

Abstract
Rehabilitation of a patient with severely worn dentition after restoring the vertical dimension is a complex procedure and assessment of the vertical dimension is an important aspect in these cases. This clinical report describes the full mouth rehabilitation of a patient who was clinically monitored to evaluate the adaptation to a removable occlusal splint to restore vertical dimension for a period 1 month and provisional restorations to determine esthetic and functional outcome for a period of 3 months. It is necessary to recognizing that form follows function and that anterior teeth play a vital role in the maintenance of oral health. Confirmation of tolerance to changes in the vertical dimension of occlusion (VDO) is of paramount importance. Articulated study casts and a diagnostic wax-up can provide important information for the evaluation of treatment options. Alteration of the VDO should be conservative and should not be changed without careful consideration.
Keywords: Crown lengthening, dental prosthesis, full mouth reconstruction, gingivectomy, removable appliance
Introduction
The wear of occlusal surfaces of natural teeth is a process that takes place during the lifetime of a person. In vivo research data shows that natural enamel wears about 30 μm/year or about 0.3 mm in 10 years. Excessive occlusal wear can result in pulpal pathology, occlusal disharmony, impaired function and esthetic disfigurement.[1] Therefore, it is important to identify the factors that contribute to excessive wear and evaluate alteration of the vertical dimension of occlusion (VDO) caused by the worn dentition.[2] In many cases, the VDO is maintained by tooth eruption and alveolar bone growth. Therefore, alteration of the VDO should be conservative and should not be changed without careful consideration.[3,4] However, the rehabilitation of the severely worn dentition is challenging when the space for restoration is not sufficient.
This clinical report describes the treatment of a patient who was clinically monitored to evaluate the adaptation to a removable occlusal splint during a 1 month trial period and provisional restorations for 3 months.
Case Report
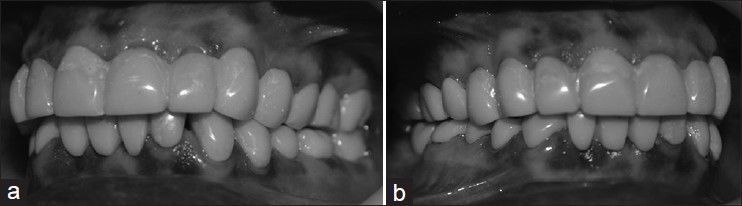
A 45-year-old man reported for the treatment of his severely worn dentition and his chief complaint was that he could not eat anything because his teeth were worn too much, were hypersensitive and had an unesthetic appearance. Patient had no relevant medical history. Intraoral examination revealed a generalized loss of tooth structure that was greater in the maxillary anteriors and mandibular posteriors. Mandibular canines, left lateral incisor and first premolars were severely worn [Figure 1a–c]. Maxillary left first molar was grossly decayed. The anterior teeth had sharp enamel edges, dentinal craters and attritional wear due to the loss of posterior support. 26, 47, 42, 41 and 31 were missing [Figure 2]. The facial type of patient was square and his lip was hypertonic. Patient did not have temporomandibular disorders, but a discrepancy between centric occlusion (CO) and maximum intercuspal position was found when she was guided to centric relation (CR) with bimanual technique.
Figure 1.
