

Abstract
Simultaneous occurrence of papillary and follicular thyroid cancer, known as differentiated thyroid cancer, has been reported with various presentations, but presence of an anaplastic cancer, as an undifferentiated cancer, in addition to differentiated thyroid cancer is rarely reported. We here report a 40-year-old man with papillary thyroid cancer on his right thyroid lobe and metastasized to the right posterior triangle of the neck. Survey on the mass in the right posterior triangle revealed presence of simultaneous papillary, follicular, and anaplastic thyroid cancer. The patient underwent right thyroid lobectomy and he received adjuvant radiotherapy in combination with chemotherapy.
Keywords: Anaplastic, follicular, papillary, thyroid cancer
INTRODUCTION
Thyroid carcinoma comprises 1% of all malignancies but is the commonest malignant endocrine tumor.1 The simultaneous occurrence of different types of thyroid cancer in a single patient is a rare event.2 Although there are noticeable reports about synchronous papillary and follicular cancer or medullary and follicular cancer, the reports of simultaneous papillary, follicular, and anaplastic cancer are actually rare.3 The origin of these cancers is from follicular cells. Among different types of thyroid cancers, papillary thyroid carcinoma (PTC) tends to metastasized to cervical lymph nodes.4 We report concurrent three types of thyroid cancer in a 40-year-old man.
CASE PRESENTATION
A 40-year-old man presented to medical clinic with right neck mass appeared 2-3 months before. He had not any significant findings in his past medical history except functional colitis. He had not history of smoking, drinking, or drug abusing. He neither had exposure to radiation. He had been working in a shoes workshop without any known risk factors for thyroid cancer. Family history revealed the presence of brain tumor in his cousin. Physical examination showed the absence of lymphadenopathy, organomegaly, or skin changes. The only finding was a round firm painless mass with 2.5-cm diameter at posterior triangle in right side of the neck.
Blood tests showed normal CBC (with differentiation), FBS, renal, hepatic and thyroid functional tests, U/A, coagulation tests, and CEA, with minimally increased alpha-feto-protein. Thyroid ultrasonography with superficial 7.5-MHz probe was normal. Spiral CT-scan of lungs, abdomen, and pelvis was normal without metastatic lesion. Spiral CT-scan of neck showed a 42 × 37 × 31 mm solid tumor with peripheral calcification in right side posterior triangle behind the SCM muscle, with anteromedial replacement of carotid artery. FNA of the mass revealed PTC.
Right thyroid lobectomy was performed with right neck lymphadenectomy from level II-V. Early pathologic survey showed normal tissue with mild chronic inflammation for thyroid right lobe, and follicular variant of papillary carcinoma with diffuse areas for resected mass at posterior triangle in right side of the neck [Figures 1 and 2].
Figure 1.
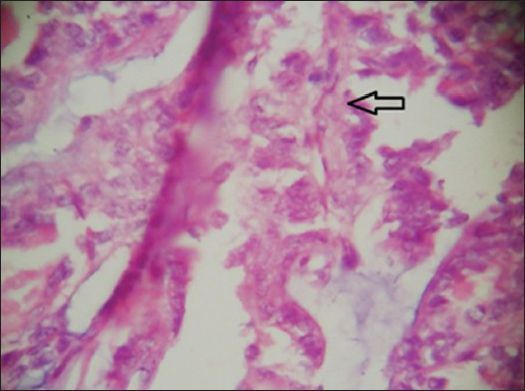
Papillary section of tumor with fibromascular core (arrow)
Figure 2.
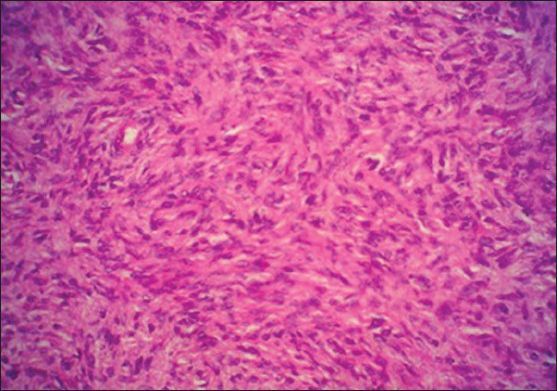
View of follicular cancer
Consultation to another expert pathologist revealed the presence of an occult focal area of papillary carcinoma in right thyroid lobe with metastasis to right posterior cervical lymph node, in which papillary and follicular variant transformed to anaplastic cancer [Figures 3 and 4].
Figure 3.
