

Abstract
Background:
This study assesses self-reported tobacco use prevalence (cigarette, water-pipe, and medwakh) among applicants to Abu Dhabi's Premarital Screening program during 2011.
Methods:
Premarital Screening data reported to the Health Authority – Abu Dhabi from April to December 2011 were utilized to estimate tobacco use prevalence among applicants. Smoking prevalence was examined by nationality, age group and gender.
Results:
Overall, 24.7% of Premarital Screening Program applicants were current smokers; 11.5% smoked cigarettes, 5.9% smoked medwakh (hand-held pipe), 4.8% smoked water-pipe and 2.5% smoked a combination (more than one type). Men (19.2%) were more likely than women (3.5%) to be current cigarette smokers. Women were much less likely to smoke medwakh (0.1%) than men (11.5%), with male UAE Nationals having the highest medwakh smoking prevalence (16.1%). The overall prevalence of water-pipe smoking was 6.8% among men and 2.8% for women with the highest water-pipe smoking prevalence (10.2%) among Arab expatriate men.
Conclusions:
Variations in tobacco use prevalence among Premarital Screening Program applicants reflect preferences for different modes of tobacco consumption by nationality, age group and gender. Enforcement of tobacco control laws, including implementation of clean indoor air laws and tobacco tax increases, and targeted health education programs are required to reduce tobacco consumption and concomitant tobacco-related morbidity and mortality.
Keywords: Cigarette, medwakh, smoking, water-pipe
INTRODUCTION
Tobacco use remains the world's leading health hazard, killing more than six million people in 2010, taking one life every 6 s.[1] Dangerous in any form, tobacco is the number one preventable cause of death world-wide.[1] The United Arab Emirates faces an extremely high burden of tobacco-related diseases. Cardiovascular disease is the country's leading cause of death, accounting for 37.5% of all deaths in the Emirate of Abu Dhabi.[2] The Health Authority – Abu Dhabi has identified tobacco control as one of the top public health priority. Accurately measuring the prevalence of tobacco use is an important first step in designing policies and programs to prevent tobacco related disease. This study assesses self-reported tobacco use prevalence (cigarette, water-pipe and medwakh) among applicants to Abu Dhabi's Premarital Screening program during 2011.
Abu Dhabi's population of 2.3 million[2] (80% expatriates) makes it the largest of the seven emirates comprising the United Arab Emirates (population 8 million).[3] Tobacco was first introduced to Europe by New World explorers during the late 15th century. Sailors and Ottoman Empire traders introduced tobacco to the Eastern Mediterranean region during the early 16th century.[4] Several smoking apparatuses were developed or adopted within the region, including the water-pipe – a small hand-held smoking pipe most commonly used in the Arabian Gulf region.
Adult male cigarette use in Abu Dhabi has been estimated at 14.9% and adult female cigarette use at 0.1%.[3] Other sources indicate, overall smoking prevalence at 25% prevalence among expatriates in Abu Dhabi (29% of men and 6.6% of women).[2] As part of the comprehensive population-based weqaya screening program, 173,501 adult United Arab Emirate (UAE) Nationals in Abu Dhabi surveyed during the period April 2008-June 2010 measured overall male smoking prevalence at 24.2% and female smoking prevalence at 0.8%. Among men in this survey, the largest survey of its kind in the Arab world, 18.8% smoked cigarettes, 3.6% smoked medwakh, 1.7% smoked water-pipe, and 0.2% smoked cigars. Among male UAE National smokers in Abu Dhabi, 78% primarily smoke cigarettes, 13% smoke midwakh, and 5% use water-pipe.[5,6]
The water-pipe (also known as shisha, goza, hookah, nargileh, arghileh, kalyan, ghelyoon, and hubble-bubble) has a head into which 10-20 g of tobacco may be loaded. Combustion is usually accomplished by laying charcoal over the tobacco on a thin sheet of tin foil. Smoke containing combustion products of tobacco, charcoal and tin foil are inhaled through a tube after cooling by bubbling through a water reservoir in the base of the water-pipe.[7]
