

Abstract
Routine portal placement for the central compartment should be based on minimizing iatrogenic injury and maximizing access. Anchor placement for labral repair/refixation requires a more distal entry position to accomplish sufficient divergence to avoid perforating the articular surface of the acetabulum. If a standard portal for joint access is moved more distal, this can compromise its utility for addressing intra-articular pathology. In addition, it can be difficult to position this portal sufficiently distally to ensure adequate divergence. Moving the anchor away from the rim to avoid perforation, due to suboptimal portal placement, can result in nonanatomic labral repair. Thus a percutaneous anchor delivery system is advantageous in ensuring adequate divergence without compromising routine portal placement for the central compartment.
Portal placement for the central compartment has been well described.1-3 The 2 principal features are minimizing potential iatrogenic injury to the joint and maximizing access to the various regions of the central compartment. More recently, the merits of labral repair/refixation have been realized and have influenced portal positioning.4,5 A growing body of evidence supports the superiority of labral preservation over labral debridement.6-8
It is my contention that portal placement should continue to focus on maximizing utility to the joint, independent of anchor placement, which can be accomplished percutaneously from an ancillary site.
Surgical Technique
Three standard portals—anterior, anterolateral, and posterolateral—allow optimal access to the central compartment (Figs 1 and 2, Video 1, Table 1).1-3 Routine hip arthroscopy includes a survey from each site with the combinations of 30° and 70° arthroscopes. When a tear in the anterior or lateral quadrant is identified that is amenable to repair or refixation, the anterolateral portal is normally used as a viewing portal with the 70° arthroscope, and a ClearTrac cannula (Smith & Nephew, Andover, MA) is placed anteriorly as a working portal to manage sutures. The anchor is delivered percutaneously from a distally based site, halfway between the anterior and anterolateral portals, by use of the Osteoraptor system (Smith & Nephew, Andover, MA) (Figs 3 and 4).9 Prepositioning is performed with a 17-gauge spinal needle. A sufficiently distal site is selected to optimize divergence of the anchor from the subchondral surface of the acetabulum. The cannulated drill guide system is placed over a nitinol guidewire. The most medial anchor is placed first, with subsequent anchors placed moving closer to the arthroscope. The drill sleeve is positioned against the rim of the acetabulum. During drilling, careful observation is given to the adjacent articular surface of the acetabulum. Any signs of rippling or motion of the articular surface, in conjunction with the drilling process, indicate that the site is too close to the articular surface and should be repositioned. For primary repair of the labrum, the drill sleeve is placed immediately adjacent to the rim, on the articular side of the labrum. More commonly, labral refixation is performed in conjunction with acetabuloplasty, reshaping the bony rim. In this circumstance the drill sleeve is placed against the rim on the capsular side of the labrum. Positioning of the delivery system entry into the joint is identical in either case. Suture management to restore the labrum is variable depending on the size, morphology, and tear pattern of the labrum.
Fig 1.
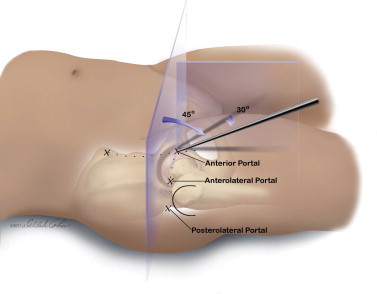
The anterior portal roughly coincides with the intersection of a sagittal line drawn distally from the anterior superior iliac spine and a transverse line across the superior margin of the greater trochanter. Generally, it is directed approximately 45° cephalad and 30° toward the midline. Depending on the patient's anatomy, one may choose to place this slightly more lateral and distal to properly intersect the joint. The anterolateral and posterolateral portals are positioned at the anterior and posterior borders of the trochanteric tip, converging slightly as they enter the joint. © J. W. Thomas Byrd.
Fig 2.
