

Abstract
Introduction
The history of HIV/AIDS in Romania is different compared to the rest of the world. Here, the vast majority of HIV-positive patients have been infected since infancy and have been receiving HAART treatment for at least ten years. This situation is a unique environment to check for long-term cardiac involvement in HIV-positive patients with a long evolution of the infection.
Methods
A group of 40 HIV-positive patients were randomly selected to undergo an echocardiogram to check for cardiac involvement. Data collection took place at the National Institute for Infectious Diseases “Prof.Dr. Matei Balş” in Bucharest, Romania, from September 2011 to February 2012. Patients were examined and compared based on cardiovascular risk factors and disease risk factors described in field literature, including: age, gender, blood pressure, lipid profile, glucose, HbA1c, lifestyle habits, time from infection, duration of treatment and drug class use.
Results
The median age of patients was 23, with a mean time from infection of 20.85 years and a duration of treatment of 15.9 years. Out of the 40 patients included in the study, 15 (37.5%) had cardiac involvement such as hyperkinetic syndrome, hypertrophy, atheroma, pulmonary hypertension or overlapping syndromes. The main risk factors were: male gender (OR 3.187, 90%CI 1.038-9.779), high cholesterol (>200 mg/dL) or smoking (OR 2.538, 90%CI 0.789-8.163), with a high risk for cardiac involvement in patients that were smokers and also had high levels of cholesterol (OR 5.75, 90%CI 1.263-26.169).
Conclusion
An important aspect of this study is that both major risk factors identified are modifiable to an extent, and while cholesterol levels can be controlled with lipid-lowering medication, smoking can be stopped with or without replacement therapy. We need to stress on the importance of smoke-reducing policies and, particularly, encouraging young patients to not start smoking.
Keywords: HIV, Cardiac involvement, HAART
Introduction
With approximately 34 million people living with HIV/AIDS worldwide and 1.4 million in Eastern Europe plus Central Asia,1,2 the Joint United Nations Programme on HIV/AIDS (UNAIDS) reports that roughly half of them are aware of their HIV status.3 At the end of 2012 in Romania there were 9,475 HIV-positive patients under active medical surveillance, of which 237 (2.5%) had ages below 14 years, most patients with ages ranging from 20 to 24 years old.4
Prior to the highly active antiretroviral therapy (HAART) era, autopsy studies found myocarditis in HIV-positive patients in varying percentages, from 9% to 52%, with an average of 33%.5 Following the introduction of HAART, it has become apparent that treatment dramatically reduces morbidity, mortality and hospitalization rates, and prolongs the life of HIV-positive patients.6 Antiretroviral (ARV) therapy also plays a role in preventing opportunistic infections and thus has been shown to lower the incidence of myocarditis, leading to a decrease in HIV-associated cardiomyopathy with about 30% in developed countries.7 On the other hand, in developing countries the median prevalence of HIV-associated cardiomyopathy has increased with about 32%, in conjunction with a limited availability of HAART.8
An increase in the life expectancy of HIV-positive patients associated a shift in the spectrum of health problems, with emphasis on non-infectious comorbidities, lifestyle-related and ageing issues, such as: arterial hypertension, metabolic changes (hyperglycemia, hyper-lipidemia),9 accelerated atherosclerosis, including but not limited to coronary artery disease.10
The history of HIV/AIDS in Romania is different compared to the rest of the world,11 due to the epidemic that occurred in the end of the '80s, when a large number of patients were infected with clade F HIV,12 mostly children and infants.13 The number of newly infected adults during those years was low, with a subsequent increase afterwards mainly by heterosexual contact. The children and infants infected in the '80s are today young adults who represent the main population treated with HAART.
This particular situation gave rise to a special population in which the majority of patients, infected with HIV since infancy, have received ART for at least ten years through governmental programs.14 This created a unique environment to check for long-term cardiac involvement due to either the treatment or the disease.
Methods
We performed a study to determine the prevalence of cardiac involvement in HIV-positive patients monitored at the National Institute for Infectious Diseases “Prof.Dr. Matei Balş” in Bucharest, Romania, and to detect and analyze the risk factors for these cardiac abnormalities. A group of 40 HIV-positive patients were randomly selected to undergo an echocardiogram (Vivid S6 ultrasound, GE Healthcare, USA), currently considered an useful test for providing a semi-quantitative assessment of left ventricular size and function.15
Data collection took place at the National Institute for Infectious Diseases “Prof.Dr. Matei Balş” in Bucharest, Romania, from September 2011 to February 2012. The Institute is a national HIV center and coordinates with the other eight regional centers in Romania.