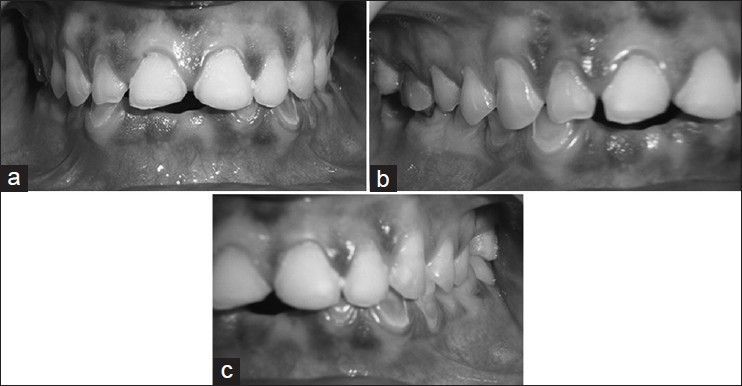
Initial oral examination. (a-c) Left lateral, frontal and right lateral views
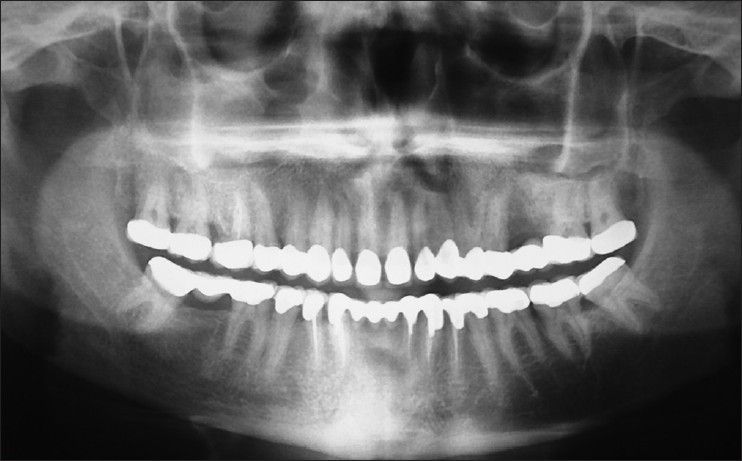
Figure 2.
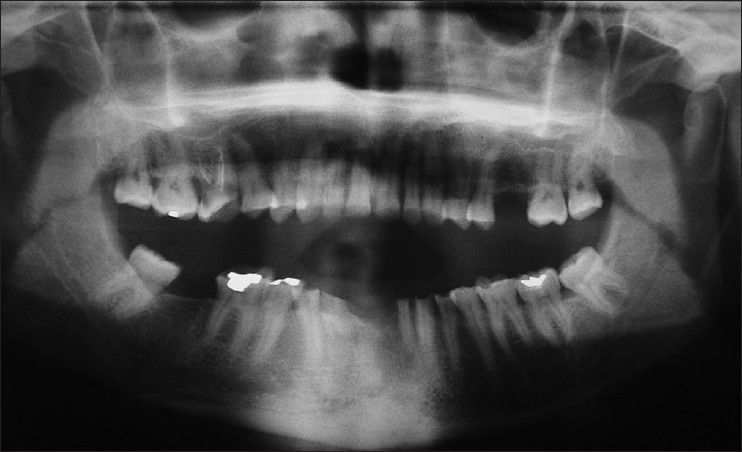
Pre-operative orthopantomogram
To determine whether VDO had been altered, the following aspects were investigated.[5]
History of wear: Physiologic wear can be compensated by tooth eruption in general, but accelerated wear may exceed the rate of eruption. The patient liked vegetables and acidic fruits and her favourite food was tough and fibrous
Phonetic evaluation: If the distance between the incisal edge of the mandibular incisors and lingual surface of the maxillary incisors is about 1 mm, the patient is able to pronounce “s” normally. The patient's increased space altered the “s” sound to “sh”
Interocclusal rest space: The patient's interocclusal rest space that was measured to be 5-6 mm. This was greater than the normal value of 2-4 mm
Facial appearance: Wrinkles and drooping commissures around the mouth were observed
The possible causes of patient's worn dentition might include posterior interferences, parafunction, eating habit and dental ignorance.
Treatment options
The options presented to the patient were removable partial dentures and full mouth rehabilitation with metal ceramic restoration with or without crown lengthening procedure and implant retained replacement of missing teeth. The patient was anxious about implant surgery, so this option was excluded. As there was clinical evidence of reduced VDO, full mouth rehabilitation with increasing VDO was planned.
Treatment planning
Pre-treatment phase
Patient's casts were mounted on a semi-adjustable articulator (Hanau™ Modular Articulator; Whip Mix Corp., Louisville, USA) using a face-bow record and an interocclusal record was made with the aid of a lucia jig and polyvinylsiloxane occlusal registration material (Exabite II; GC Corp., Tokyo, Japan).
