

Abstract
Objective:
This study was carried out to measure the caries prevalence and treatment needs in school children of 6-14 year old residing in coastal areas of West Bengal.
Materials and Methods:
A total of 1764 children of 6-14 years age group, studying in different primary and high schools of the coastal areas were examined using World Health Organization criteria (1997) to record the prevalence of dental caries. The treatment needs were also calculated according to that given criteria.
Statistical Analysis:
The results were subjected to statistical analysis using the Chi-square test and unpaired ‘t’ test.
Results:
Dental caries were founded low in the studied population. The overall all caries prevalence in the permanent dentition was 28.06%, in boys it was 25.39% and in girls it was 30.86%. Therefore caries prevalence in female was higher and which was statistically highly significant (P < 0.05). The most frequently required treatment was one surface filling followed by other treatments irrespective of sex and age group.
Discussion:
The presence of sea foods containing high fluoride and least availability of refined carbohydrate in the diet may be the reason of lower prevalence.
Conclusion:
child oral health is always a matter of concern for a developing country so further research is required to explore actual causes.
Keywords: Coastal areas, dental caries, prevalence, treatment needs
Introduction
Dental caries is the most prevalent chronic infectious disease in developed and as well as in developing countries and it prevails as a worldwide epidemic[1] . More than 40% of Indian children are found to be afflicted with dental caries[2] . A large number of those children are residing in the coastal areas of West Bengal.
Geographical location plays a great role in caries prevalence, It varies with the change in location. According to National Oral Health Survey report 2004[3] , caries prevalence in India was 51.9%, 53.8% and 63.1% at ages 5, 12 and 15 years respectively in different parts of India. Available literature from 1940-1960, the prevalence of dental caries in India showed a varied picture[4,5,6] . In spite of conflicting reports it has been observed that during 1940 the prevalence of dental caries in India[7] was 55.5%, during 1960 it was reported to be 68.4%.
Materials and Methods
The area of the study was coastal districts of West Bengal and it was conducted in between 2010 and 2011. The Bay of Bengal is situated in the southern border of West Bengal. Schools were randomly selected from the two coastal districts (East Midnapore and South 24 Parganas) and dental investigation was carried out for 6-14 years aged children. Cluster sampling technique was used for the study because it was more beneficial to examine a cluster of children rather than an individual
At first informed consent, after discussing the risk and benefit of the study, was taken from the school authority as well as from the guardian of the children. The dental examination of children studying in different Primary and high schools in different region of the coastal area was conducted. The examination was carried out in the respective school of the students, sitting in an ordinary chair with the help of a simple mouth mirror and dental explorer. CPITN (Community Periodontal Index for Treatment need) probe was used for diagnosis of dental caries to differentiate between cavitated lesion and surface demineralization. Dental caries were assessed as per the World Health Organization criteria 1997[8] and treatment needs was also calculated accordingly. A simple questioner season was carried out with the child keeping his parent in front, regarding their socioeconomic status and oral hygiene practice. Last 7 days dietary history was also taken.
There was a source of natural light in the room in which examination was conducted. The light was consistent as far as possible throughout the survey. A torch light was kept by the operator for extra illumination if required. The examination area was partitioned and arranged in such a way that the subject entered at one way and left another way along his or her guardians. They were not allowed to crowd around examination table. No radiograph was taken.
Results
The study was carried out among 1764 children of 6 to 14 years of age from different government primary and high schools in coastal areas of West Bengal mainly in East Midnapore and South 24 Parganas districts.
Total children those who were examined in the present study were divided into three age groups (6-8 years, 9-11 years and 12-14 years). The distributions of boys and girls of those age groups were shown in Table 1.
Table 1.
Age and sex wise sample distribution

The distribution table [Table 2] depicts a comparative evaluation of a number of children with caries and caries free permanent teeth in 6-8 years age group. When statistical analysis was performed to evaluate the frequency of carious children, it reveals statistically insignificant (χ2 = 0.956, df = 1, P = 0.328). On the other hand in spite of high decayed, missing and filled teeth DMFT in boys statistical analysis gave an insignificant interpretation (t = 0.74 P = 0.460 df = 61).
Table 2.