Eligibility criteria included: adult patients, living with HIV for at least ten years, under current antiretroviral treatment after having received at least ten years of HAART. Exclusion criteria were: history of injecting drug use, coinfections such as hepatitis, endocarditis, history of sexually transmitted diseases with potential cardiac implications (e.g. syphilis),16 pregnancy during or one year prior to the echocardiogram exam. All patients were informed on the nature of the study, agreed be included in the study group, and signed informed consent forms.
Patients were examined and compared based on cardiovascular risk factors and disease risk factors described in field literature, including: age >30 years old; gender (male, female); blood pressure (normal 120/80); lipid profile: cholesterol (normal <200 mg/dL), high-density lipoprotein (HDL, normal ≥40 mg/dL, low <40 mg/dL), low-density lipoprotein (LDL, normal <100 mg/dL, borderline 100-129 mg/dL, high >130 mg/dL), triglycerides (TG, high >200 mg/dL); glucose (with or without diabetes) and HbA1c (normal 4-5.9 mg/dL); lifestyle habits such as smoking (above ten pack-years) and alcohol intake (at least one alcoholic drink per day); time from infection (10-14 years, 15-20 years, 21-25 years), duration of treatment (10-14 years, 15-20 years) and drug class use (non-nucleoside reverse-transcriptase inhibitors – NNRTI – and non-nucleoside reverse-transcriptase inhibitors/ protease inhibitors – NNRTI/PI).
Data regarding treatment duration and choice of ARVs were matched with the national database and interpreted according to ARV classes: PI, NNRTI, NRTI (nucleoside reverse-transcriptase inhibitors), integrase inhibitor, CCR5-receptor antagonist, fusion inhibitor.17
The cardiovascular risk was calculated based on the Framingham Risk Score.18 To compare whether the incidence of cardiac abnormalities in our study group was significantly different from the EU baseline, we used the Z-test for proportions (and verified using binomial distribution as our sample size was relatively low). For each risk factor we calculated the odds ratio (OR) and the 90% confidence interval (90%CI).
Results
The study included 40 patients, all with ages over 21 years old. The median age of patients was 23. The mean (± standard deviation, SD) time from infection was 20.85 (±1.5) years. The mean (±SD) duration of treatment was 15.9 (±1) years. All patients were on classical HAART regimens with PIs, NRTIs, NNRTIs; none of the patients received integrase inhibitor, CCR5-receptor antagonist or fusion inhibitor.
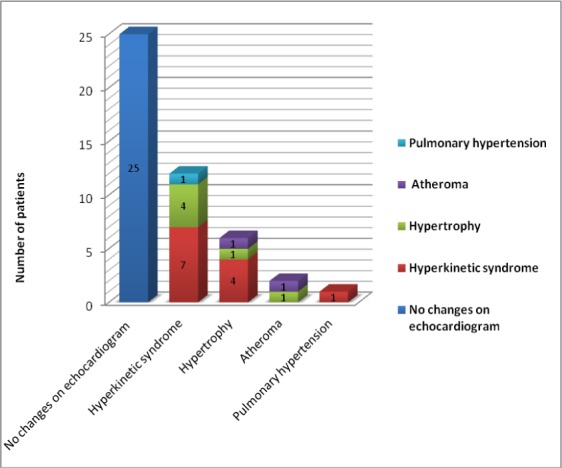
Out of the 40 patients in the study, a cumulated 15 (37.5%) had cardiac abnormalities (figure 1), compared to other non-cumulated percentages in developed countries with access to HAART: 14.5% for left ventricle hypokinesia19 or 8% for dilated cardiomyopathy20 (p<0.001). Most of the patients in this study displayed more than one cardiac abnormality, with a high prevalence of the hyperkinetic syndrome (110 beats per minute) and hypertrophy (left ventricle 56 mm).
Figure 1. Graphic display of cardiac abnormalities identified in the study.
