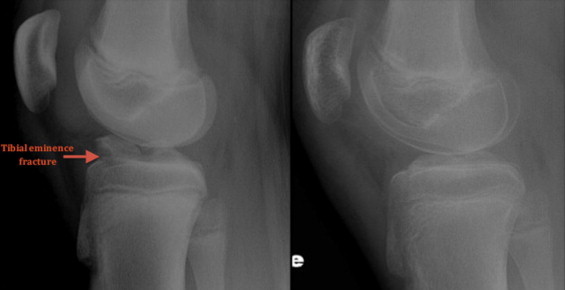
Comparison of preoperative (left) and postoperative (right) lateral radiographs of the knee in a pediatric patient with a displaced tibial eminence fracture.
Table 1.
Tips, Tricks, and Pitfalls Associated With Arthroscopic Suture Bridge Fixation of Tibial Intercondylar Eminence Fractures
| Tips and Tricks |
| 1. Debride the fracture bed to remove obstructions to fracture reduction. |
| 2. Attempt a trial reduction with a probe before fixation. |
| 3. Use a spinal needle to determine the appropriate position of the accessory high portals to access the fracture bed. |
| 4. Use percutaneous retraction sutures around the transverse meniscal ligament to improve visualization and allow fracture reduction. |
| 5. Place anchors at an angle to avoid physis in pediatric patients. |
| Pitfalls |
| 1. Assess for concomitant intrasubstance ACL tears, especially in the adult patient. |
Postoperative Management
Postoperatively, the knee is placed into a knee immobilizer. Determination of weight-bearing status and when to initiate range-of-motion exercises is made based on the stability of fixation and patient reliability. Typically, children remain immobilized and are allowed partial weight bearing using crutches for 2 weeks. Gradual range-of-motion and isometric quadriceps strength exercises with partial weight bearing are then begun. Closed-chain strengthening and full weight bearing begin 4 to 6 weeks postoperatively. Progression is made to nonimpact functional exercises. Reliable adolescent and adult patients begin immediate range of motion and strengthening using an accelerated ACL protocol. Return to normal activities including sports is allowed when the patient is asymptomatic, examination shows full range of motion and restoration of quadriceps strength, and the fracture is healed on radiographs.
Discussion
Suture bridge fixation has most extensively been studied for rotator cuff repair. First described by Park et al.5 as a “transosseous-equivalent” repair technique, a medial-row repair was performed with preservation of the suture limbs. Sutures were subsequently bridged over the footprint insertion and secured laterally with interference screws. This suture bridge fixation was reported to have significantly higher contact pressure between tendon and insertion, as well as improved ultimate failure load, when compared with double-row fixation.6,7
The use of suture bridge fixation has expanded beyond rotator cuff repair. Kim et al.8 reported fixation of greater tuberosity fractures using suture anchors medially through the intact rotator cuff, with suture limbs passed over the greater tuberosity fragment and secured laterally with PushLock anchors. In the knee, Bowers and Huffman9 reported the use of suture bridge fixation for traumatic osteochondral defects of the femoral condyle in 2 patients. At 12 months’ follow-up, 1 patient required a second-look arthroscopy for mechanical “clicking” whereas the second patient had full, painless range of motion. Lawrence et al.10 reported an all-arthroscopic suture bridge technique for fixation of chondral fragments in a pediatric patient using both bioabsorbable anchors and suture. They reported on a 12-year-old patient who was symptom free at 24 months’ follow-up.
The only other growth plate–sparing technique in the literature, described by Vega et al.,14 uses a single preloaded suture anchor placed in the epiphysis, with the suture limbs passed through the substance of the ACL and tied down with a sliding knot. Our suture bridge technique uses multiple anchors and 2 No. 2 FiberWire sutures to provide significant compression of the fracture fragment and rigid fixation with high pullout strength. Biomechanical testing has shown this technique to have a higher ultimate failure load than both screw and suture fixation.15
Potential postoperative complications are similar to those reported for other techniques, including loss of knee motion, fracture nonunion, fracture malunion, and persistent knee laxity.16,17 There is an increased cost of the operation with use of multiple anchors; however, we believe that this is offset by the potential for less operative time, rigid fracture fixation, improved healing, faster rehabilitation, and decreased need for future reoperation. This technique can also be technically challenging for surgeons performing a lower volume of arthroscopic procedures but offers no other disadvantages compared with an open fixation technique.
The all-inside, all-epiphyseal arthroscopic suture bridge technique for tibial intercondylar eminence fracture repair with PushLock anchors can be used in both the adult and pediatric patient. This procedure has low morbidity, allows easy visualization and reduction, provides firm fixation, can be effective in either comminuted or non-comminuted fractures, preserves the proximal tibial physis in pediatric patients, avoids metal hardware, and does not require a second procedure for implant removal. Postoperative rehabilitation can be accelerated within the restraints of fracture healing and patient reliability.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Intraoperative arthroscopic video of suture bridge fixation technique for tibial intercondylar eminence fractures. The title slide with author disclosures is shown at 0.0 seconds; patient background, 6.0 seconds; arthroscopic portals, 14.0 seconds; fracture bed preparation, 20.0 seconds; posterior anchor placement and suture passage, 38.0 seconds; and anteromedial and anterolateral PushLock anchor placement, 3 minutes 29.0 seconds.
