

Abstract
Community-based studies are required to accurately describe the supportive services needed by people with multiple sclerosis (MS). Characteristics that influence (or result from) care-seeking may introduce bias into other types of studies. The Participation and Activity Limitation Survey (PALS) was a post-census survey conducted by Statistics Canada in association with a 2006 national census. The PALS collected data from a sample of 22,513 respondents having health-related impairments according to their census forms. The survey collected self-reported diagnostic data and obtained ratings for items assessing impairment as well as perceived met and unmet needs for care and support. It identified 245 individuals with MS, leading to an estimated (weighted) population prevalence of 0.2% (200 per 100,000). As expected, those with MS reported more-severe health problems than did those with other types of disability, particularly in the areas of mobility, dexterity, and cognition; they were also more likely to report having multiple caregivers. People with MS also reported more unmet health-care needs than did those with other forms of disability, particularly with respect to meal preparation, housework, shopping, and chores. Despite their more negative health status and greater reliance on caregivers, people with MS reported participation in society comparable to that of people without MS. Thus, people with MS report greater needs than do people with other forms of health-related disability and utilize supportive services more often. However, they also report higher levels of unmet needs. The substantial needs of people with MS are only partially addressed by existing services.
Multiple sclerosis (MS) is the most common disabling neurologic condition among young people,1,2 but the condition is sufficiently rare that population-based studies are difficult to carry out. Only a few studies have used probability-based general population samples to examine use of health-care services and perceived unmet needs in people with MS. One was a Canadian study based on data from the Canadian Community Health Survey. People with MS were found to use more services, but also to report greater unmet health-care needs.3 Another was the Stockholm MS Study, which found a high frequency (70%) of reliance on others for activities of daily living.4 The Stockholm study identified several specific problem areas for people with MS: heavy housework, shopping, and cooking. Transportation outside the home also figured prominently among areas of concern.5
An opportunity to examine health status, care needs, and unmet needs in a community sample with MS arises from a Canadian post-census survey called the Participation and Activity Limitation Survey (PALS).6 This survey is based on a probability sample of respondents reporting health-related impairments during a national census conducted in 2006. Conditions responsible for impairment were recorded in the data set, allowing disease-specific analysis. The survey's linkages to a national census allow some population-based inferences to be made. In this analysis, we were interested in examining health status, the use of aids and supports, perceived unmet needs, and participation in society by people with MS in Canada.
Methods
In a Canadian census conducted in 2006, 80% of households received a short-form questionnaire that contained eight basic questions. The remaining, randomly sampled 20% received a more detailed questionnaire containing 61 questions (the census “long form”).7 A copy of the 2006 census long form may be found on the Statistics Canada website.8 Questions on the long form were usually answered by a single household informant providing data on all residents of the household.
The long form contained two questions concerning health-related impairments: 1) Does this person have any difficulty hearing, seeing, communicating, walking, climbing stairs, bending, learning, or doing any similar activities? 2) Does a physical condition or mental condition or health problem reduce the amount or the kind of activity this person can do: (a) at home? (b) at work or at school? (c) in other activities, for example, transportation or leisure? Affirmative responses to one or more of these items were used by Statistics Canada to develop a sampling frame. The selection of the PALS sample from this frame used stratified random sampling to ensure feasibility of estimation by both province/territory and age group. Severity of disability was also included as a stratification factor during sampling.8
Because it is linked to a census, the PALS sampling frame covered people living in private and some collective households in the ten provinces and three territories of Canada. Populations living on First Nations reserves were excluded, as were residents of institutional collectives, military bases, Canadian Armed Forces vessels, merchant vessels, and coast guard vessels, as well as campgrounds and parks. Data were collected primarily by computer-assisted telephone interview. Deterministic imputation for missing data was carried out in specific circumstances by Statistics Canada, but only when sufficient information was available from related questions.6 Proxy responses were allowed. However, proxies were used only after “every effort” had been made to contact and interview respondents directly. If a respondent was not available when the interviewer called, multiple follow-up attempts were made. The proxy rate among those aged 15 and above in the PALS was 12.1%.9
The PALS interview included a questionnaire called the Comprehensive Health Status Measurement System (CHSMS), which was administered to all respondents. This questionnaire was originally designed to classify health status for the Health Utility Index (HUI).10 The HUI is a health utility measure, but utility weights were not used in this project. The CHSMS items were used to produce impairment ratings in six health status dimensions: vision, speech, mobility, dexterity, emotions, and cognition. Two additional dimensions, hearing and pain, are also covered by the CHSMS but could not be included in this study because of low frequencies of reported impairment. A listing of the CHSMS items can be found in the PALS questionnaire (available at http://www.statcan.gc.ca/imdb-bmdi/indexiP-eng.htm).