After identifying the patients with cardiac abnormalities, the study group was divided into two smaller groups: without cardiac abnormalities (WOCA) and with cardiac abnormalities (WCA) in order to permit a comparison based on the data collected.
Table 1 presents the cardiac risk factors assessed, including descriptive data for patients and results of relevant laboratory tests.
Table 1. Incidences by risk factors.
| Characteristic | Interpretation | WCA (n=15) | WOCA (n=25) | All patients (n=40) |
| Gender | Female | 6 | 17 | 23 |
| Male | 9 | 8 | 17 | |
| Age | <30 | 11 | 18 | 29 |
| >30 | 4 | 7 | 11 | |
| Cholesterol | Normal | 9 | 20 | 29 |
| High | 6 | 5 | 11 | |
| LDL | Optimal | 7 | 14 | 21 |
| Borderline | 4 | 6 | 10 | |
| High | 4 | 5 | 9 | |
| HDL | Low | 3 | 5 | 8 |
| Normal | 6 | 12 | 18 | |
| High | 6 | 8 | 14 | |
| TG | Normal | 11 | 20 | 31 |
| High | 4 | 5 | 9 | |
| Serum glucose | <100 | 15 | 25 | 40 |
| HbA1c | 4-5.9 | 15 | 25 | 40 |
| Blood pressure | <120/80 | 15 | 25 | 40 |
| Framingham score | At risk (above 10%) | 1 | 1 | 2 |
| Not at significant risk (under 10%) | 14 | 24 | 38 | |
| Smoking | Yes (10 pack-years) | 11 | 13 | 24 |
| No (below 10 pack-years) | 4 | 12 | 16 | |
| Alcohol use | Yes | 7 | 14 | 21 |
| No | 8 | 11 | 19 | |
| Time from infection | 10-14 years | 2 | 2 | 4 |
| 15-20 years | 1 | 4 | 5 | |
| 21-25 years | 12 | 19 | 31 | |
| Duration of treatment | 10-14 years | 3 | 2 | 5 |
| 15-20 years | 12 | 23 | 35 | |
| Treatment regimen | NNRTI | 3 | 1 | 4 |
| NNRTI/PI | 12 | 24 | 36 |
A multivariate analysis (table 2) identified the main risk factors for developing cardiac abnormalities (taken as a whole) as: male gender (OR 3.187, 90%CI 1.038-9.779), high cholesterol (>200 mg/dL) or smoking (OR 2.538, 90%CI 0.789-8.163), with a high risk for cardiac involvement in patients that were smokers and had high levels of cholesterol (OR 5.75, 90%CI 1.263-26.169). The variance had a low distribution making the results accurate for the number of patients in the study.
Table 2. Multivariate analysis of risk factors for cardiac involvement in HIV-positive patients.
| Risk factor | Odds Ratio | 90%CI |
| Cholesterol AND smoking | 5.75 | 1.263-26.169 |
| Gender (male) | 3.187 | 1.038-9.779 |
| Cholesterol (>200 mg/dL) | 2.666 | 0.804-8.842 |
| Smoking (above 10 packs-year) | 2.538 | 0.789-8.163 |
| Low HDL (<40 mg/dL) | 1.416 | 0.461-4.346 |
| High LDL (>130 mg/dL) | 1.454 | 0.409-5.170 |
| High TG (>200 mg/dL) | 1.454 | 0.409-5.170 |
| Age >30 years | 0.935 | 0.278-3.141 |
| Alcohol consumption | 0.687 | 0.232-2.028 |
| Duration of ARV therapy (>15 years) | 0.347 | 0.069-1.751 |
Regarding the time from infection, duration of treatment and drugs used, the data did not yield any significant result (as can be seen in table 2).
The Framingham score did not yield significant results since only two patients were in the risk range according to the score (table 1), one patient with cardiac abnormalities and one without cardiac abnormalities.
Discussion
The results of this study did not entirely come as a surprise, but they are interesting particularly due to the fact that both major risk factors identified are modifiable to an extent, and while cholesterol levels can be controlled with lipid-lowering medication, smoking can be stopped with or without nicotine-replacement therapy. As such, we need to stress on the importance of smoke-reducing policies, ensuring smoke-free environment, providing relevant counseling and more importantly, encouraging young patients to not start smoking, since it is said that the best treatment option is prophylaxis.
