

Abstract
The high burden of syphilis in China presents a unique opportunity to examine temporal trends. This study used wavelet transformation and Fourier analysis to assess the presence of temporal oscillations in the incidence of syphilis among adults, gonorrhea, and congenital syphilis over 11 years in China's largest province. This study found a significant annual oscillation trend in the incidence of adult syphilis, consistent with a peak during July–September, which was 4-fold higher than the trough, which occurred during January–March. A similar but dampened trend was observed in the incidence of gonorrhea, and no trend was observed for the incidence of congenital syphilis. Further research on the temporal oscillation of the incidence of syphilis is needed.
Keywords: syphilis, gonorrhea, oscillation, wavelet, Fourier transform, immunity, disease dynamics
Since the 1990s, syphilis has reemerged as the most commonly reported communicable disease in many of China's largest cities, with an annual incidence of 32 cases per 100 000 population in 2011 [1, 2]. However, the declining gonorrhea case burden [3] alongside population-based reports of stable rates of condom use suggest that the increasing syphilis burden may not be related to behavioral changes. Instead, these conflicting trends may be related to immunological or ecological factors driving syphilis spread. A modeling study based on US data previously suggested that syphilis cases oscillated temporally, with a period of 8–11 years, because of natural immunity [4]. In the Chinese context, the low syphilis prevalence in the 1950s and 1960s may have attenuated partial immunity, causing increased susceptibility in the Chinese population today. In addition, ecological factors related to periodic holiday celebrations may shift clustered syphilis cases into hyperendemic periods [5]. Hormonal changes due to varying photoperiods and temperatures during different seasons may also lead to increased unsafe sex during specific months [6–8]. Better understanding of the temporal patterns of the syphilis burden may shed light on these factors and inform targeted syphilis control programs in China and worldwide.
The biological differences and similarities between syphilis in adults, congenital syphilis, and gonorrhea allow us to make inferences about temporal oscillation and drivers associated with observed trends. First, congenital syphilis is also reported in Chinese hospitals, but it should not oscillate because pregnant women can acquire syphilis at any point during gestation. Therefore, oscillation in congenital syphilis cases would suggest that the provision and reporting of health services underpin any observed temporal oscillation. Next, comparison with other sexually transmitted infections (STIs), such as gonorrhea, would control for seasonal variations in human sexual behavior. Last, syphilis has a high rate of symptomatic infection (50%–60%); thus, new primary and secondary syphilis cases can accurately represent incident syphilis. We use the same techniques to examine monthly reported primary and secondary syphilis cases, congenital syphilis cases, and gonorrhea cases in Guangdong Province, China, to assess for significant periodicity and infer temporal drivers responsible for those trends.
METHODS
Data
Primary and secondary syphilis, gonorrhea, and congenital syphilis case data were obtained from the Guangdong Provincial STI Control Center. For each month from 1996 through 2007, we collected data on the total incidence of syphilis (primary, secondary, and congenital) and gonorrhea, expressed as cases per 100 000 population for adult infections and cases per 100 000 live births for congenital syphilis. The availability of detailed disease incidence statistics across data sets allowed us to conduct analyses to determine the presence of temporal oscillations at the monthly level. Data after 1996 were analyzed because they were complete, had a consistent gonorrhea clinical definition, and separated primary/secondary syphilis cases from latent syphilis cases. This study did not use identifiable data and was exempted by the Guangdong Provincial STD Control Center Institutional Review Board.
Analytic Overview
Primary and secondary syphilis, gonorrhea, and congenital syphilis cases were examined as follows. First, a discrete wavelet transformation was performed to visually assess the presence of oscillatory patterns. Discrete wavelet transformations examine the frequency of incident cases to determine the presence of oscillation and whether the period of the detected oscillation varies over time. It allows us to ascertain whether the period is constant or varying. Second, data were detrended and processed. This was to eliminate the year-to-year change in disease incidence. Last, Fourier analysis was used to determine the statistical significance and nature of the oscillation period.
Wavelet Analysis
Wavelet analysis is a standardized tool to decompose data and examine temporal trends. For each disease, we performed a discrete wavelet transform on the incidence rate per 100 000 persons for adult infections and the incidence rate per 100 000 live births for syphilis. This was done in MATLAB 7.13 (Natick, MA), using the dwt function. The MATLAB wavelet analysis function transforms the reported incidence rate from a time series format to a time-frequency format. Thus, we are able to visually detect the frequency of each disease across time.