Vertical dimension at rest was found to be 68 mm by using facial measurements after swallowing and relaxing and was verified using phonetics. VDO was found to be 61 mm using Niswonger's and Thomson's technique. Freeway space was 7 mm.
The existing VDO was increased by 4 mm using the incisal guidance pin of the articulator to a new VDO of 65 mm. The splint was designed to offer bilateral contacts of all posterior teeth in CR and guide the anterior teeth in excursive movements. The anterior guidance disoccluded the posterior teeth in all jaw positions except CR.
The adaptation of the patient to the increased VDO was evaluated during a 1 month period using the orthodontic appliance. No muscle tenderness or temporomandibular discomfort was found. Increasing the VDO was mandatory to allow the condyles to assume their most SAM position in intimate contact with the thinnest part of biconcavity of disc. It permitted the entire temporomandibular joint (TMJ) complex to attain an improved functional health and allowed the posterior avoidance patterns of occlusion to wane and a new vertical dimension to be established.
After recording the CR using lucia jig and wax-rim, diagnostic wax-up was performed.
Diagnostic Provisionalization
Autopolymerizing acrylic resin (Alike™; GC America, Alsip, USA) provisional crowns were fabricated using a vacuum formed matrix (Drufolen H; Dreve Dentamid GmbH, Unna, Germany) on a cast using indirect technique that was duplicated from the cast with the diagnostic wax-up.
Initial preparation
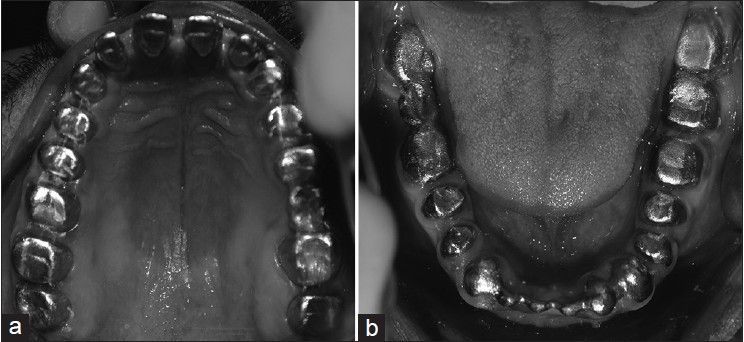
The simultaneous arch technique was employed for rehabilitation. All existing teeth were prepared to accept full veneer metal ceramic restorations with equigingival chamfer margins [Figure 3a and b].
Figure 3.
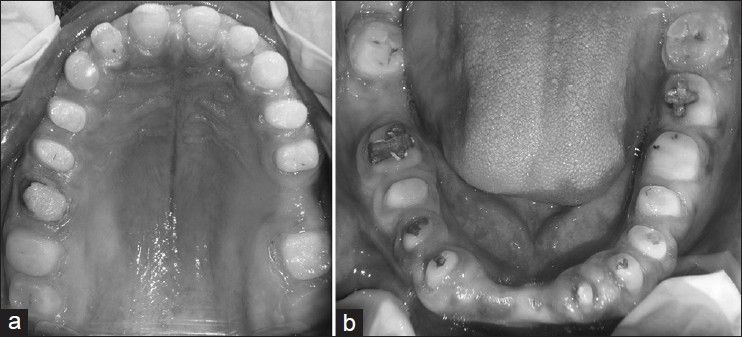
(a,b) Teeth prepared in maxillary and mandibular arch
The provisional fixed restorations were cemented with temporary cement (Freegenol Temporary Pack; GC Corp., Tokyo, Japan) and esthetics and emergence profile was evaluated. It was noticed that the crown height was insufficient and the patient had a gummy smile. It was decided that the gingiva needed recontouring. The maxillary and mandibular provisional were temporarily removed. The gingival zenith of maxillary and mandibular anteriors were evened horizontally and leveled using gingivectomy and gingivoplasty[6] [Figure 4a and b].