DMFT index and caries prevalence in permanent teeth of 6-8-year-old children

The deft index and caries prevalence in primary teeth of 6-8 year- old children is summarized in Table 3. Though the prevalence in boys were higher but the frequency was statistically insignificant (χ2 = 0.430, df = 1, P = 0.512), similarly the mean deft was higher in boys but statistically insignificant (t = 1.18 P = 0.239 df = 244).
Table 3.
Deft index and caries prevalence in primary teeth of 6-8-year-old children

The contingency table [Table 4] shows the mean DMFT index and caries prevalence in permanent teeth of 9-11 years old children. Chi-square statistical test was performed to analyze the frequency of caries in boys and girls and revealed a significantly higher (χ2 = 6.542, df = 1, P = 0.011) caries prevalence in the permanent dentition in boys. Similarly when statistical analysis was performed for the two mean (mean DMFT), it revealed significantly higher (t = 3.16 P = 0.002 df = 272) DMFT index in boys than girls.
Table 4.
DMFT index and caries prevalence only in permanent teeth of 9-11-year-old children

Table 5 express the caries prevalence in primary teeth of 9-11 year old children residing in coastal areas of West Bengal. Chi-square test was performed to evaluate the data and test revealed an insignificant variation in caries prevalence in boys and girls (χ2 = 1. 515, df = 1, P = 0. 218). The unpaired t test was also performed to explore the difference between two mean (mean deft) and it showed a significantly higher (t = 2.16 P = 0.031 df = 312) deft index in boys than girls.
Table 5.
Deft index and caries prevalence in primary teeth of 9-11-year-old children

Table 6 depict a comparative evaluation of caries prevalence of permanent teeth in boys and girls of 12-14 years age group children. Statistical analysis revealed that χ2 = 2. 913, df = 1, P = 0. 088, which signifies that in this age group there was no significant variation in caries prevalence. Although there was a difference present in mean DMFT index and statically significantly higher DMFT index proved in boys (t = 2.10 P = 0.036 df = 305).
Table 6.
DMFT index and caries prevalence in permanent dentition of 12-14-year-old total children

The contingency table [Table 7 and Figure 1] depicts the prevalence of dental caries in permanent teeth of the total sample examined for the present study. Chi-square test revealed a significantly higher (χ2 = 6.534, df = 1, P = 0.011) caries prevalence in girls than boys.
Table 7.
Caries prevalence in permanent teeth in total children
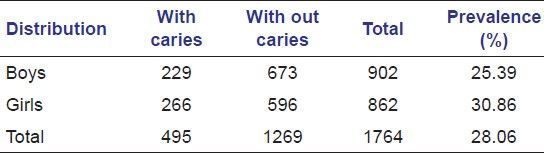
Figure 1.
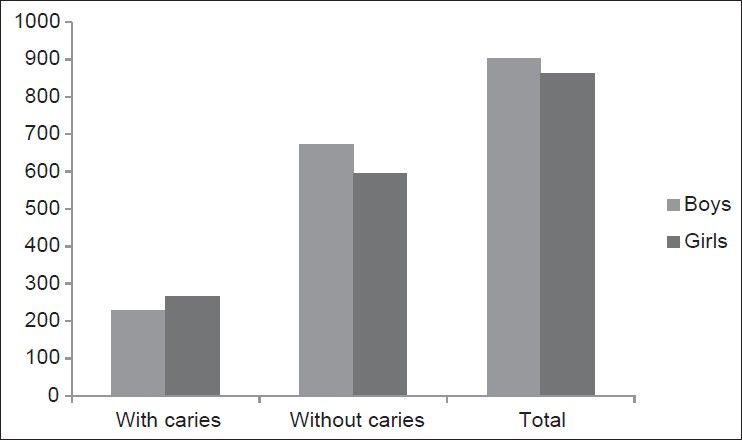
Caries prevalence in permanent teeth in total children
Table 8 and Figure 2 highlight the status only of primary teeth of the total sample. The prevalence dental caries in the primary dentition in boys and girls were 55.72% and 51.81% respectively. The chi-square test showed a statistically insignificant co-relation (χ2 = 1. 598, df = 1, P = 0. 206) in caries prevalence.
Table 8.