Two types of tobacco are commonly used – “ajami” and “ma’assel” (cured with molasses or honey). In one session (a water-pipe head), the amount of tar exposure is equivalent to smoking about 20 cigarettes and the amount of carbon monoxide, much of it from the charcoal, is equivalent to smoking about 100 cigarettes.[8] The misconception that water filtration renders water-pipe tobacco smoke harmless is as old as the water-pipe, dating back to at least the late 16th century.[9] The wide variety of fruit flavors and honey sweetener added to water-pipe tobacco tends to be more attractive to youth and sometimes is used to falsely present the water-pipe as a healthier, more “natural” alternative to cigarettes.[10]
The capacity of the medwakh bowl is about 0.5 g, smaller than most pipes in other parts of the world. However, the high nicotine content of the sifted tobacco (dokha) smoked in the medwak[11] h produces an effect that gives the tobacco its name (dokha in Arabic means “dizziness”). Dokha tobacco can be mixed with herbs, spices, dried flowers, fruit, and may contain other adulterants, such as powdered pharmaceutical products.[12] Unlike water-pipe tobacco, dokha tobacco is usually not cured with molasses or honey although, these varieties are available. Common types of dokha tobacco include barid (cold), daffi (warm), and har (hot). Although, research on the prevalence of water-pipe use in several countries exists, very little is known about the prevalence of medwakh use. Overall medwakh smoking prevalence has been estimated at 4.2% for the six northern emirates of Sharjah, Umm Al Quwain, Dubai, Ajman, Ras Al Khaimah and Fujairah.[12]
Water-pipe and medwakh users often harbor misconceptions that these alternate modes of tobacco consumption are less harmful than cigarettes. In some communities, water-pipe and medwakh are more socially acceptable forms of tobacco use. Water-pipe, in particular, is often portrayed as a component of traditional Arab social gatherings and interpersonal socialization. Arab youth may be introduced to a lifetime of tobacco addiction at family gatherings where it is not uncommon for underage youth to join adults in smoking from a shared water-pipe.[13] Medwakh is attractive to some users because the small bowl of tobacco can be smoked quickly during breaks or while driving, leaving less trace of smoke or odor on clothing than cigarettes.
METHODS
This article reports the prevalence of cigarette, water-pipe, and medwakh use among the adult (18 years and above) population of nationals and expatriates screened by Abu Dhabi's Premarital Screening program. All couples applying for a marriage license in Abu Dhabi are required by law[14] to complete a battery of tests for specific genetic conditions and infectious diseases, as well as questions about behavioral risk factors, including tobacco use.[15]
Data from the Health Authority-Abu Dhabi's (HAAD) Premarital Screening Program from April to December 2011 were used to estimate tobacco use prevalence among applicants during this period. Cigarette smokers were defined as applicants who reported having smoked at least one cigarette per day (regular smokers) or smoke on some days (occasional smokers). Medwakh smokers were defined as applicants who reported having smoked at least one medwakh per day or smoked on some days. Applicants who smoked at least one water-pipe head per week or smoked regularly were classified as water-pipe smokers. Nationality was classified as UAE Nationals (citizens) and Expatriates. Expatriates were further identified as either Arab expatriates if they held citizenship in one of the Arab League countries (not including the UAE) or other expatriates, representing all other countries. Countries of the Arab League (aside from UAE) are: Algeria, Bahrain, Comoros, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Palestinian Authority, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, and Yemen.[16] Descriptive statistics were calculated utilizing CDC EpiInfo 7™. Smoking status was examined by gender, nationality, age group, and mode of tobacco consumption (cigarette, medwakh, or water-pipe).