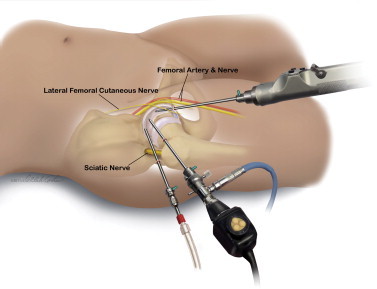
The relation of the major neurovascular structures to the 3 standard portals is shown. The femoral artery and nerve lie well medial to the anterior portal. The sciatic nerve lies posterior to the posterolateral portal. Small branches of the lateral femoral cutaneous nerve lie close to the anterior portal. Injury to these is avoided by use of proper technique in portal placement. The anterolateral portal is established first because it lies most centrally in the safe zone for arthroscopy. © J. W. Thomas Byrd.
Table 1.
Tips and Pearls
|
Fig 3.
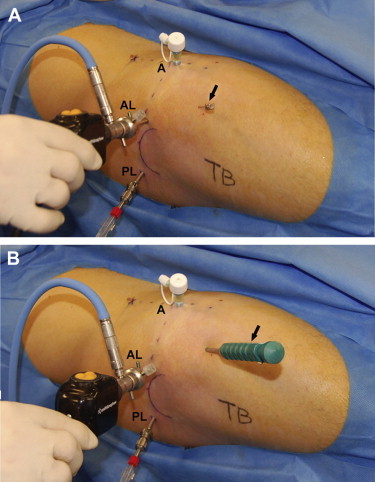
For this right hip, 3 standard portals are used for routine arthroscopy: anterior (A), anterolateral (AL), and posterolateral (PL). A large-diameter disposable cannula has been placed anteriorly for suture management. (A) A spinal needle has been prepositioned (arrow) for the anchor delivery system. It is midway between the anterior and anterolateral portals and sufficiently distal for divergence from the acetabular surface. (B) By use of the cannulated guide system and a nitinol wire, the anchor delivery system (arrow) has replaced the spinal needle. © J. W. Thomas Byrd.
Fig 4.
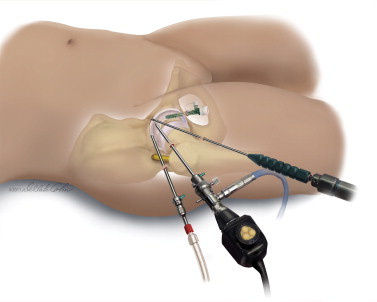
Drill sleeve placed against acetabular rim. © J. W. Thomas Byrd.
Discussion
The anterolateral portal is the most consistent site described by various authors for access to the central compartment.1,4 In our experience the traditional anterior portal, located at the site of intersection of a sagittal line distally through the anterior superior iliac spine and a transverse line across the tip of the trochanter, is usually modified slightly. This modification may be lateral and distal, as necessary, to reliably intersect the joint underneath the labrum at a cephalad angle. The most important feature is not to stray medially, which could place the femoral neurovascular structures at risk.
A more exaggerated lateral and distal modification of the anterior portal site is often proposed for the purposes of anchor placement.4 However, there are 2 caveats. First, the portal becomes less utilitarian for accessing the various regions of the central compartment. From its distal position, it is more difficult to clear the femoral head for reaching the medial regions of the joint. Second, this site is often still not distal enough to ensure adequate divergence to avoid perforating the articular surface of the acetabulum during anchor placement. To avoid perforation, the anchor is often placed slightly away from the rim of the acetabulum. Thus, when the labrum is repaired, it is not truly restored to the rim of the acetabulum. The labrum has shown excellent healing capacity; however, if its normal anatomy is not restored at the margin of the acetabulum, it is unlikely that its function will be restored either.10,11
The advantage of a percutaneous anchor delivery system is that a sufficiently distant site can be selected to accomplish the divergence necessary to avoid perforating the articular surface while one is placing the anchor adjacent to the acetabular rim.6 Even with an optimal distal position, placement of the anchor adjacent to the rim can still occasionally cause the drill to pass too close to the articular surface. If rippling or motion of the articular surface is identified during drilling, a new site, slightly further away from the rim, needs to be selected. Most labral tears amenable to restoration occur anterior and lateral. This percutaneous site serves well for tears from just below the equator anteriorly (9-o'clock/3-o'clock position) to just posterior to the 12-o'clock position superiorly. More inferior tears are uncommon, and once below the level of the acetabular fossa, there is little bone for anchor placement. Sometimes, the conventional anterior portal may serve better for placement inferiorly. As labral tears extend posterolaterally, the anterolateral portal is better used for anchor placement, with viewing from the anterior portal.