In HIV-positive patients, the exact mechanisms whereby smoking increases the risk of cardiovascular events are yet to be determined,21 but endothelial damage appears to be the cornerstone of heart disease in HIV22 and it has become apparent that the effect of smoking can augment the damage produced by the virus itself, the immune response of the host,23 or by potential toxicity of older drugs used in the treatment of HIV infection.24
Furthermore, recent studies have shown that the population-attributable risk of death associated with smoking is higher (61.5%) among HIV-positive patients compared to controls (34.2%), postulating that in this particular category or patients, more life-years are lost to smoking than to HIV.25
Despite an implementation of policies for reducing tobacco use, smoking continues to be a major issue in Romania. Having signed the World Health Organization (WHO) Framework Convention on Tobacco Control in 2004, with subsequent ratification in 2006, Romania has since made it on the list of highest achieving countries for monitoring the prevalence of tobacco use, tobacco dependence treatment and raising taxes on tobacco. With implemented cessation programs (national quit line, nicotine replacement therapy and cost-covered cessation services), health warnings on cigarette packages, some mass media campaigns, and advertising bans on national televisions, radio, print media and some forms of direct/indirect advertising, the prevalence of smoking remained borderline high, at 29% by the end of 2011, comparable to the percentage reported by the global adult tobacco use survey, conducted between 2008-2010, which reported prevalence values ranging from 16% to 43%.26
An interesting recent study has shown that the prevalence of smoking may be up to three times higher in HIV-positive patients than in the general population,27 which is an alarming finding, particularly given the high risk for morbidity in this category of patients. The risk of chronic obstructive pulmonary disease28 and that of local infections due to a baseline suppressive lung inflammatory environment29 have been clearly described, but the cardiac involvement is still to be determined.
Given that a 23 year-old should not have any kind of cardiac pathology (except for congenital issues), it is potentially alarming that in our study 15 out of 40 patients (37.5%) presented cardiac abnormalities. This high prevalence of cardiac involvement could be due to the occurrence of HIV infection at young ages, or to cumulative risk factors, lifestyle and heath habits.
The abnormalities identified echographically in this group of patients were mild, and did not require specialty treatment for the time being. However, there is no way of knowing how the cardiac involvement will develop in each patient, and it would be very interesting to return to this group of patients in 5-10 years time, to check for differences compared to the baseline data derived from this study.
A recent study30 evaluated cardiac function through echocardiography in 53 naïve HIV positive patients without clinical evidence of cardiovascular disease, revealing a higher prevalence (36% in HIV patients vs. 9% in healthy controls) of diastolic left ventricular dysfunction (36% in HIV patients vs. 9% in healthy controls), leading to the conclusion that subclinical cardiac abnormalities do appear in early stages of HIV infection, independent of ARV therapy.30 Larger studies, observing clinical endpoints rather than echocardiographic changes, have shown that certain ARV classes (such as protease inhibitors) can be associated with an increased risk of myocardial infarction, explained in part by dyslipidemia.31 In our study, HAART duration was not associated with an increase in cardiac abnormalities, nor was a particular ARV class, and this may be due to the fact that we did not look at clinical endpoints, but rather at morphological and functional changes in the heart.
Study limitations
The group of patients was relatively small (only 40 patients), which lowered the statistical significance of the results and did not allow for further statistic analyses. Some of the patients in the study were born in orphan homes or had been given to one at a very young age and thus an important potential risk factor, family history for cardiac involvement, could not be obtained in all cases.
Healthcare implications
In conclusion, the main question refers to the progression of the cardiac involvement identified in patients in this study: will it become more severe and potentially worsen with time? And if so, how soon are significant changes to be expected? In order to be able to provide an answer to these questions and to offer the best care to these patients, specialty monitoring by a cardiologist will be provided to our best effort, to determine if, or when, treatment is in order. Also, we would consider extending this study to determine whether the prevalence of cardiac involvement is indeed this high and, if confirmed, to determine the age at which an echocardiogram should be considered in routine screening for HIV-positive patients.
Smoking cessation programs should be offered to HIV-positive patients, together with public health education programs. Cholesterol issues should also be addressed with some simple lifestyle changes and with better nutrition. Both the physician and the patient should understand that lifestyle and healthy habits are important factors to the success of the treatment.
