

Abstract
Fractures of the acromion and scapula are known to occur after reverse shoulder arthroplasty. We present a case of a fracture at the base of the acromion 5 months after arthroplasty treated successfully with dual plating of the acromion. Eighteen months after fracture fixation, the patient had 160 degrees of active forward flexion, a QuickDASH of 29.5, a Constant score of 69 and she was satisfied with the result. A concomitant review of the literature produced, in addition to our patient, 56 cases. These were used to produce a classification system, based on bony and functional anatomy as follows. Tip fractures are of the most lateral or anterior portion of the acromion, those of the body of the acromion are medial to the tip but lateral to the beginning of the scapular base. Fractures at the scapular base are termed fractures of the base of the acromion and those more medial to that, fractures of the scapular spine. The functional results of these case series demonstrated poorer functional outcomes for more medial fractures. As future research in this domain increases, clarity on the nomenclature of these fractures will allow for prognostication and treatment based on fracture location as well as comparison between studies.
Keywords: Acromial fracture, post-operative complication, reverse shoulder arthroplasty, scapular fracture
INTRODUCTION
Reverse shoulder prosthesis is an excellent surgical option for patients with certain shoulder pathologies, of which rotator cuff arthropathy is one.[1,2,3] This is a procedure whose indications and surgical techniques are currently evolving. One area where we are gaining a greater understanding is that of managing acromial pathology. Recent studies are showing that not all acromial pathology is a contraindication to reverse shoulder arthroplasty; in both pre- and post-operative patients, small lateral fractures of the acromion can be treated non-operatively or fixed surgically with a tension band technique.[4,5,6] Overall, results comparable to that of reverse arthroplasty can be achieved with either of these treatment options.
However, fractures at the base of the acromion or of the scapular spine present a different problem.[7,8] In these types of fractures, a larger length of deltoid muscle is detached, and therefore defunctioned. In reverse shoulder arthroplasty, in order to achieve a stable shoulder, the deltoid must be tensioned a great deal. This in turn causes a deforming force and distraction at the fracture site, making for a poor healing potential. Also, as the reverse shoulder prosthesis relies on the deltoid muscle to move the arm, if the deltoid is detensioned or improperly tensioned, this will lead to poor functional capacity.[9]
We present a case of treatment of a fracture at the base of the acromion using a 90/90 plating construct that healed in a good position. We also present a review of the literature.
CASE REPORT
A 71-year-old right-handed woman presented with a 2-year history of right shoulder pain and dysfunction, which began abruptly when lifting a heavy load. At the initial evaluation, her range of motion was limited, particularly in active abduction as she achieved only 45 degrees in this plane. A cuff arthropathy (Hamada grade 3) was diagnosed and the decision was taken to proceed with reverse shoulder arthroplasty. To complete the pre-operative assessment, a CT scan was performed which confirmed there was no acromial pathology involved.
A reverse shoulder prosthesis and a biceps tenodesis was carried out (Delta Xtend™, Depuy, Warsaw, IN, USA) through a deltopecoral approach [Figure 1]. The patient's right arm was immobilized in a sling and the range of motion exercises were started 6 weeks after arthroplasty [Figure 1a]. Five months after surgery, she sustained a blow to the right shoulder but sought medical attention 1 month later, at her scheduled follow-up visit. Radiographs showed a displaced fracture at the base of the acromion [Figure 1]. A CT scan was performed to better characterize the fracture. This showed that both the humeral and glenoid components were well fixed and the only pathology was the fracture.
Figure 1.
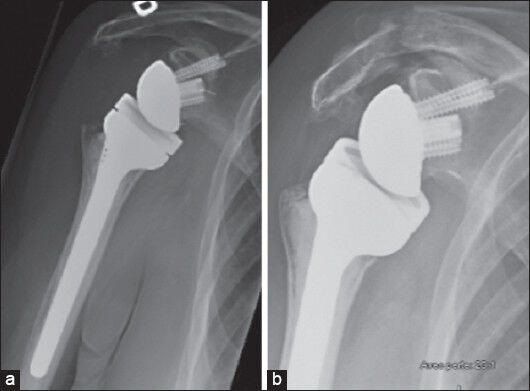
Antero-posterior radiographs showing the patient's right shoulder immediately after reverse shoulder arthroplasty (a) and after fracture, 5 months later (b). The post-operative image shows no pre-existing acromial pathology
She was taken to the operating room and her previous incision was extended into a “sabre” incision to better expose the acromion. Two small fragment (3.5 mm) locking plates (Synthes, West Chester, PA, USA) were used in a 90/90 configuration; one was a fragment specific clavicular plate and the other a reconstruction plate. The fragment specific clavicular plate was applied on the superior edge of the scapular spine in a compression mode. Distally, 2.7 mm locking screws were used. A second reconsrtuction plate was applied from the posterior acromion to the posterior cortex of the scapular spine, in the infraspinatus fossa. Long screws were placed from the posterior to the anterior acromion. Fixation was solid, but in order to protect the construct, the patient was placed in an abduction brace for 6 weeks.