RESULTS
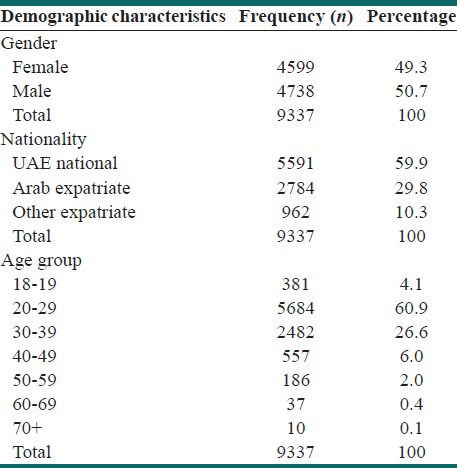
A total of 9337 adult applicants with a recorded smoking status were registered in the HAAD Premarital Screening Program database during the study period. Of which 2309 were self-reported adults smokers with further recorded information on current smoking behaviors. Table 1 illustrates demographic characteristics of the participants. The study pool was roughly equally divided between men (50.7%) and women (49.3%). (The slight discrepancy is probably due to some male applicants applying for marriage outside the country or other emirates hence not accompanied with the female partners). Sixty percent of applicants were UAE Nationals and more than half (60.9%) were in the 20-29 year age bracket. The mean age of applicants was 29 years with a standard deviation of 7.6 years.
Table 1.
Demographic characteristics, Abu Dhabi premarital screening program 2011 (n=9337)
Tobacco use prevalence
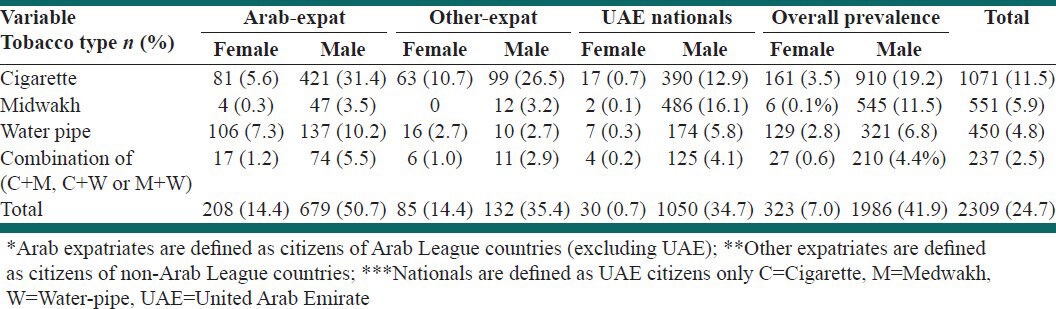
During the study period, 24.7% of premarital screening applicants were self-reported current smokers; 11.5% smoked cigarettes, 5.9% smoked using medwakh and 4.8% smoked using water-pipe [Table 2]. Arab expatriates had the highest prevalence of smoking at 31.9%, followed by other expatriates (22.6%) and Nationals (21.6%). Men (19.2%) were more likely than women (3.5%) to be cigarette smokers. Arab expatriate men reported the highest cigarette smoking prevalence (31.4%) and National women reported the lowest cigarette smoking prevalence (0.7%). Women were much less likely to smoke medwakh (0.1%) than men (11.5%), with male Nationals having the highest medwakh smoking prevalence (16.1%). The overall prevalence of water-pipe smoking was 6.8% among male and 2.8% among female applicants with the highest water-pipe smoking prevalence (10.2%) among Arab expatriate men.
Table 2.
Adult smoking prevalence by type, Abu Dhabi 2011 (premarital screening program applicants)
Cigarette use alone
The prevalence of current cigarette smoking varied substantially across population subgroups from 0.7% among National women to 31.4% among Arab expatriate men. Cigarette smoking prevalence was higher among Arab expatriate men (31.4%) than among other expatriate men (26.5%) and National men (12.9%). Among women, other expatriates had higher cigarette smoking prevalence (10.7%) than Arab expatriates (5.6%) and Nationals (0.7%).
Medwakh use alone
Variations on medwakh prevalence were observed by nationality. National men had the highest medwakh smoking prevalence (16.1%), followed by Arab expatriate men (3.5%), and Other expatriate men (3.2%). Women of all nationalities were much less likely (<1%) than men to smoke medwakh.
Water-pipe use alone
Smoking water-pipe is more common among Arab expatriates men (10.2%) than National men (5.8%) or other expatriates (2.7%). Arab expatriate women (7.3%) were more likely than other expatriates (2.7%) to use water-pipe. Only 0.3% of National women reported smoking water-pipe.