Footnotes
Conflicts of interest: All authors – none to declare.
ED performed the study, collected the data, interpreted the results and drafted the manuscript, DY performed the statistic analysis and interpreted the results, BM performed the cardiac assessment pivotal to the study, ASC drafted and supervised the study. All authors contributed significantly to the manuscript.
References
- 1.UNAIDS Report on the global AIDS epidemic 2012. [Accessed on: December 29, 2012]. Available at: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/20121120_UNAIDS_Global_Report_2012_en.pdf.
- 2.Dragović G, Jevtović D. Highlights from the 13th European AIDS Conference (EACS) GERMS. 2011;1(1):9–11. doi: 10.11599/germs.2012.1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.UNAIDS World AIDS Day Report 2012. [Accessed on: December 29, 2012]. Available at: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/JC2434_WorldAIDSday_results_en.pdf.
- 4.Compartment for monitoring and evaluating HIV/AIDS infection in Romania. National Institute for Infectious Diseases “Prof.Dr. Matei Balş”. HIV/AIDS infection at December 1, 2012. [Accessed on: December 17, 2012]. Available at: http://www.cnlas.ro/images/doc/1dec2012.pdf.
- 5.Cheitlin MD. Cardiac involvement in HIV-infected patients. In: UpToDate, Basow, DS (Ed), editor. UpToDate; Waltham, MA: 2013. [Google Scholar]
- 6.May MT, Sterne JA, Costagliola D, Sabin CA, Phillips AN, Justice AC, et al. HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis. Lancet. 2006;9534(368):451–8. doi: 10.1016/S0140-6736(06)69152-6. [DOI] [PubMed] [Google Scholar]
- 7.Barbaro G. Immune dysfunction and immunotherapy in heart disease. In: Watson R, Larson D, editors. Blackwell Futura; 2007. (Ed) [Google Scholar]
- 8.Barbaro G, Barbarini G. Human immunodeficiency virus & cardiovascular risk. Indian J Med Res. 2011;134(6):898–903. doi: 10.4103/0971-5916.92634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Streinu-Cercel A, Ion DA, Chivu LI, Chivu RD. [Lipodystrophy syndrome in HIV-infected patients. Clinical and diagnostic features] Rev Med Chir Soc Med Nat Iasi. 2006;110(3):521–5. [PubMed] [Google Scholar]
- 10.Guaraldi G. Evolving approaches and resources for clinical practice in the management of HIV infection in the HAART era. GERMS. 2011;1(1):6–8. doi: 10.11599/germs.2012.1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stanojević M, Jevtović D, Dragović G. Predicting HIV treatment response in Romania – Comment. GERMS. 2012;2(1):23–4. doi: 10.11599/germs.2012.1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Revell A, Ene L, Duiculescu D, Wang D, Youle M, Pozniak A, et al. The use of computational models to predict response to HIV therapy for clinical cases in Romania. GERMS. 2012;2(1):6–11. doi: 10.11599/germs.2012.1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Revell A, Wang D, Alvarez-Uria G, Streinu-Cercel A, Ene L, Wensing A, et al. Computational models that predict response to HIV therapy can reduce virological failure and therapy costs in resource-limited settings. J Int AIDS Soc. 2012;15(6):18114. [Google Scholar]
- 14.Aramă V, Tilişcan C, Ion D, Mihăilescu R, Munteanu D, Streinu-Cercel A, et al. Serum adipokines and HIV viral replication in patients undergoing antiretroviral therapy. GERMS. 2012;2(1):12–7. doi: 10.11599/germs.2012.1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J. Harrison's Principles of Internal Medicine, 18th Edition. McGraw-Hill; 2011. Chapter 234. Heart Failure and Cor Pulmonale. [Google Scholar]
- 16.Streinu-Cercel O. AIDS and Sexually Transmitted Infections in Africa. GERMS. 2012;2(1):5. doi: 10.11599/germs.2012.1006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Streinu-Cercel A, de Gorgolas M, Muller M, Portilla J, Rugina S, Bocher W, et al. Switching from a toxicity-causing antiretroviral to enfuvirtide in patients with HIV: the SWITCH TOX study. HIV Clin Trials. 2008;9(6):375–86. doi: 10.1310/hct0906-375. [DOI] [PubMed] [Google Scholar]