Figure 4.
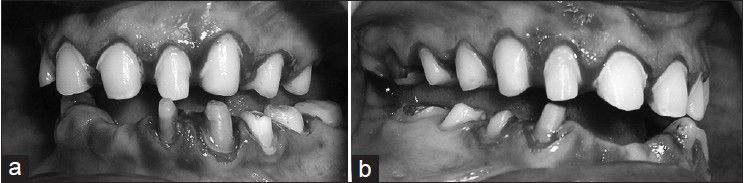
Gingivectomy for crown lengthening, (a) right lateral (b) left lateral
Final preparation
The maxillary and mandibular anterior teeth preparations were redefined in harmony with the altered gingival margins 1 week after gingival recontouring.
Final provisionalization
The final provisional restorations were fabricated from autopolymerizing acrylic resin (Alike™; GC America, Alsip, USA) using the direct-indirect technique. The provisional restorations were cemented with temporary cement (Freegenol Temporary Pack; GC Corp., Tokyo, Japan) and the patient's adaptation was monitored [Figure 5a and b].
Figure 5.
Luted final provisional restorations, (a) right lateral (b) left lateral
Interim restorations were observed for 3 months and used as a guide for definitive oral rehabilitation. During this period, the patient's condition and functions, such as muscle tenderness, discomfort of TMJ, mastication, range of the mandibular movements, swallowing and speech, were evaluated. Improvement in mastication, speech and facial esthetics confirmed the patient's tolerance to the new mandibular position with the restored VDO.
Bite registration was performed using occlusal registration material (StoneBite; Dreve Dentamid GmbH, Unna, Germany) by first removing the provisionals on the right side of the arch while maintaining the provisionals on the left side of the arch and vice-versa. Definitive impressions were made with polyvinylsiloxane impression material (Extrude; Kerr Corp., Romulus, Germany). After 1 week, metal trial was done [Figure 6a and b] and porcelain fused to metal restorations were fabricated using a customized anterior guide table, utilizing the duplicated provisional restoration casts and cemented with resin modified glass ionomer cement (FujiCEM; GC America, Alsip, USA)[7] [Figure 7a–c and an orthopantomogram was obtained [Figure 8]. Because the patient's anterior guidance table was used in the production of definitie restoration, the amount of occlusal adjustment on the lingual surface of maxillary anterior teeth was minimal. The prostheses were designed using mutually protected occlusion. The anterior teeth protected the posterior teeth from excessive force and wear and the posterior teeth supported the bite force in CO. Oral hygiene instruction were given and regular reviews were scheduled. Three reviews were completed in a period of 6 months.
Figure 6.
Metal trial (a) maxillary occlusal view (b) mandibular occlusal view
Figure 7.
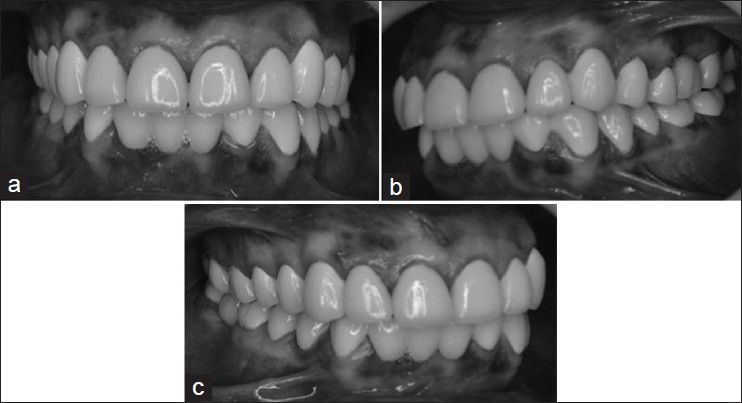
Definitive restorations were luted. (a) frontal view, frontal and right lateral view, (b) left lateral, (c) right lateral
Figure 8.