Data Processing
A data transformation was required to eliminate year-to-year variations in mean disease incidence because STIs increased annually over the entire period. A polynomial was fitted to each disease data set as an estimate of the moving average. The degree of the polynomial used was determined by the highest degree that had a nonzero coefficient for the xn term. The polynomial function was subtracted from the raw data to detrend the data set, which was then normalized. Plots for each year were overlaid to observe potential monthly trends.
Fourier Analysis
For each disease data set, a fast Fourier transformation (FFT) was performed, and the statistical significance of the frequency spectrum was determined by bootstrapping (ie, by resampling the data set and performing an FFT 1000 times). To determine the effect of each month on the frequency spectrum of each data set, we removed the same month for every year and performed a FFT. This was done separately for each of the 12 months.
Male/Female Syphilis Subpopulations
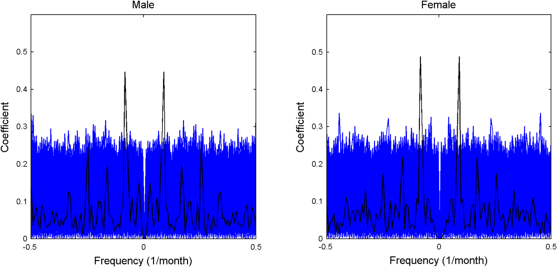
Because the syphilis incidence showed a statistically significant annual oscillation, we repeated the analysis for the male and female primary and secondary syphilis incidence data sets separately to ensure that the oscillation was still significant within subpopulations. This would confirm that the statistical significance is not merely an artifact when the syphilis incidence data set is analyzed as a whole.
RESULTS
A total of 92 685 primary and secondary syphilis cases, 252 492 gonorrhea cases, and 3001 congenital syphilis cases were reported from 1996 to 2007 in Guangdong Province, China.
Wavelet Analysis
Adult primary and secondary syphilis incidences revealed a regular and clear annual oscillatory period, while the gonorrhea incidence displayed a similar but more irregular periodicity (Supplementary Figure 1). The second lowest frequency subband showed a clear oscillatory pattern, with a period of 1 year, across both syphilis and gonorrhea data sets from 1996 through 2007. The oscillatory period was time invariant, making the data amenable to Fourier analysis. No oscillatory pattern was observed in the congenital syphilis data set (Supplementary Figure 1C).
Fourier Analysis (FFT)
Fourier analyses showed that only the adult primary/secondary syphilis oscillation was statistically significant (Figure 1). For adult primary/secondary syphilis, the historical reported incidence has a distinct peak, compared with the bootstrapped values, corresponding to a dominant period throughout the 11-year period. For gonorrhea, the incidence does not have a distinct peak, compared with the bootstrapped values, meaning that there was no significant periodicity. The case is the same for congenital syphilis.
Figure 1.

Fast Fourier transformation analyses of adult syphilis (A), gonorrhea (B), and congenital syphilis (C) from 1996 through 2007 in Guangdong Province. The black line represents the historical reported incidence, while the blue lines represent the randomized 1000 bootstrap values. Only the adult syphilis oscillation was statistically significant.
Mean Monthly Incidence
Figure 2 shows the mean monthly incidence, 95% confidence intervals, and highest/lowest incidence values over the entire data set. For primary/secondary syphilis, a peak was observed during July–September, which was 4-fold higher than the trough, which occurred during January–March. Based on the mean incubation period of Treponema pallidum infection of 2–3 months [9], these data suggest an annual increase in syphilis acquisition from March to May. For gonorrhea, there was no clear peak, but a decrease can be seen every January–February.
Figure 2.

Annual overlay of the incidence of adult syphilis (A) and gonorrhea (B) from 1996 through 2007 in Guangdong Province. The middle red line represents the mean disease incidence, the upper and lower ends of the box represents the 95% confidence interval, and the upper and lower lines represent the maximum and minimum disease incidence.
Male/Female Syphilis Subpopulations
Wavelet and Fourier analyses results for both male and female subgroups were similar to the above results (Supplementary Figures 2 and 3). This confirms the annual periodicity of syphilis.