The PALS inquired about the use of mobility aids, the extent of instrumental support received, and help with preparing meals. The survey also sought to evaluate aspects of participation in leisure activity using items with the following wording: “Now I will ask you some questions about activities you do. In the past 12 months, did you do any of the following activities within your spare time?” This was followed by a series of specific response choices, such as “exercise, watch TV or videos, listen to radio or CDs.” Endorsement of responses indicating participation was followed by items asking about the frequency of participation in each activity.
The PALS incorporated complex design features including stratified sampling (unequal selection probabilities) but as a post-census survey is unique in not requiring clustering in the way that most large population surveys do. Statistics Canada develops sampling weights that account for these design features and support unbiased estimation of statistical parameters and their associated 95% confidence intervals. Adjustments to these weights for nonresponse were also made by Statistics Canada, reducing the risk of bias due to non-response. All of the analyses reported here incorporated these sampling weights, helping to ensure unbiased estimation of population parameters despite unequal selection probabilities and nonresponse. Statistical analyses were performed using the survey commands in Stata 11, version 11.0 (Stata Corp, College Station, TX) at the Prairie Regional Research Data Centre on the University of Calgary campus. Certain low-frequency estimates could not be reported in this article (eg, CHSMS ratings for hearing and pain, as mentioned above). The release of low-frequency estimates is prohibited because of data release rules intended to ensure the confidentiality of census respondents. The project was approved by the University of Calgary Conjoint Ethics Review Board.
Results
The number of sampled respondents aged 15 or older for the PALS was 38,839. The response rate was approximately 74%, with an actual sample of 28,640 respondents. Among these respondents, health-related impairments were confirmed for 22,513 (79%). According to Statistics Canada, the discrepancy between those apparently eligible because of health-related impairments and those confirmed to have health-related impairments arose primarily because some respondents had short-lived health issues that had resolved by the time they were contacted for participation in the PALS. A total of 245 people had MS, representing 1.1% of the PALS sample. Under the unrealistic assumption that no members of the population failing to screen into PALS would have MS, this would translate into a weighted population prevalence estimate of 0.2% (200 per 100,000). In the PALS sample, people with MS were predominantly female (71%) and married (59.8%), percentages comparable to those reported in prior studies.11–14 They were less likely than the general population to be employed at the time of the survey (26% working as compared with 62% of the general population). The proportion working is lower than the 40% to 70% reported in previous studies.11–14 This discrepancy may partially reflect a relatively older mean age in PALS respondents with MS (weighted mean of 50.5 years, compared with mean ages of 42 to 51 years in prior studies11–14 and 45.0 years in the general population). In turn, the older age of people with MS in PALS may arise partially from the need to have health impairments in order to screen into PALS, because early in the disease there is often no impairment. Thirty-eight percent of the PALS sample reported that they were permanently unable to work. The higher rate of employment in previous studies may also reflect a greater likelihood of working people being identified in the clinical sampling frames used in the previous studies, as they did not screen out those with no impairment.