Post-operative orthopantomogram
Discussion
Full-mouth reconstructions involving full arch preparations, impressions, provisional restorations and master casts are regarded as simultaneous reconstructions. A variety of techniques may be used in simultaneous constructions to obtain complete arch dies and mounted casts. These techniques assist in concomitant laboratory construction of the units. When all of the prepared teeth are on a single articulator, there is flexibility in developing the occlusal plane, occlusal theme, embrasures, crown contour and esthetics. The chairside disadvantages include arduous, unpredictable patient visits, full arch anesthesia, full arch chairside treatment restorations, multiple occlusal records and possible loss of the VDO. Miscellaneous disadvantages are (1) the need for accurate cross-arch multiple tooth impressions and/or (2) the need for transfer techniques to fabricate full arch working casts. An alternative approach to the full-mouth simultaneous reconstruction is to complete one quadrant before beginning another. The advantages of this approach are that it is primarily chairside and includes preparation and final impressions of select teeth, maintenance of vertical dimension, quadrant anesthesia and shorter, predictable appointments. The disadvantages of the quadrant reconstruction include restrictions for achieving ideal occlusion when altering the vertical dimension, occlusal plane and embrasure development. The existing opposing dentition limits the reconstruction of an isolated quadrant. Esthetic consistency can be compromised because the porcelain restorations are made in stages. The advantages of the simultaneous and quadrant full-mouth reconstruction are combined in the present technique. The heat-processed treatment restorations are the key factors in providing both clinical and laboratory advantages. They closely resemble the final restorations while maintaining vertical and CR, minimizing the need for multiple and complicated occlusal records. Treatment restorations also provide a stable and esthetic interim prosthesis during the fabrication of the final restoration and allow appraisal of an altered VDO. The cost and laboratory time involved in fabricating the processed acrylic resin temporary restorations are a limitation, but the complexity of the patient's treatment warrants the extra effort.[5,6,7]
In 1984, Turner and Missirlian[1] classified the treatment of a severely worn dentition by the amount of the loss of VDO and available space to restore. His classification and conventional treatment, which includes raising VDO with multiple crown-lengthening procedures, have been widely used. The occlusal splint, which is reversible and conservative in nature, has been used as a diagnostic tool to judge adaptation to the altered VDO. The waiting period to judge adaptability is between 3 weeks and 5 months for the occlusal splint and 2-6 months for the provisional prosthesis.[1,3,8] In this case, the patient was carefully monitored for 1 month to evaluate the adaptation to the removable occlusal splint.[8] Furthermore, the patient's adaptation to the provisional restoration was monitored for 3 months. Discomfort, wear and muscle fatigue were not observed during this period. The increase of VDO was determined by standardized esthetic golden proportion of anterior teeth and also by patient's factors like interocclusal rest space and speech. If the increase of VDO was decided arbitrarily without close evaluation, multiple complications could arise. Depending on the patient's situation and adaptability, the interim period can be modified. In this case, the following principles were governed the gingiectomy: The gingival zenith points lie distal to the long axis of the maxillary centrals and cuspids, the zenith points of the maxillary laterals and mandibular incisors are coincident with their long axes, the gingival margins of the maxillary centrals and cuspids are apical to that of the laterals.[9,10]
Principles governing the design of porcelain fused to metal restoration:[11,12,13]
The occlusal plane was made parallel to interpupillary line
The lips were individually evaluated for symmetry and fullness
The lip position at rest was evaluated for proper lip contact as well as for the range of lip mobility when smiling
The amount of incisal display when the lips and lower jaw are in rest position was limited to 1.91 mm
The dental midline was made to be perpendicular to incisal plane and parallel or coincident to the midline of the face. The midline of the nose, forehead, interpupillary plane, philtrum and chin can be useful guides to assess the midline of face in relation to the dental midline
Negative space for the buccal corridor was incorporated to impart depth to the smile
The proportions of the maxillary six anterior teeth were designed according to the principles of golden proportion in dentistry
Good adaptation of the pontic to the ridge ensured there is no air escape through the tissue surface of the pontic while speaking, especially during the production of sibilants causing faulty phonation
Based on previous studies contact points were established in our case.