Eighteen months after fracture fixation, the patient was satisfied with the clinical result [Figure 2]. She was capable of 125 degrees of abduction, 160 degrees of forward flexion, 85 degrees of external rotation in adduction, and 60 degrees of internal rotation. Her QuickDASH score was 29.5 (compared to 82.5 pre-op) and Constant score was 69 on the affected side compared to 85 on the left side, for a “good” functional outcome.
Figure 2.

Antero-posterior radiograph of the right shoulder demonstrating the dual plating technique. This radiograph was taken at final follow-up (18 months)
LETERATURE REVIEW
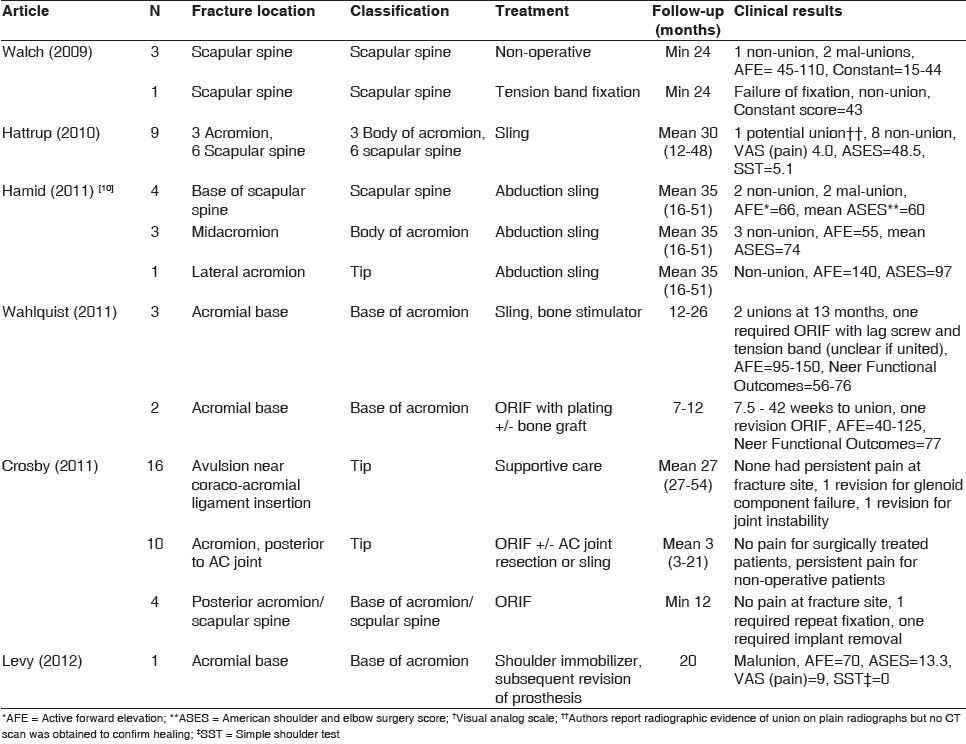
A MEDLINE search using the key words [acromion fracture], [scapula fracture], [reverse arthroplasty] was performed. Six relevant articles were identified, with a total of 57 cases. We then sought to classify and separate the cases by location; there were 30 cases of fractures at the base of the acromion, and scapular spine. When our case is added, we have a total of 31 cases. Results are summarized in Table 1. In brief, of the 30 more proximal cases, 21 were treated non-operatively in a sling, 7 were treated with open reduction and open fixation and one with revision of the prosthesis. Of those treated non-operatively, and for whom results are published, fourteen had a non-union, four had a malunion and in two cases, it was unclear whether union was achieved. For patients receiving fixation of the fracture, there was one non-union, two repeat fixations, and one patient required removal of the fixation. The patient who had a revision of the prosthesis had a malunion of the acromion.
Table 1.
Results of the literature review. In the fracture location column, the fracture description provided by the authors is presented. Our classification of the fracture follows in the classification column
DISCUSSION
Although recent studies have shown that good outcomes may be achieved with non-surgical management of lateral acromial fractures, the same does not hold true for basal acromial fractures.[5,6,7,8,9] The likely reason for this is that with fractures at the base of the acromion, a large length of the deltoid is defunctioned and the deltoid muscle is essential to the functioning of the reverse shoulder prosthesis.
Previously described techniques, such as tension band fixation achieved poor functional results for fractures at the base of the acromion.[4,7] We postulate that this is because the fixation method is insufficient to withstand the forces generated by the deltoid muscle — a tension band can neutralize forces parallel to the axis of the band but in the case of the deltoid, force vectors are generated in different directions. The dual locking plate technique described provides very rigid fixation. It also allows for compression along the fracture site and resists motion in all directions. Good screw purchase can be achieved by angling the screws either toward the scapular spine or the coracoid. The locking option enables good fixation and improves cut-out strength in osteopenic or osteoporotic bone. In addition to the stable fixation achieved with this technique, we further recommend immobilization of the affected shoulder using a sling and an abduction pillow to detension the deltoid, thus at least partially removing the distractive forces at the fracture site. Also essential to achieving a good functional result is regaining function of the shoulder. We thus also recommend a program of range of motion exercises followed by strengthening exercises to maximize functional capabilities.