Combination use (2 or more types)
An overall 2.5% of smokers were combination users – smoking using more than one type of tobacco apparatus. Combination use was more common in men (4.4%) compared to women (0.6%). Highest prevalence was observed in Arab expatriate men (5.5%).
Age
National men aged 30-39 years were more likely to smoke cigarette (21.3%) or water-pipe (8.5%) compared to the 20-29 age group (9.2% and 5.1% respectively). In contrast, the prevalence of current medwakh smoking was higher (17.3%) among 20-29 year old National men than in the 30-39 age group (15.8%) [Table 3].
Table 3.
National men smoking prevalence for selected age group, Abu Dhabi, 2011 (pre-marital screening program applicants)

DISCUSSION
This report describes smoking prevalence among applicants to Abu Dhabi's Premarital Screening Program during April-December 2011. The results reflect patterns of tobacco use by gender, national origin and age group with Arab expatriate men reporting high cigarette smoking prevalence and National men reporting high medwakh use prevalence. Among women, Arab expatriates report the highest water-pipe smoking prevalence and other expatriates report the highest cigarette smoking prevalence. Medwakh smoking prevalence was highest among National men (16.1%), particularly the 20-29 year old age group (17.3% prevalence). Water-pipe smoking prevalence was highest among Arab expatriate men (10.2%); followed by Arab expatriate women (7.3%) and National men (5.8%). National women report very low smoking prevalence (<1%) for all tobacco types.
These results reflect the importation of female cigarette smoking habits by non-Arab expatriates residing in Abu Dhabi, the importation of water-pipe smoking patterns by Arab expatriates from neighboring Arab countries, and the high prevalence of medwakh smoking among male National youth. The extreme variations in the smoking patterns between male National compared to female National can be explained by the cultural acceptance for the males to smoke. Health promotion efforts should target young male UAE nationals to raise awareness about the harmful health effects of medwakh smoking and other forms of tobacco consumption. All expatriates should be educated about the tobacco hazard in all its forms. Smoking cessation services should be supported and other public health measures, enforcing clean indoor air regulations and increasing taxes on all types of tobacco products should be instituted to control the tobacco problem in Abu Dhabi.
Implications for public health practice
As the regulatory body for the healthcare sector in the Emirate of Abu Dhabi, HAAD has launched the “Abu Dhabi Says No to Tobacco” program to reduce smoking initiation, increase smoking cessation, and ensure clean indoor air environments for all residents of Abu Dhabi. A Tobacco Control Taskforce was established in 2010, chaired by HAAD and including key stakeholders, including government agencies and community organizations. Technical assistance is provided to partners in implementing the Federal Law 15 of 2009 on Tobacco Control. In addition to health education activities to raise awareness of the dangers of tobacco, the number of Continuing Medical Education sessions provided for health care professionals on smoking cessation has been increased and minimum requirements set for such trainings. The “Abu Dhabi Says No to Tobacco” program focuses on the three main modes of tobacco consumption in the UAE in all educational material. Three distinct symbols are used to raise awareness about the dangers of cigarette, water-pipe and medwakh smoking [Figure 1].
Figure 1.