Footnotes
The author reports the following potential conflict of interest or source of funding: Smith & Nephew. Fee received. A3 Surgical. No fee received. Springer Medical Publishing.
Supplementary Data
Percutaneous anchor placement through a modified anterior portal site in a right hip. The portal is positioned equidistant between the anterior and anterolateral portals and sufficiently distal to achieve divergence of the anchor away from the articular surface of the acetabulum.
References
- 1.Byrd J.W.T. Hip arthroscopy utilizing the supine position. Arthroscopy. 1994;10:275–280. doi: 10.1016/s0749-8063(05)80111-2. [DOI] [PubMed] [Google Scholar]
- 2.Byrd J.W.T., Pappas J.N., Pedley M.J. Hip arthroscopy: An anatomic study of portal placement and relationship to the extra-articular structures. Arthroscopy. 1995;11:418–423. doi: 10.1016/0749-8063(95)90193-0. [DOI] [PubMed] [Google Scholar]
- 3.Byrd J.W.T. Routine arthroscopy and access: Central and peripheral compartments, iliopsoas bursa, peritrochanteric, and subgluteal spaces. In: Byrd J.W.T., editor. Operative hip arthroscopy. Ed 3. Springer; New York: 2013. pp. 131–160. [Google Scholar]
- 4.Ejnisman L., Philippon M.J., Lertwanich P. Acetabular labral tears: Diagnosis, repair and a method for labral reconstruction. Clin Sports Med. 2011;30:317–329. doi: 10.1016/j.csm.2010.12.006. [DOI] [PubMed] [Google Scholar]
- 5.Robertson W.J., Kelly B.T. The safe zone for hip arthroscopy: A cadaveric assessment of central, peripheral, and lateral compartment portal placement. Arthroscopy. 2008;24:1019–1026. doi: 10.1016/j.arthro.2008.05.008. [DOI] [PubMed] [Google Scholar]
- 6.Philippon M.J., Briggs K.K., Yen Y.-M., Kuppersmith D.A. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction. J Bone Joint Surg Br. 2009;91:16–23. doi: 10.1302/0301-620X.91B1.21329. [DOI] [PubMed] [Google Scholar]
- 7.Larson C.M., Giveans M.R. Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement. Arthroscopy. 2009;25:369–376. doi: 10.1016/j.arthro.2008.12.014. [DOI] [PubMed] [Google Scholar]
- 8.Krych A.J., Thompson M., Knutson Z., Scoon J., Coleman S.H. Arthroscopic labral repair versus selective labral debridement in female patients with femoroacetabular impingement: A prospective randomized study. Arthroscopy. 2013;29:46–53. doi: 10.1016/j.arthro.2012.07.011. [DOI] [PubMed] [Google Scholar]
- 9.Byrd J.W.T. Labral management: An overview. In: Byrd J.W.T., editor. Operative hip arthroscopy. Ed 3. Springer; New York: 2013. pp. 171–184. [Google Scholar]
- 10.Philippon M.J., Arnoczky S.P., Torrie A. Arthroscopic repair of the acetabular labrum: A histologic assessment of healing in an ovine model. Arthroscopy. 2007;23:375–380. doi: 10.1016/j.arthro.2007.01.017. [DOI] [PubMed] [Google Scholar]
- 11.Audenaert E.A., Dhollander A.A., Forsyth R.G., Corten K., Verbruggen G., Pattyn C. Histologic assessment of acetabular labrum healing. Arthroscopy. 2012;28:1784–1789. doi: 10.1016/j.arthro.2012.06.012. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Percutaneous anchor placement through a modified anterior portal site in a right hip. The portal is positioned equidistant between the anterior and anterolateral portals and sufficiently distal to achieve divergence of the anchor away from the articular surface of the acetabulum.