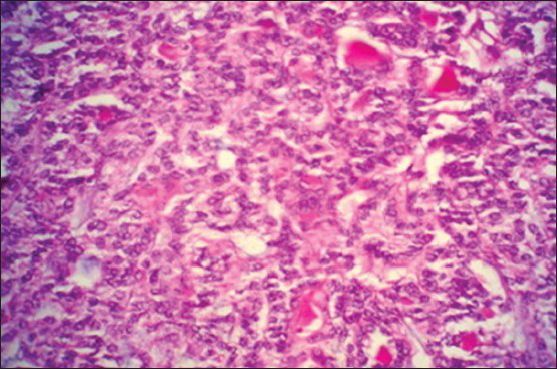
Anaplastic section of tumor with anaplastic spindle cells
Figure 4.
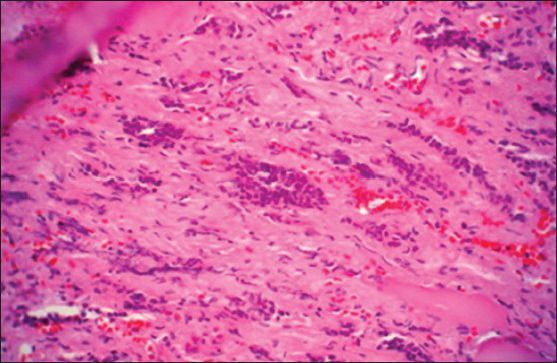
Anaplastic section of tumor with anaplastic round cells
The patient underwent adjuvant radiotherapy with Cobalt 60 THR machine. This therapy continued for five sessions in every week at level I-V and right supraclavicular and infraclavicular region with the dosage of 4500 CG in combination with 30-mg adriamycine. Then, by exclusion of spinal cord, the radiotherapy as boost dosage of 2600 CG was continued at level III-V and right supraclavicular and infraclavicular region without chemotherapy. He is alive and healthy after 4 years. His left thyroid lobe is intact and is being followed-up regularly. Until now, no recurrence is detected.
DISCUSSION
Thyroid carcinoma usually presents with a solitary or multi-nodular neck mass.5 Differentiated thyroid carcinoma (DTC) includes papillary and follicular subtypes6,7 and comprises 90% of all cases of thyroid cancer and its incidence varies from 0.5 to 10 new cases per 100000 population in whole world.8 It is usually curable when discovered at an early stage. However, because of the absence of prospective randomized trials of treatment, management of DTC is based on cohort studies which are not randomized.6 It is more common in females than males, but severity of disease in males is worse than in females. The prognosis is favorable in DTC with a 10-year survival rate of 80-95%.9 Mortality rate is low under the age of 40 and recurrence rate is low after the second decade of life until the age of 60.6,9
Anaplastic or undifferentiated carcinoma is a rare type of thyroid cancer, accounting for 1.6% of all thyroid cancers, and the most lethal one with the median life expectancy of 4 months.10,11 Anaplastic carcinoma has three subtypes including spindle cell, giant cell and squamoid or related combinations.12,13 In order to manage this cancer, surgery, and chemotherapy is suggested.14 Postoperative radiotherapy improved survival of patients with disease extending to adjacent tissue, but it does not provide much benefit for patients with further extended disease or distant metastasis.15
The patient, mentioned in this report, has had three types of thyroid cancer simultaneously, including differentiated and undifferentiated thyroid cancer in a mass in the right posterior triangle. First presentation of the disease was the right neck mass. Spiral CT-scan of neck showed a 42 × 37 × 31-mm solid tumor with peripheral calcification in right-side posterior triangle and FNA of the mass displayed papillary carcinoma. The mass was metastasized from the right lobe of thyroid which was developing DTC. Surgery was performed on him and right thyroid lobectomy and excision of the mass was done. After excision and double survey by two pathologists, it was revealed that right neck mass having DTC was transformed into anaplastic carcinoma. The patient received aggressive radiotherapy and chemotherapy after surgery. Adjuvant radiotherapy was done with Cobalt 60 THR machine for five sessions in every week at level I-V and right supraclavicular and infraclavicular region with the dosage of 4500 CG in combination with 30-mg adriamycine. Then, by exclusion of spinal cord, the radiotherapy as boost dosage of 2600 CG was continued at level III-V and right supraclavicular and infraclavicular region without chemotherapy.