Primary and Secondary Syphilis Cases
Incidences of both primary and secondary syphilis showed oscillations with an annual period. Oscillations in the incidence of primary syphilis case was more pronounced than oscillations in the incidence of secondary syphilis.
DISCUSSION
Our study found a statistically significant annual temporal oscillation in the incidences of reported primary and secondary syphilis in Guangdong Province, China, which is home to a population of >90 million. The lack of oscillation in the incidences of congenital syphilis makes health services explanations less likely to account for the observed trend. Previous syphilis research has suggested [4] and subsequently challenged [10] endogenous oscillation with a periodicity of 8–11 years, based on US Centers for Disease Control and Prevention (CDC) data. Although other research has examined temporal variations in the reported STI case burden [6, 8, 11–13], none have explored annual oscillations in the context of hyperendemic spread. With the exception of the study on CDC data, no studies have examined population-wide data. In addition, previous research in this field has not investigated trends at the fine temporal unit of a month; thus, subannual oscillations would not have been detected.
The incidence of gonorrhea did not show a statistically significant oscillation in the Fourier analysis. This might be attributed to a few reasons. First, the biology and immunology of gonorrhea and syphilis follow different patterns. This has been suggested in previous modeling studies [4]. Partial immunity to syphilis could account for this temporal oscillation. Second, syphilis has a higher transmission rate than gonorrhea [9, 14]. Thus, any underlying periodicity would be more pronounced. Third, in terms of transmission dynamics, syphilis is known to cluster, compared with gonorrhea. This phenomenon might contribute to the pronounced annual oscillations of the syphilis incidence. Taken together, the annual oscillations of the syphilis and gonorrhea incidences do not support the hypothesis by Grassy et al that syphilis incidence patterns can be explained by population-level immunity because syphilis and gonorrhea incidences oscillate in a similar pattern with a peak at the same time.
Our data show an annual increase in primary/secondary syphilis cases during July–August, which corresponds to an increase in syphilis transmission during April–May. There are possible mechanisms that could be investigated in further studies. One possible explanation for more-frequent sex during this period is the seasonal fluctuation in testosterone level, which is known to influence sexual activity. Another potential explanation is the occurrence of Labor Day in China, a 3-day annual holiday at the end of April and the start of May. Increased unsafe sex during this period could contribute to the observed data. This pattern is also consistent with findings from other studies, in which temporal oscillations in sexually transmitted diseases were observed [6, 12].
This research has several limitations. First, the surveillance infrastructure in Guangdong Province is more extensive in urban areas. Thus, reporting rates in urban areas are higher than those in rural areas and may not be entirely representative of the Guangdong population. The ecological drivers of disease transmission might also differ between rural and urban areas, which have not been investigated in this study. Second, we can only estimate the time of syphilis acquisition, given the lack of associated behavioral data. Third, pregnant women have a slightly higher risk of acquiring syphilis during the first and second trimester from a partner in the secondary stage of syphilis. Taking into account the periodicity of syphilis in the male population, there might be a certain degree of seasonal variation reflected in congenital syphilis rates, regardless of variation in sexual health services provision. Fourth, we do not have gonorrhea data disaggregated by sex. A seasonal gonorrhea fluctuation may be easier to detect among men who are more commonly symptomatic. Finally, we have no data on seasonal changes in health-seeking behaviors, which could also influence reported STI cases.
The observed annual temporal oscillation in the syphilis incidence has several important public health implications and has the potential to help sharpen syphilis responses in China and internationally. First, the predictable annual surges in syphilis cases suggest the need for greater vigilance at clinic-based services before the typical peak in reported cases. Syphilis control efforts and campaigns should be temporally focused immediately before the estimated peak in acquisition. Temporally focused clinic-based programs could include physician and nurse training about syphilis, enhanced partner services for partners of individuals with syphilis, and free screening programs. Many temporal safe sex campaigns have focused on World AIDS Day, held annually on 1 December, but our data suggest this may not be the time of greatest need for sexual health programs in China. Second, our data suggest the need for optimizing the temporal organization of sexual health services to better match needs and provision of services. Finally, more research is needed to understand the behavioral and biological underpinning of seasonal fluctuations in syphilis.