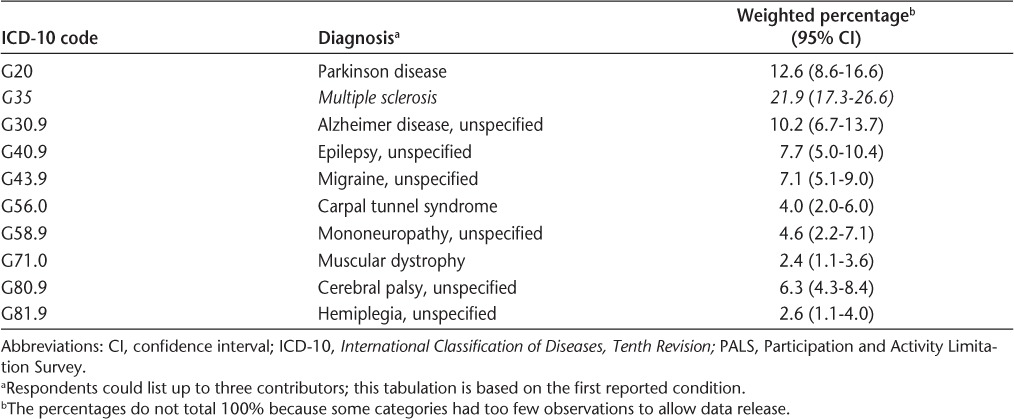
The percentages of PALS participants reporting various disabling conditions are reported in Table 1. The most common category of conditions was musculoskeletal. A total of 5.3% of the sample reported that their impairments were caused by a neurologic condition; the categories of such neurologic conditions are shown in Table 2. Among respondents with neurologic conditions, MS was among the most common conditions reported.
Table 1.
Categories of disabling conditions in the PALS sample
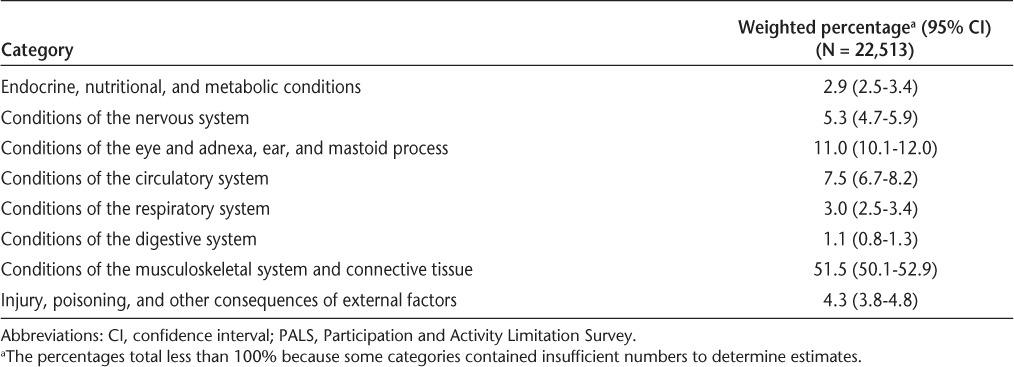
Table 2.
Categories of neurologic conditions in the PALS
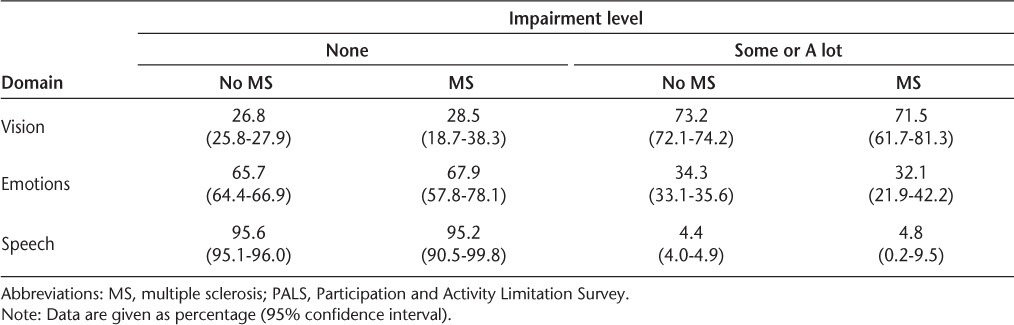
Health status information from the CHSMS is presented in Tables 3 and 4. The instrument identifies percentages of the sample reporting “none,” “some,” or “a lot” of impairment in various domains. The sample size supported estimation in six of the CHSMS domains: mobility, cognition, dexterity, vision, emotions, and speech. For mobility, cognition, and dexterity it was possible to estimate the frequencies in people with and without MS, whereas for vision, emotions, and speech the “some” and “a lot” categories had to be collapsed. Those with MS more often reported impairments, particularly severe impairments, in mobility, cognition, and dexterity.