In a study, Fletcher et al., after doing ploidy analyses, have shown aneuploidy in both differentiated and undifferentiated components.16 On the other hand, 71% of anaplastic carcinomas are said to either follow or occur simultaneously with differentiated carcinomas.13,17 Therefore, presence of concurrent follicular, papillary and spindle cell type of anaplastic cancer in patient's thyroid can describe two theories: The first and most probable one is dedifferentiation of a pre-existing follicular or papillary carcinoma into anaplastic carcinoma. The second one demonstrates that a common follicular cell was the origin of follicular, papillary and anaplastic carcinoma.13
We reported this case due to its rareness, in order to indicate that his prognosis was influenced by the therapy he received.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.2nd edition. London: Royal College of Physicians; 2011. British Thyroid Association. “Royal College of Physicians (2007) Guidelines for the management of thyroid cancer.” Report of the Thyroid Cancer Guidelines Update Group. [Google Scholar]
- 2.Cupisti K, Raffel A, Ramp U, Wolf A, Donner A, Krausch M, et al. Synchronous occurrence of a follicular, papillary and medullary thyroid carcinoma in a recurrent goiter. Endocr J. 2005;52:281. doi: 10.1507/endocrj.52.281. [DOI] [PubMed] [Google Scholar]
- 3.Lam K, Lo C, Chan K, Wan K. Insular and anaplastic carcinoma of the thyroid: A 45-year comparative study at a single institution and a review of the significance of p53 and p21. Ann Surg. 2000;231:329. doi: 10.1097/00000658-200003000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rosai J. Handling of thyroid follicular patterned lesions. Endocr Pathol. 2005;16:279–83. doi: 10.1385/ep:16:4:279. [DOI] [PubMed] [Google Scholar]
- 5.Tickoo SK, Pittas AG, Adler M, Fazzari M, Larson SM, Robbins RJ, et al. Bone metastases from thyroid carcinoma. Arch Pathol Lab Med. 2000;124:1440–7. doi: 10.5858/2000-124-1440-BMFTC. [DOI] [PubMed] [Google Scholar]
- 6.Reis L, Eisner M, Kosary C, Hankey B, Miller B, Clegg L, et al. Bethesda: National Cancer Institute; 2000. SEER Cancer Statistics Review, 1973-1997. [Google Scholar]
- 7.Steinhagen E, Guillem JG, Chang G, Salo-Mullen EE, Shia J, Fish S, et al. The prevalence of thyroid cancer and benign thyroid disease in patients with familial adenomatous polyposis may be higher than previously recognized. Clin Colorectal Cancer. 2012 doi: 10.1016/j.clcc.2012.01.006. [DOI] [PubMed] [Google Scholar]
- 8.Parkin DM, Muir C, Whelan S, Gao Y, Ferlay J, Powell J. VI. International Agency for Research on Cancer; 1992. Cancer incidence in five continents. [Google Scholar]
- 9.Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994;97:418–28. doi: 10.1016/0002-9343(94)90321-2. [DOI] [PubMed] [Google Scholar]
- 10.Gilliland FD, Hunt WC, Morris DM, Key CR. Prognostic factors for thyroid carcinoma. Cancer. 2000;79:564–73. doi: 10.1002/(sici)1097-0142(19970201)79:3<564::aid-cncr20>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 11.Kebebew E, Greenspan FS, Clark OH, Woeber KA, McMillan A. Anaplastic thyroid carcinoma. Cancer. 2005;103:1330–5. doi: 10.1002/cncr.20936. [DOI] [PubMed] [Google Scholar]
- 12.Carcangiu M, Steeper T, Zampi G, Rosai J. Anaplastic thyroid carcinoma. A study of 70 cases. Am J Clin Pathol. 1985;83:135. doi: 10.1093/ajcp/83.2.135. [DOI] [PubMed] [Google Scholar]
- 13.Ganguly R, Mitra S, Datta A. Synchronous occurrence of anaplastic, follicular and papillary carcinomas with follicular adenoma in thyroid gland. Indian J Pathol Microbiol. 2010;53:337. doi: 10.4103/0377-4929.64328. [DOI] [PubMed] [Google Scholar]
- 14.Pierie JP, Muzikansky A, Gaz RD, Faquin WC, Ott MJ. The effect of surgery and radiotherapy on outcome of anaplastic thyroid carcinoma. Ann Surg Oncol. 2002;9:57–64. doi: 10.1245/aso.2002.9.1.57. [DOI] [PubMed] [Google Scholar]
- 15.Chen J, Tward JD, Shrieve DC, Hitchcock YJ. Surgery and radiotherapy improves survival in patients with anaplastic thyroid carcinoma: Analysis of the surveillance, epidemiology, and end results 1983-2002. Am J Clin Oncol. 2008;31:460–4. doi: 10.1097/COC.0b013e31816a61f3. [DOI] [PubMed] [Google Scholar]
- 16.Galera-Davidson H, Bibbo M, Dytch H, González-Cámpora R, Fernandez A, Wied G. Nuclear DNA in anaplastic thyroid carcinoma with a differentiated component. Histopathology. 2007;11:715–22. doi: 10.1111/j.1365-2559.1987.tb02685.x. [DOI] [PubMed] [Google Scholar]
- 17.Spires JR, Schwartz MR, Miller RH. Anaplastic thyroid carcinoma. Association with differentiated thyroid cancer. Arch Otolaryngol Head Neck Surg. 1988;114:40. doi: 10.1001/archotol.1988.01860130044012. [DOI] [PubMed] [Google Scholar]