References
- 1.LaFrance R.M., Giordano B., Goldblatt J., Voloshin I., Maloney M. Pediatric tibial eminence fractures: Evaluation and management. J Am Acad Orthop Surg. 2010;18:395–405. doi: 10.5435/00124635-201007000-00002. [DOI] [PubMed] [Google Scholar]
- 2.Perugia D., Basiglini L., Vadala A., Ferretti A. Clinical and radiological results of arthroscopically treated tibial spine fractures in childhood. Int Orthop. 2009;33:243–248. doi: 10.1007/s00264-008-0697-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Meyers M.H., McKeever F.M. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1959;41:209–222. [PubMed] [Google Scholar]
- 4.Zaricznyj B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59:1111–1114. [PubMed] [Google Scholar]
- 5.Park M.C., ElAttrache N.S., Ahmad C.S., Tibone J.E. “Transosseous-equivalent” rotator cuff repair technique. Arthroscopy. 2006;22:1360.e1–1360.e5. doi: 10.1016/j.arthro.2006.07.017. www.arthroscopyjournal.org Available online at. [DOI] [PubMed] [Google Scholar]
- 6.Park M.C., ElAttrache N.S., Tibone J.E., Ahmad C.S., Jun B.J., Lee T.Q. Part 1: Footprint contact characteristics for a transosseous-equivalent rotator cuff repair technique compared with a double-row repair technique. J Shoulder Elbow Surg. 2007;16:461–468. doi: 10.1016/j.jse.2006.09.010. [DOI] [PubMed] [Google Scholar]
- 7.Park M.C., Tibone J.E., ElAttrache N.S., Ahmad C.S., Jun B.J., Lee T.Q. Part II: Biomechanical assessment for a footprint-restoring transosseous-equivalent rotator cuff repair technique compared with a double-row repair technique. J Shoulder Elbow Surg. 2007;16:469–476. doi: 10.1016/j.jse.2006.09.011. [DOI] [PubMed] [Google Scholar]
- 8.Kim K.C., Rhee K.J., Shin H.D., Kim Y.M. Arthroscopic fixation for displaced greater tuberosity fracture using the suture-bridge technique. Arthroscopy. 2008;24:120.e1–120.e3. doi: 10.1016/j.arthro.2007.05.003. www.arthroscopyjournal.org Available online at. [DOI] [PubMed] [Google Scholar]
- 9.Bowers A.L., Huffman G.R. Suture bridge fixation of a femoral condyle traumatic osteochondral defect. Clin Orthop Relat Res. 2008;466:2276–2281. doi: 10.1007/s11999-008-0357-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lawrence J.T., Trivedi V., Ganley T.J. All arthroscopic suture-bridge fixation of a delaminated chondral fragment. Univ PA Orthop J. 2011;21:83–86. [Google Scholar]
- 11.Mann M.A., Desy N.M., Martineau P.A. A new procedure for tibial spine avulsion fracture fixation. Knee Surg Sports Traumatol Arthrosc. 2012;20:2395–2398. doi: 10.1007/s00167-012-1906-9. [DOI] [PubMed] [Google Scholar]
- 12.Fu F.H., Cohen S.B. SLACK Incorporated; Thorofare, NJ: 2008. Current concepts in ACL reconstruction. [Google Scholar]
- 13.McGinty J.B., Burkhart S.S., Jackson R.W., Johnson D.H., Richmond J.C. Lippincott Williams & Wilkins; Philadelphia, PA: 2003. Operative arthroscopy. [Google Scholar]
- 14.Vega J.R., Irribarra L.A., Baar A.K., Iniguez M., Salgado M., Gana N. Arthroscopic fixation of displaced tibial eminence fractures: A new growth plate-sparing method. Arthroscopy. 2008;24:1239–1243. doi: 10.1016/j.arthro.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 15.Sawyer G.A., Anderson B.C., Paller D., Schiller J., Eberson C.P., Hulstyn M. Biomechanical analysis of suture bridge fixation for tibial eminence fractures. Arthroscopy. 2012;28:1533–1539. doi: 10.1016/j.arthro.2012.02.020. [DOI] [PubMed] [Google Scholar]
- 16.Aderinto J., Walmsley P., Keating J.F. Fractures of the tibial spine: Epidemiology and outcome. Knee. 2008;15:164–167. doi: 10.1016/j.knee.2008.01.006. [DOI] [PubMed] [Google Scholar]
- 17.Mulhall K.J., Dowdall J., Grannell M., McCabe J.P. Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury. 1999;30:289–292. doi: 10.1016/s0020-1383(99)00084-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Intraoperative arthroscopic video of suture bridge fixation technique for tibial intercondylar eminence fractures. The title slide with author disclosures is shown at 0.0 seconds; patient background, 6.0 seconds; arthroscopic portals, 14.0 seconds; fracture bed preparation, 20.0 seconds; posterior anchor placement and suture passage, 38.0 seconds; and anteromedial and anterolateral PushLock anchor placement, 3 minutes 29.0 seconds.