Health authority-Abu Dhabi's “Abu Dhabi says no to tobacco” slogan image
Limitations
Limitations on this analysis include the self-reported source of the smoking prevalence data. Because, traditional cultural values in the region tend to stigmatize female smoking as unacceptable behavior, self-reported smoking prevalence, especially among UAE National women, may underestimate true smoking prevalence. Other groups, such as Arab expatriate women, may also be inclined to under-report their smoking status. The pool of applicants for the Abu Dhabi Premarital Screening Program may not be representative of the general population. Therefore, results cannot reliably be extrapolated to the general population. The premarital screening survey questionnaire asks applicants about their smoking status and primary mode of consumption but does not afford an opportunity for applicants to describe use of multiple product types, such as cigarettes and water-pipe or cigarettes and medwakh. Because applicants described only the primary type of tobacco used, the true prevalence of use for all types may be higher than the reported values.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Switzerland: World Health Organization; 2011. World Health Organization. Warning about the dangers of tobacco. WHO Report on the Global Tobacco Epidemics; pp. 8–12. [Google Scholar]
- 2.Abu Dhabi: Annual Health Statistics: Health Authority Abu Dhabi; 2010. [Accessed 2012 Aug 12]. Health Authority Abu Dhabi. Health population status in Abu Dhabi; pp. 14–6. Available from: http://www.haad.ae/Haad . [Google Scholar]
- 3.Abu Dhabi, UAE: National Bureau of Statistics; 2011. [Accessed on 2012 Sep 24]. National Bureau of Statistics. Population Estimates 2006-2010; pp. 14–5. Available from: http://www.uaestatistics.gov.ae/ReportPDF/Millennium%20Report_210113.pdf . [Google Scholar]
- 4.Ericksen M, Mackay J, Ross H. The Tobacco Atlas. Am J Epidemiol. (4th ed) 2012;15:14–8. [Google Scholar]
- 5.Al-Houqani M, Ali R, Hajat C. Tobacco smoking using Midwakh is an emerging health problem – Evidence from a large cross-sectional survey in the United Arab Emirates. PLoS One. 2012;7:e39189. doi: 10.1371/journal.pone.0039189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.AlHouqani M, Hajat C. Tobacco use amongst UAE Nationals. Am Coll Chest Physicians. 2011;140:438A. [Google Scholar]
- 7.American Lung Association, Tobacco Policy Trend Alert: From Joe Camel to Kauai Kolada—The Marketing of Candy-Flavored Cigarettes. [Last updated 2006 May]. Available from: http://www.lungusa2.org/embargo/slati/Trendalert_Waterpipes.pdf .
- 8.Shihadeh A, Saleh R. Polycyclic aromatic hydrocarbons, carbon monoxide, “tar”, and nicotine in the mainstream smoke aerosol of the narghile water pipe. Food Chem Toxicol. 2005;43:655–61. doi: 10.1016/j.fct.2004.12.013. [DOI] [PubMed] [Google Scholar]
- 9.Chattopadhyay A. Emperor Akbar as a healer and his eminent physicians. Bull Indian Inst Hist Med Hyderabad. 2000;30:21–255. [PubMed] [Google Scholar]
- 10.Switzerland: World Health Organization; 2005. WHO Study Group on Tobacco Product Regulation. Waterpipe tobacco smoking: Health effects, research needs and recommended actions by Regulators. s.l; pp. 45–7. [Google Scholar]
- 11. [Last accessed 2012 Oct 11]. Available from: http://www.midwakh.com/index.php?option=com_content&view=article&id=75&Item id=486 .
- 12.Jayakumary M, Jayadevan S, Ranade AV, Mathew E. Prevalence and pattern of dokha use among medical and allied health students in Ajman, United Arab Emirates. Asian Pac J Cancer Prev. 2010;11:1547–9. [PubMed] [Google Scholar]
- 13.Geneva: World Health Organization; 2008. [Last accessed 2012 Aug 14]. WHO report on the global tobacco epidemic, 2008. The MPOWER package. Available from: www.who.int/tobacco/mpower/en/index.html . [Google Scholar]
- 14.Ministry of Justice (UAE). Federal Law No. 28, Article 27. 2005. [Last accessed 2012 Sep 24]. Available from http://ejustice.gov.ae/portal/page/portal/eJustice%20MOJ%20Portal/About%20Us/Law%20of%20Personal%20Affairs .
- 15.Abu Dhabi: Health Authority Abu Dhabi; 2011. [Accessed 2012 Aug 12]. Health Authority-AbuDhabi. HAAD standard for premarital screening. s.l; pp. 14–6. Available from: http://www.haad.ae/Haad . [Google Scholar]
- 16.League of Arab States. Pact of the League of Arab States. 2010. [Last accessed 2012 Jun 3]. Available from: http://www.arableagueonline.org .