Table 3.
Health-related impairments in the PALS sample by MS status: mobility, cognition, and dexterity
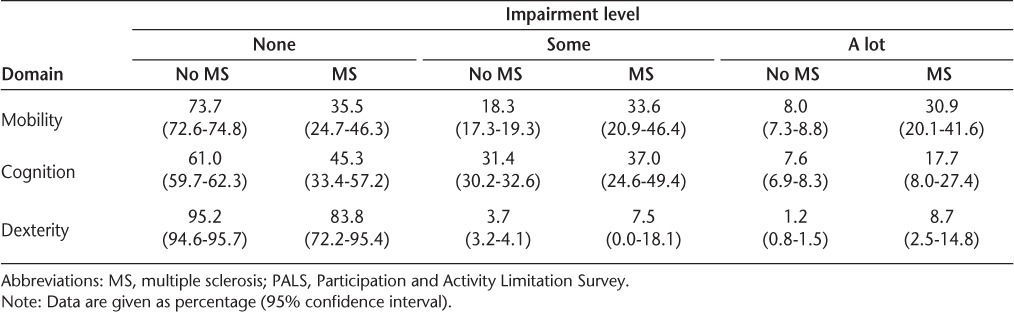
Table 4.
Health-related impairments in the PALS sample by MS status: vision, emotions, speech
As expected, the use of mobility aids was more common in people with MS (Table 5). The differences were most evident in the use of canes, grab bars, wheelchairs, walkers, scooters, and motor-vehicle modifications.
Table 5.
Use of mobility aids in the PALS sample by MS status
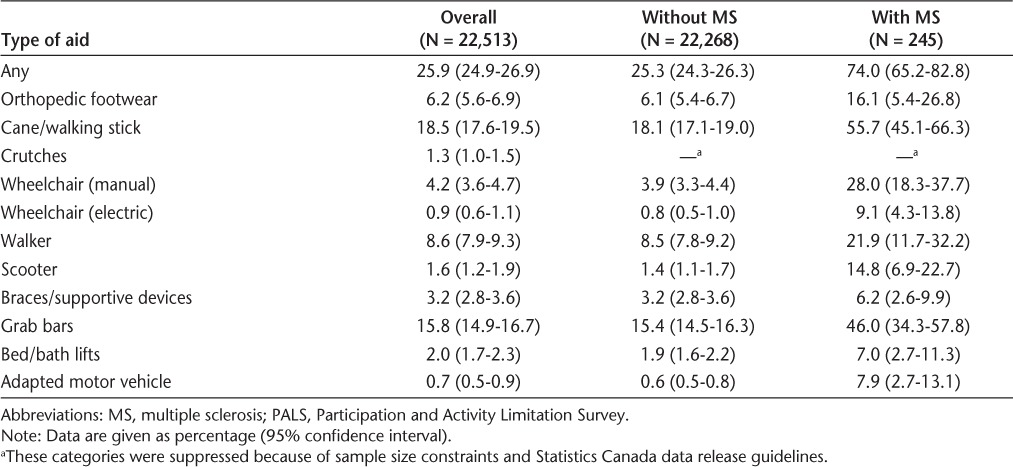
Table 6 presents the types and number of caregivers identified by PALS respondents with and without MS. The people with MS were more likely to have one or more caregivers and to identify multiple caregivers. Similar proportions of people with and without MS identified family or friend caregivers, but those with MS were far more likely to report having a paid caregiver.
Table 6.