- 18.Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97(18):1837–47. doi: 10.1161/01.cir.97.18.1837. [DOI] [PubMed] [Google Scholar]
- 19.Herskowitz A, Vlahov D, Willoughby S, al e. Prevalence and incidence of left ventricular dysfunction in patients with human immunodeficiency virus infection. Am J Cardiol. 1993;71(11):955–8. doi: 10.1016/0002-9149(93)90913-w. [DOI] [PubMed] [Google Scholar]
- 20.Barbaro G, Di Lorenzo G, Grisorio B, Barbarini G. Incidence of dilated cardiomyopathy and detection of HIV in myocardial cells of HIV-positive patients. Gruppo Italiano per lo Studio Cardiologico dei Pazienti Affetti da AIDS. N Engl J Med. 1998;339(16):1093–9. doi: 10.1056/NEJM199810153391601. [DOI] [PubMed] [Google Scholar]
- 21.Sen S, Rabinstein AA, Elkind MS, Powers WJ. Recent developments regarding human immunodeficiency virus infection and stroke. Cerebrovasc Dis. 2012;33(3):209–18. doi: 10.1159/000335300. [DOI] [PubMed] [Google Scholar]
- 22.Lopez M, Vispo E, San Roman J, Herrero D, Peris A, Corral A, et al. Short communication high risk of endothelial dysfunction in HIV individuals may result from deregulation of circulating endothelial cells and endothelial progenitor cells. AIDS Res Hum Retroviruses. 2012;28(7):656–9. doi: 10.1089/AID.2011.0152. [DOI] [PubMed] [Google Scholar]
- 23.Osakwe CE, Bleotu C, Chifiriuc MC, Grancea C, Otelea D, Paraschiv S, et al. TH1/TH2 cytokine levels as an indicator for disease progression in human immunodeficiency virus type 1 infection and response to antiretroviral therapy. Roum Arch Microbiol Immunol. 2010;69(1):24–34. [PubMed] [Google Scholar]
- 24.Streinu-Cercel A. Nanoparticles. GERMS. 2012;2(3):90. doi: 10.11599/germs.2012.1017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Helleberg M, Afzal S, Kronborg G, Larsen CS, Pedersen G, Pedersen C, et al. Mortality Attributable to Smoking Among HIV-1-Infected Individuals: A Nationwide, Population-Based Cohort Study. Clin Infect Dis. 2012 doi: 10.1093/cid/cis933. [DOI] [PubMed] [Google Scholar]
- 26.WHO Report on the global tobacco epidemic, 2011. Warning about the dangers of tobacco. [Accessed on: June 19, 2012]. Available at: http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf.
- 27.Tesoriero JM, Gieryic SM, Carrascal A, Lavigne HE. Smoking among HIV positive New Yorkers: prevalence, frequency, and opportunities for cessation. AIDS Behav. 2010;14(4):824–35. doi: 10.1007/s10461-008-9449-2. [DOI] [PubMed] [Google Scholar]
- 28.Madeddu G, Fois AG, Calia GM, Babudieri S, Soddu V, Becciu F, et al. Chronic obstructive pulmonary disease: an emerging comorbidity in HIV-infected patients in the HAART era? Infection. 2012 doi: 10.1007/s15010-012-0330-x. [DOI] [PubMed] [Google Scholar]
- 29.Wewers MD, Diaz PT, Wewers ME, Lowe MP, Nagaraja HN, Clanton TL. Cigarette smoking in HIV infection induces a suppressive inflammatory environment in the lung. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1543–9. doi: 10.1164/ajrccm.158.5.9802035. [DOI] [PubMed] [Google Scholar]
- 30.Oliviero U, Bonadies G, Bosso G, Foggia M, Apuzzi V, Cotugno M, et al. Impaired diastolic function in naive untreated human immunodeficiency virus infected patients. World J Cardiol. 2010;2(4):98–103. doi: 10.4330/wjc.v2.i4.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sabin CA, Worm SW, Weber R, Reiss P, El-Sadr W, Dabis F, et al. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaboration. Lancet. 2008;9622(371):1417–26. doi: 10.1016/S0140-6736(08)60423-7. [DOI] [PMC free article] [PubMed] [Google Scholar]