Caries prevalence in primary teeth of total children
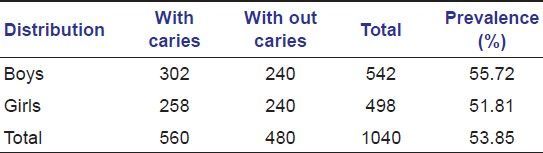
Figure 2.
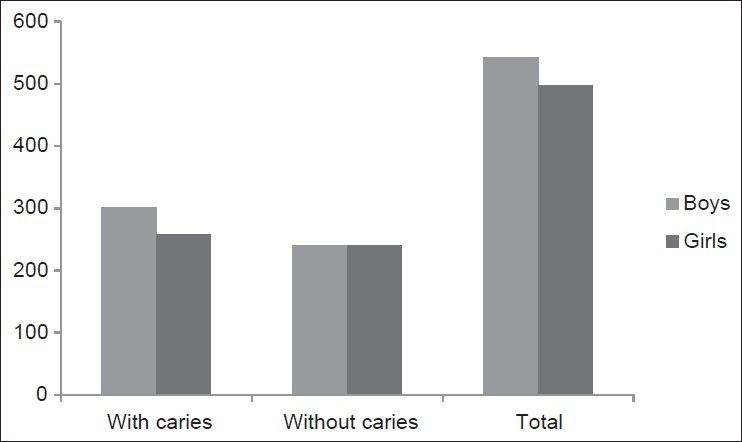
Caries prevalence in primary teeth of total children
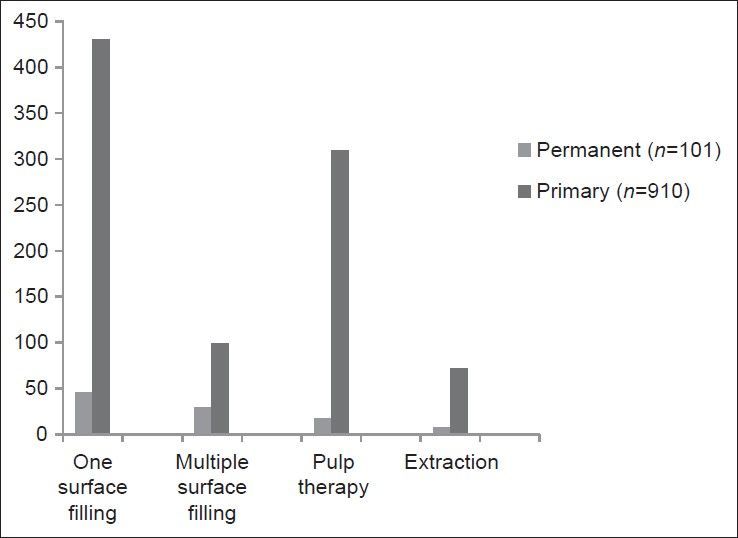
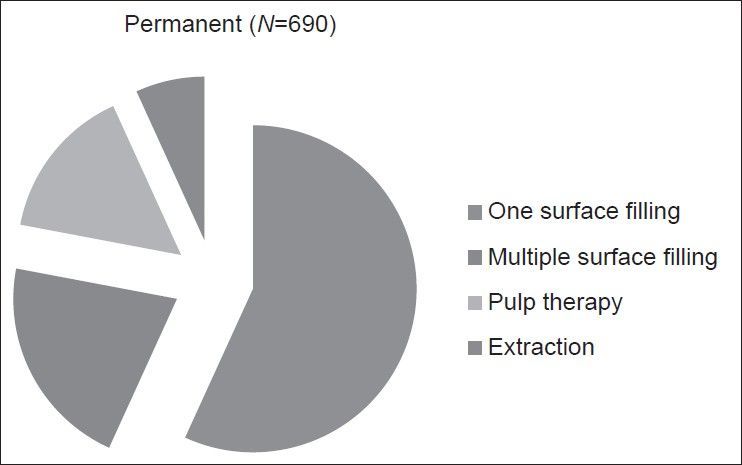
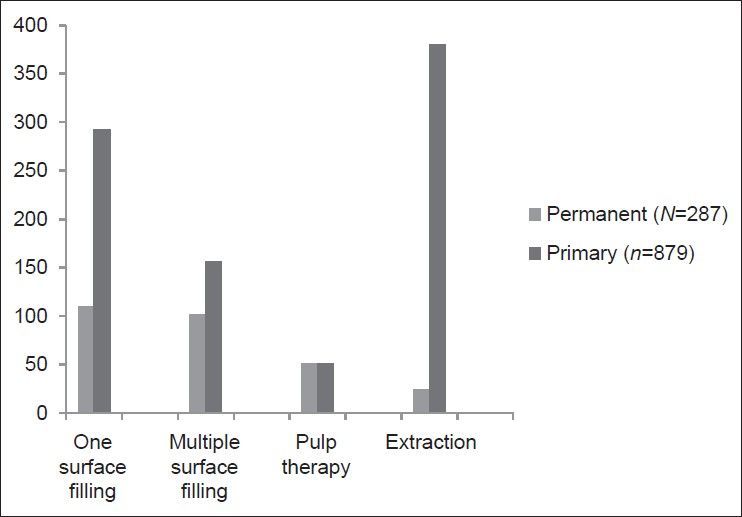
Tables 9–11 and Figures 3–5 depict the treatment need for the affected teeth of the children studied. Irrespective of age group and sex the most frequently required treatment were one surface filling followed by multiple surface filling pulp therapy and extraction except for the primary teeth of 9-11 years of age group where the most frequently required treatment was extraction.
Table 9.
Treatment need for 6-8-year-old children
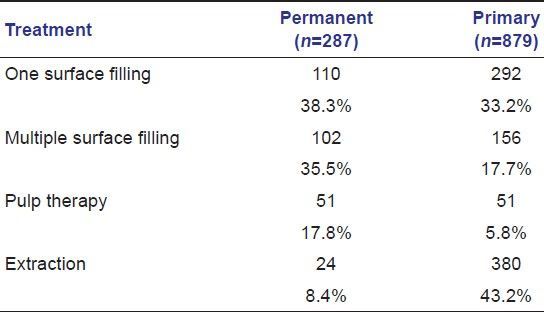
Table 11.
Treatment need for 12-14-year-old children
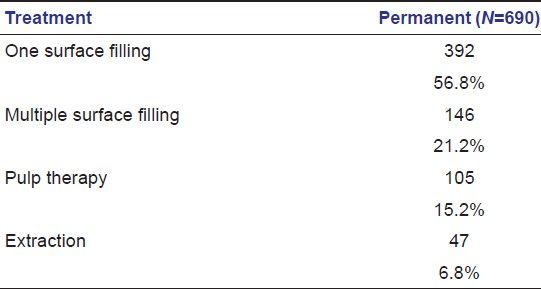
Figure 3.
Treatment need for 6-8-year-old children