Based on results from previous studies, bony and functional anatomy, and functional outcomes, fractures were classified by location. Fractures of the tip were those of the most lateral or anterior portion of the acromion. Fractures of the body of the acromion are those medial to the tip of the acromion and lateral to the beginning of the scapular base. The scapular base is the lateral border of the scapular spine, which is smooth and round. In our nomenclature, fractures at the scapular base are termed fractures at the base of the acromion as functionally, this zone connects the acromion to the rest of the scapula and this term avoids confusion with any more medially occurring fractures. Scapular spine fractures are those medial to the scapular base. This is represented in Figure 3.
Figure 3.
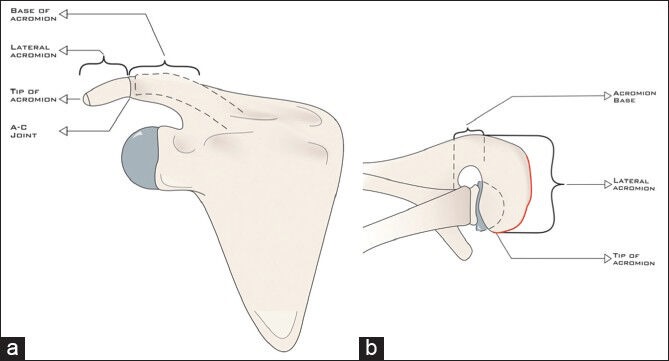
Coronal (a) and axial (b) representations of the proposed classification scheme for acromial fractures associated with revere arthroplasty
We propose the above mentioned classification system as it provides a nomenclature for acromial fractures that is descriptive and is based on the anatomy and functionality of the scapula. As the results from the review of the literature indicate, the more medial the fracture, the worse the prognosis with non-operative treatment. Thus, this classification system may be used to predict outcomes and determine treatment offered. It differs from other classification systems (Crosby) in that it further subclassifies more medial fractures, which are the more ominous fractures. As more research is carried out in this field, this will allow for more standardization amongst reports.
Footnotes
Source of Support: No external source of funding was used in the preparation of this study.
Conflict of Interest: The authors report no conflicts of interest
REFERENCES
- 1.Favard L, Katz D, Colmar M, Benkalfate T, Thomazeau H, Emily S. Total shoulder arthroplasty – Arthroplasty for glenohumeral arthopathies: Results and complications after minimum follow-up of 8 years according to the type of arthroplasty and etiology. Orthop Traumatol Surg Res. 2012;98:S41–7. doi: 10.1016/j.otsr.2012.04.003. [DOI] [PubMed] [Google Scholar]
- 2.Frankle M, Levy JC, Pupello D, Siegal S, Saleem A, Mighelli M, et al. The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. Surgical technique. J Bone Joint Surg Am. 2005;87:1697–705. doi: 10.2106/JBJS.D.02813. [DOI] [PubMed] [Google Scholar]
- 3.Rittmeister M, Kerschbaumer F. Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg. 2001;10:17–22. doi: 10.1067/mse.2001.110515. [DOI] [PubMed] [Google Scholar]
- 4.Walch G, Mottier F, Wall B, Boileau P, Mole D, Favard L. Acromial insufficiency in reverse arthoplasties. J Shoulder Elb Surg. 2009;18:495–502. doi: 10.1016/j.jse.2008.12.002. [DOI] [PubMed] [Google Scholar]
- 5.Crosby LA, Hamilton A, Twiss T. Scapula fractures after reverse total shoulder arthroplasty: Classification and treatment. Clin Orthop Relat Res. 2011;469:2544–9. doi: 10.1007/s11999-011-1881-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hattrup SJ. The influence os postoperative acromial and scapular spine fractures on the results of reverse shoulder arthroplasty. Orthopedics. 2010:33. doi: 10.3928/01477447-20100329-04. [DOI] [PubMed] [Google Scholar]
- 7.Wahlquist TC, Hunt AF, Braman JP. Acromial base fractures after reverse total shoulder arthroplasty: Report of five cases. J Shoulder Elbow Surg. 2011;20:1178–83. doi: 10.1016/j.jse.2011.01.029. [DOI] [PubMed] [Google Scholar]
- 8.Levy JC, Blum S. Postoperative acrmion base fracture resulting in subsequent instability of reverse shoulder replacement. J Shoulder Elbow Surg. 2012;21:e14–8. doi: 10.1016/j.jse.2011.09.018. [DOI] [PubMed] [Google Scholar]
- 9.Boileau P, Watkinson DJ, Hatzidakis AM, Balg F. Grammont reverse prosthesis: Design, rationale and biomechanics. J Shoulder Elbow Surg. 2005;14:147S–61S. doi: 10.1016/j.jse.2004.10.006. [DOI] [PubMed] [Google Scholar]
- 10.Hamid N, Connor PM, Fleischli JF. Acromial fracture after reverse shoulder arthroplasty. Am J Orthop. 2011;40:E125–9. [PubMed] [Google Scholar]