Conclusion
An ideal esthetic treatment plan attempts to achieve perfection in every way. It is important to review a range of treatment options to achieve an esthetic smile while maintaining a healthy oral environment. Recognizing that form follows function and that anterior teeth play a vital role in the maintenance of oral health is paramount. In this clinical report, raising VDO using a removable occlusal splint followed by fixed provisionals based on accurate diagnosis ensured successful full mouth rehabilitation for a severely worn dentition.
Clinical Significance
Management of worn dentition using fixed or removable prostheses is complex and among the most difficult to rehabilitate. Assessment of the vertical dimension is important and a comprehensive treatment plan is required for each individual case. Articulated study casts and a diagnostic wax-up can provide important information for the evaluation of treatment options. In this case, tolerance to changes in VDO was confirmed with clinical evaluation of the patient after having worn a diagnostic splint and provisional prosthesis.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984;52:467–74. doi: 10.1016/0022-3913(84)90326-3. [DOI] [PubMed] [Google Scholar]
- 2.Prasad S, Kuracina J, Monaco EA., Jr Altering occlusal vertical dimension provisionally with base metal onlays: A clinical report. J Prosthet Dent. 2008;100:338–42. doi: 10.1016/S0022-3913(08)60230-9. [DOI] [PubMed] [Google Scholar]
- 3.Jahangiri L, Jang S. Onlay partial denture technique for assessment of adequate occlusal vertical dimension: A clinical report. J Prosthet Dent. 2002;87:1–4. doi: 10.1067/mpr.2002.120845. [DOI] [PubMed] [Google Scholar]
- 4.Dawson PE. From TMJ to Smile Design. 1st ed. New York: Elsevier Inc.; 2008. [Google Scholar]
- 5.Kar AK, Parkash H, Jain V. Full-mouth rehabilitation of a case of generalized enamel hypoplasia using a twin-stage procedure. Contemp Clin Dent. 2010;1:98–102. doi: 10.4103/0976-237X.68601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Banerjee S, Chakraborty N, Singh R, Gupta T. Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure. Contemp Clin Dent. 2012;3:103–7. doi: 10.4103/0976-237X.94558. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 7.Dawson PE. Functional Occlusion: From TMJ to Smile Design. 1st ed. New York: Elsevier Inc.; 2008. pp. 430–52. [Google Scholar]
- 8.Ganddini MR, Al-Mardini M, Graser GN, Almog D. Maxillary and mandibular overlay removable partial dentures for the restoration of worn teeth. J Prosthet Dent. 2004;91:210–4. doi: 10.1016/j.prosdent.2003.12.021. [DOI] [PubMed] [Google Scholar]
- 9.Hempton TJ, Dominici JT. Contemporary crown-lengthening therapy: A review. J Am Dent Assoc. 2010;141:647–55. doi: 10.14219/jada.archive.2010.0252. [DOI] [PubMed] [Google Scholar]
- 10.Hoyle DE. Fabrication of a customized anterior guide table. J Prosthet Dent. 1982;48:490–1. doi: 10.1016/0022-3913(82)90089-0. [DOI] [PubMed] [Google Scholar]
- 11.Brown KE. Reconstruction considerations for severe dental attrition. J Prosthet Dent. 1980;44:384–8. doi: 10.1016/0022-3913(80)90094-3. [DOI] [PubMed] [Google Scholar]
- 12.Sato S, Hotta TH, Pedrazzi V. Removable occlusal overlay splint in the management of tooth wear: A clinical report. J Prosthet Dent. 2000;83:392–5. doi: 10.1016/s0022-3913(00)70032-1. [DOI] [PubMed] [Google Scholar]
- 13.Davis NC. Smile design. Dent Clin North Am. 2007;51:299–318. doi: 10.1016/j.cden.2006.12.006. [DOI] [PubMed] [Google Scholar]