Figure 5.
Treatment need for 12-14-year-old children
Table 10.
Treatment need for 9-11-year-old children
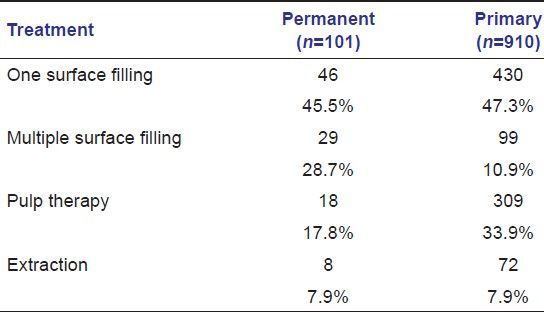
Figure 4.
Treatment need for 9-11-year-old children
Discussion
Dental caries is a multi-factorial, microbial, infectious, transmissible disease of hard tissues of teeth characterized by the demineralization of inorganic structures and subsequent breakdown of organic moieties along with remineralization of the demineralized structures until there is cavitation. A plenty of influencing factors have been postulated by various authors regarding its etiology. Socioeconomic status, availability of the sticky carbohydrate containing foods, dietary intake of fibrous foods, the presence of fluoride or other micronutrients in diet, sugar intake frequency and oral hygiene maintenance all have to some extent influence over the causation of dental caries.