Types and number of identified caregivers by MS status
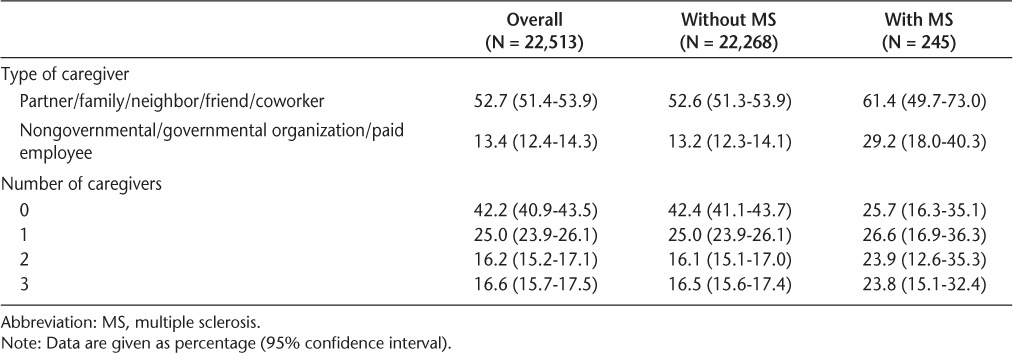
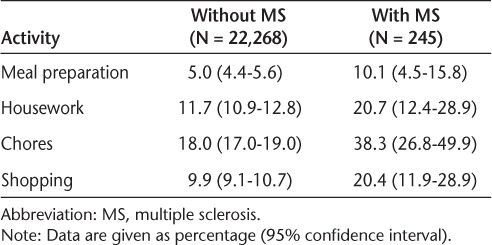
Table 7 presents the percentages of respondents with and without MS reporting that they either received no help or received inadequate help with four activities of daily living: meal preparation, housework, chores, and shopping. Unfortunately, the sample size did not permit a distinction to be made between those receiving no help and those receiving inadequate help. The differences between people with and without MS are substantial, with people with MS being twice as likely to fall into the “no help/inadequate help” category.
Table 7.
Proportions of respondents reporting no support or inadequate support for activities of daily living
In other domains of functioning, the proportion of people with MS reporting that they either did not need help or received all the help they needed was very high, with no differences discerned from those without MS: caring for self (95.8%), specialized home care (96.3%), and moving around the residence (97.3%).
Leisure activity is an aspect of participation in society. Of those activities evaluated in the PALS, the participation percentages were generally similar between those with MS and the rest of the PALS sample. Exercising at home at least once per week was reported by a higher proportion of those with MS (57.1%; 95% confidence interval [CI], 41.9%–72.2%) than without MS (44.5%; 95% CI, 42.7%–46.2%), but imprecision associated with the MS estimate precludes statistical differentiation from the non-MS component of the sample. Watching television or listening to music was reported as a daily activity by 94.8% (95% CI, 91.3%–98.2%) of those with MS and 91.3% (95% CI, 90.6%–92.0%) of those without MS. Reading was less often a daily activity for people with MS, being reported by 62.9% (95% CI, 51.0%–74.7%), as compared with 76.1% of those without MS (95% CI, 74.9%–77.4%). Participation in activities outside of the home was also comparable between people with MS and those with other types of disability. Of those with MS, 53.7% (95% CI, 41.2%–66.2%) reported visiting with family or friends at least once per week, compared with 48.8% (95% CI, 47.4%–50.1%) of those with other types of disability. Participation in physical activities outside of the home at least once per week was reported by 39.7% (95% CI, 22.6%–56.9%) of those with MS, compared with 45.3% (95% CI, 43.8%–46.9%) of those without MS. In both groups, 40% to 50% reported attending sporting or cultural events or visiting museums, libraries, or parks. Only 4.5% (95% CI, 1.3%–7.7%) reported no participation in society in any of the above-listed domains of participation.