Supplementary Data
Supplementary materials are available at The Journal of Infectious Diseases online (http://jid.oxfordjournals.org/). Supplementary materials consist of data provided by the author that are published to benefit the reader. The posted materials are not copyedited. The contents of all supplementary data are the sole responsibility of the authors. Questions or messages regarding errors should be addressed to the author.
Notes
Financial support. This work was supported by the National Institutes of Health (Fogarty award 1K01TW008200-01A1), the Guangdong Provincial STI Control Center, and the Burroughs Wellcome Fund/American Society of Tropical Medicine and Hygiene Wellcome Junior Faculty Award in Tropical Infectious Diseases.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References
- 1.Tucker JD, Cohen MS. China's syphilis epidemic: epidemiology, proximate determinants of spread, and control responses. Curr Opin Infect Dis. 2011;24:50–5. doi: 10.1097/QCO.0b013e32834204bf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.China Centers for Disease Control and Prevention. 2011 report on syphilis and gonorrhea epidemic analysis in China.: Bull. STI Prev Control. 2012;26:9–19. [Google Scholar]
- 3.Chen XS, Peeling RW, Yin YP, Mabey DC. The epidemic of sexually transmitted infections in China: implications for control and future perspectives. BMC medicine. 2011;9:111. doi: 10.1186/1741-7015-9-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Grassly NC, Fraser C, Garnett GP. Host immunity and synchronized epidemics of syphilis across the United States. Nature. 2005;433:417–21. doi: 10.1038/nature03072. [DOI] [PubMed] [Google Scholar]
- 5.Gesink Law DC, Bernstein KT, Serre ML, et al. Modeling a syphilis outbreak through space and time using the Bayesian maximum entropy approach. Ann Epidemiol. 2006;16:797–804. doi: 10.1016/j.annepidem.2006.05.003. [DOI] [PubMed] [Google Scholar]
- 6.Fortenberry JD, Orr DP, Zimet GD, Blythe MJ. Weekly and seasonal variation in sexual behaviors among adolescent women with sexually transmitted diseases. J Adolesc Health. 1997;20:420–5. doi: 10.1016/S1054-139X(96)00275-3. [DOI] [PubMed] [Google Scholar]
- 7.Meriggiola MC, Noonan EA, Paulsen CA, Bremner WJ. Annual patterns of luteinizing hormone, follicle stimulating hormone, testosterone and inhibin in normal men. Hum Reprod. 1996;11:248–52. doi: 10.1093/humrep/11.2.248. [DOI] [PubMed] [Google Scholar]
- 8.Shah AP, Smolensky MH, Burau KD, Cech IM, Lai D. Recent change in the annual pattern of sexually transmitted diseases in the United States. Chronobiol Int. 2007;24:947–60. doi: 10.1080/07420520701648325. [DOI] [PubMed] [Google Scholar]
- 9.Garnett GP, Aral SO, Hoyle DV, Cates W, Anderson RM. The natural history of syphilis. Implications for the transmission dynamics and control of infection. Sex Transm Dis. 1997;24:185–200. doi: 10.1097/00007435-199704000-00002. [DOI] [PubMed] [Google Scholar]
- 10.Breban R, Supervie V, Okano JT, Vardavas R, Blower S. Is there any evidence that syphilis epidemics cycle? Lancet Infect Dis. 2008;8:577–81. doi: 10.1016/S1473-3099(08)70203-2. [DOI] [PubMed] [Google Scholar]
- 11.Schnell D, Zaidi A, Reynolds G. A time series analysis of gonorrhea surveillance data. Stat Med. 1989;8:343–52. doi: 10.1002/sim.4780080315. discussion 63. [DOI] [PubMed] [Google Scholar]
- 12.Wright RA, Judson FN. Relative and seasonal incidences of the sexually transmitted diseases. A two-year statistical review. Br J Vener Dis. 1978;54:433–40. doi: 10.1136/sti.54.6.433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fenton KA, Breban R, Vardavas R, et al. Infectious syphilis in high-income settings in the 21st century. Lancet Infect Dis. 2008;8:244–53. doi: 10.1016/S1473-3099(08)70065-3. [DOI] [PubMed] [Google Scholar]
- 14.Singh AE, Romanowski B. Syphilis: review with emphasis on clinical, epidemiologic, and some biologic features. Clin Microbiol Rev. 1999;12:187–209. doi: 10.1128/cmr.12.2.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
{kind=link}
{kind=link}
{kind=link}