The present study was carried out among 1764 school children from 6-14 years of age and the overall all caries prevalence in permanent teeth were 28.06%, in boys it was 25.39% and in girls it was 30.86%.
Hence, it was seen that the prevalence of dental caries was much lower in the studied population than many other studies conducted by different researchers in different parts of the globe. However the burden of treatment need was high. Not a single tooth was found treated by any dentist in the total studied children.
Few unique features of the samples might be the key factors of this kind of result. These were.
Almost all the children used to take sea fish 4-5 times a week in their diet which is a rich source of fluoride, the principal caries inhibiting substance
As the areas were very remote and the study children were from socioeconomically backward families so the availability and accessibility to refined a sticky carbohydrate food was very meagre
One good sign regarding the study group was that 65% to 78% children use toothbrush regularly.
A similar result was reported by Saravanan et al.[9] in 2005. They reported the prevalence of caries in the permanent dentition was 26.5%. The prevalence of caries increases significantly with age in the permanent dentition.
A very low level of dental caries was reported by Frencken et al.[10] in 12 year old school children of urban Kenya in 1984. Nearly 22% caries prevalence and 0.5 DMFT were reported by the author.
Low caries prevalence was reported by Knutson[11] in 1947. He reported the caries prevalence of 6 years old in Nicollet Country, Minnesota. The caries prevalence was 24.3%.
In 1939 Sarkar[12] examined 18,445 school children up to 16 years of age in West Bengal. He reported that 13.3% children had defective teeth. furthermore in 1931 he examined 2,000 children and found 14.4% had defective teeth.
Similar findings like the present study was also seen in studies of Bagramian et al.[2] on Amish children and Sgan-Cohen et al.[2] founded the prevalence of dental caries to be very low among 5 and 12-year old children.
On the other hand the findings of the present study were dissimilar with the study performed by Bhat Meghashyam et al.[2] among coastal fisherfolk communities of the Uttera Kannada district of Karnataka in 2007. They reported a very high prevalence of dental caries in permanent dentition of around 63.87% with a mean DMFT of 1.896 at the age of 10-14 years. The authors had concluded that the availability of sticky carbohydrate rich diet and certain trace elements such as selenium, relative humidity might have influenced the occurrence of dental caries in the study population.
Kulkarn and Deshpande[13] in 2002 carried out a study among 2005 school children in 11-15 years age at Belgaum city. The prevalence of dental caries in the population was 45.12%. The mean DMFT was 1.18. Males and low socioeconomic groups showed a higher prevalence.
Dash et al.[14] in 2002 also reported a high level of dental caries in children from Cuttack, Orissa. The point prevalence of dental caries was reported to be 64.3% with an average DMFT index of 2.38 at the age of 5-15 years. According to them the prevalence of caries showed a pattern of occurrence, i.e., prevalence consistently increased from 5 years to 8 years age group and subsequently decreased at 11 years and 15 years age.
Rao et al.[15] in 1999 also examined the dental caries status among school children of Moodbidri and the reported caries prevalence was as high as 76.9%. They also blamed the presence of refined carbohydrate in the diet and lack of oral hygiene maintenance for such high caries prevalence
Tayebe et al.[16] in 1985 reported the caries prevalence of 10-14 year old children of urban Sudan. They found 64% of children were affected by dental caries with a mean DMFT index of 1.7.
In 1941 Shourie[6] reported an overall 55.5% of caries prevalence in Indian children.
On the other hand in the present study the overall caries prevalence in primary teeth was 53.85% (in Boys- 55.72% and in girls 51.81%). Though the prevalence was slightly higher in boys but the difference was statistically insignificant (P > 0.05).
In 2005 Saravanan et al.[9] reported dental caries was more prevalent in the primary dentition in boys and the prevalence of caries was 71.1% and not associated with increasing age.
King[17] in 1938 reported In West Ross-Shire country school 53.3% of deciduous teeth were carious. In the Lewis country primary school 24.2% of deciduous teeth were carious.
Ainsworth and Young[18] . In 1925 examined a total of 4600 school children of 5-13 years age of the British Isles. They reported that 43.3% of all upper deciduous teeth were carious.