Discussion
A key finding of this study is that people with MS more frequently reported unmet needs in certain activities of daily living than did those with other types of disability. This replicates the finding of Pohar and colleagues3 of higher levels of unmet need for services in people with MS. The result is also consistent with a report by Ytterberg et al.,12 although that study did not include a comparison group. Unlike the study of Pohar et al., the current analysis compared people with MS with those with other disabling health conditions rather than with the general population. The Stockholm MS Study found a high frequency (approximately 70%) of reliance on others for activities of daily living, consistent with the results reported here.4 A detailed analysis of activities of daily living from the Stockholm study identified some of the same problems with activities of daily living found in the present study, including in the areas of heavy housework, shopping, and cooking. Transportation outside the home also figured prominently among problematic areas in that study.5 In an Italian mail survey, home assistance and home modifications were strongly associated with disease severity.13 Khan et al.11 reported irregular access to support and rehabilitative services, another finding broadly consistent with the results reported here. In the current analysis, differences in unmet need between those with and without MS were not evident in self-care, specialized home care, or moving around the house but were dramatic in meal preparation, shopping, chores, and housework. These domains may not receive adequate attention in traditional home-care and community supportive services. These results cannot inform an overall assessment of the quality of home-care services available in Canada, as the comparisons are across MS and non-MS categories. Relatively speaking, however, the results indicate greater unmet need among people with MS than among people with other types of disability.
The PALS is a valuable source of data but has many limitations. One is that it does not use an entirely representative sample. Rather, respondents are screened in because they have impairments of various types. Respondents with MS can be identified because MS is likely to be reported as a cause of impairment by PALS respondents. However, the remainder of the PALS sample is heterogeneous. The most common sources of disability reported in PALS were musculoskeletal conditions. Another weakness of the PALS is a general lack of validated measures, although Statistics Canada did conduct extensive field testing of the items, including obtaining feedback from focus groups, in order to help ensure validity of the responses. The PALS is a general population survey that is not specifically designed for people with MS. The survey did not include standard MS measures such as the Expanded Disability Status Scale (EDSS)15 or any of the fatigue scales commonly used in MS research.16,17 Nor did it include validated assessment instruments for activities of daily living. Data available from the CHSMS, however, confirm that people with MS often struggle with more-severe health difficulties than do people with other conditions. Another weakness of the PALS is a lack of solid information about health-care utilization. Access to specific types of services has been assessed in previous studies but could not be assessed here because of limitations of the PALS data set.
The PALS provides a snapshot of certain important aspects of health status in the MS population in a way that is not distorted by help-seeking or voluntary subject recruitment. The picture is one of people struggling with a particularly intrusive illness, requiring considerable support, but continuing to have more unmet needs than people with other forms of disability. Despite this challenge, people with MS reported high levels of participation in society. A key finding for policy makers is that the areas of greatest unmet need are those that may be viewed as falling outside of the scope of traditionally defined health-care services and may therefore not receive adequate attention in the current system.
PracticePoints.
Although people with MS access more community supportive services than people with other disabling conditions, they also report higher levels of unmet need. This indicates that health-care systems are only partially effective in meeting the needs of people with MS.
The domains with the greatest unmet needs are meal preparation, housework, shopping, and chores. Innovative strategies are needed to deliver required supportive services in these areas.
Despite their relatively high level of impairment, people with MS maintain a strong level of participation in society. This can be interpreted as an indication of resiliency in the face of neurologic impairment.
Footnotes
Financial Disclosures: The authors have no conflicts of interest to disclose.
Funding/Support: This study was funded by an operating grant from the Alberta Addiction and Mental Health Partnership Program's Collaborative Research Grant Initiative (CRGI). The CRGI is funded by Alberta Health Services and Alberta Seniors and Community Supports. The funding source placed no restrictions on the presentation or publication of study results. The analysis presented here was based on data collected by Statistics Canada, but the results and conclusions do not represent the opinions of Statistics Canada. Dr. Patten is a Senior Health Scholar with Alberta Innovates, Health Solutions. Ms. Berzins is supported by an EndMS Studentship.
References
- 1.Murray TJ. Diagnosis and treatment of multiple sclerosis. BMJ. 2006;332:525–527. doi: 10.1136/bmj.332.7540.525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nicholas R, Chataway J. Multiple sclerosis. Clin Evid (Online). 2007;2007 [PubMed] [Google Scholar]
- 3.Pohar SL, Jones CA, Warren S, Turpin KV, Warren K. Health status and health care utilization of multiple sclerosis in Canada. Can J Neurol Sci. 2007;34:167–174. doi: 10.1017/s0317167100005990. [DOI] [PubMed] [Google Scholar]
- 4.Gottberg K, Einarsson U, Ytterberg C, Fredrikson S, von Koch L, Holmqvist LW. Use of health care services and satisfaction with care in people with multiple sclerosis in Stockholm County: a population-based study. Mult Scler. 2008;14:962–971. doi: 10.1177/1352458508089688. [DOI] [PubMed] [Google Scholar]
- 5.Einarsson U, Gottberg K, Fredrikson S, von Koch L, Holmqvist LW. Activities of daily living and social activities in people with multiple sclerosis in Stockholm County. Clin Rehabil. 2006;20:543–551. doi: 10.1191/0269215506cr953oa. [DOI] [PubMed] [Google Scholar]
- 6.Statistics Canada. Participation and Activity Limitation Survey (PALS) http://www.statcan.gc.ca/cgi-bin/imdb/p2SV.pl?Function=getSurvey&SDDS=3251&lang=en&db=imdb&adm=8&dis=2#a2. Updated November 30, 2007. Accessed January 20, 2012.
- 7.Statistics Canada. Overview of the Census. http://www12.statcan.gc.ca/census-recensement/2006/ref/dict/overview-apercu/pop1-eng.cfm. Updated November 30, 2011. Accessed January 20, 2012.
- 8.Statistics Canada. 2006 Census Long Form. http://www.statcan.gc.ca/imdb-bmdi/instrument/3901_Q2_V3-eng.pdf. Accessed January 20, 2012.
- 9.Statistics Canada. The 2006 Participation and Activity Limitation Survey: Disability in Canada. Data collection. http://www.statcan.gc.ca/pub/89-628-x/2007001/4124990-eng.htm. Updated December 3, 2007. Accessed January 20, 2012.
- 10.Furlong WJ, Feeny DH, Torrance GW. Multiplicative multi-attribute utility function for the Health Utilities Index Mark 3 (HUI3) system: a technical report. et al. McMaster University Centre for Health Economics and Policy Analysis Working Paper #98-11. 1998.
- 11.Khan F, McPhail T, Brand C, Turner-Stokes L, Kilpatrick T. Multiple sclerosis: disability profile and quality of life in an Australian community cohort. Int J Rehabil Res. 2006;29:87–96. doi: 10.1097/01.mrr.0000194393.56772.62. [DOI] [PubMed] [Google Scholar]
- 12.Ytterberg C, Johansson S, Gottberg K, Holmqvist LW, von Koch L. Perceived needs and satisfaction with care in people with multiple sclerosis: a two-year prospective study. BMC Neurol. 2008;8:36. doi: 10.1186/1471-2377-8-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Solari A, Radice D. Health status of people with multiple sclerosis: a community mail survey. Neurol Sci. 2001;22:307–315. doi: 10.1007/s10072-001-8173-8. [DOI] [PubMed] [Google Scholar]
- 14.Gottberg K, Einarsson U, Ytterberg C, et al. Health-related quality of life in a population-based sample of people with multiple sclerosis in Stockholm County. Mult Scler. 2006;12:605–612. doi: 10.1177/1352458505070660. [DOI] [PubMed] [Google Scholar]
- 15.Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability scale (EDSS) Neurology. 1983;33:1444–1452. doi: 10.1212/wnl.33.11.1444. [DOI] [PubMed] [Google Scholar]
- 16.Fisk JD, Pontefract A, Ritvo PG, Archibald CJ, Murray TJ. The impact of fatigue on patients with multiple sclerosis. Can J Neurol Sci. 1995;21:9–14. [PubMed] [Google Scholar]
- 17.Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The Fatigue Severity Scale: application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46:1121–1123. doi: 10.1001/archneur.1989.00520460115022. [DOI] [PubMed] [Google Scholar]