Conclusion
The present study was carried out to assess the caries prevalence and treatment need for the children of 6-14 years of age of coastal areas of West Bengal. Following conclusions can be drawn from the results:
The overall all caries prevalence in the permanent dentition was 28.06%, in boys it was 25.39% and in girls it was 30.86%. Therefore caries prevalence in female was higher and which was statistically highly significant (P < 0.05)
The overall caries prevalence in the primary dentition was 53.85% (in Boys- 55.72% and in girls 51.81%). Though the prevalence was slightly higher in boys but the difference was statistically insignificant (P > 0.05)
Caries prevalence in the study was lower than most of the national study done in India. Frequent dietary intake of sea fish containing high fluoride and less availability of refined carbohydrate may be the probable reasons of such low prevalence
Regarding treatment need the most frequently required treatment was one surface filling followed by other treatments irrespective of sex and age group.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Jams SW, Kevin JD. Cariology. Dent clin North Am. 1999;43:569–78. [PubMed] [Google Scholar]
- 2.Meghashyam B, Nagesh L, Ankola A. Dental caries status and treatment needs of children of fisher folk communities, residing in the coastal areas of Karnataka region, south India. West Indian Med J. 2007;56:96–8. doi: 10.1590/s0043-31442007000100018. [DOI] [PubMed] [Google Scholar]
- 3.National oral health care program implementation strategies . DGHS. MOH and FW; Govt of India. 2004 [Google Scholar]
- 4.Damle SG, Patel AR. Caries prevalence and treatment needs amongst children at Dharavi, Mumbai. J Community Dent Oral Epidemio. 1994;22:62–3. doi: 10.1111/j.1600-0528.1994.tb01572.x. [DOI] [PubMed] [Google Scholar]
- 5.Antia FE. The dental caries experience of school going children in the City of Bombay. J Indian Dent Assoc. 1962;39:325. [Google Scholar]
- 6.Shourie KL. Dental Caries in Indian Children. Ind J Medical Res. 1941;29:709–21. [Google Scholar]
- 7.Oral Health. ICMR Bulletin. 1994 (Apr)24:4. [Google Scholar]
- 8.Oral Health Survey Basic Methods. 4th edition 1997. [Google Scholar]
- 9.Saravanan S, Madivanan I, Subashini B, Felix JW. Prevalence pattern of dental caries in the primary dentition among school children. Indian J Dent Res. 2005;16:140–6. doi: 10.4103/0970-9290.29907. [DOI] [PubMed] [Google Scholar]
- 10.Frencken J, Manji F, Mosha H. Dental caries prevalence amongst 12-year-old urban children in East Africa. Community Dent Oral Epidemiol. 1986;14:94–8. doi: 10.1111/j.1600-0528.1986.tb01505.x. [DOI] [PubMed] [Google Scholar]
- 11.Prepared for the Food and Nutrition Board. Washington DC: National Academy of Science-National Research Council; 1952. A survey of the literature of dental caries. [Google Scholar]
- 12.Sarkar S N. Dental condition in India. Calcutta Med J. 1939;35:369. [Google Scholar]
- 13.Kulkami SS, Deshpande SD. Caries prevalence and treatment needs in 11-15 year old children of Belgaum city. J Indian Soc Pedod Prev Dent. 2002;20:12–5. [PubMed] [Google Scholar]
- 14.Dash JK, Sahoo PK, Bhuyan SK, Sahoo SK. Prevalence of dental caries and treatment needs among children of Cuttack (Orissa) J Indian Soc Pedo Prev Dent. 2002;20:139–43. [PubMed] [Google Scholar]
- 15.Rao A, Sequeira SP, Peter S. Prevalence of dental caries among school children of Moodbidri. J Indian Soc Pedod Prev Dent. 1999;17:45–8. [PubMed] [Google Scholar]
- 16.El Tayeb Y, Bratthall D, Carlsson P. Dental caries and streptococcus mutans in Suanese school children. Odontostomatol Trop. 1985;8:77–80. [PubMed] [Google Scholar]
- 17.King JD. Dental caries in Lewis and parts of West Ross-shire. Lancet. 1938;235:109. [Google Scholar]
- 18.Ainsworth NJ, Young M. The incidence of dental disease in children, London. Spec. Rep. Ser., Med. Res. Council. II. 1925 [Google Scholar]