

Abstract
Purpose: Prescription of ketotifen as an effective antihistamine in asthma and allergic conditions is associated with side effect of weight gain. Caffeine is an agent which increases thermogenesis and improves energy expenditure and also effective in asthma. The aim of current study was to evaluate caffeine impact in reducing weight gain side effect of ketotifen.
Methods: Male mice at the weight limit of 20-30 gr in 8 groups were randomly chosen and injected following drug dosages for 45 days intraperitoneally: control group (normal saline 10 ml/kg), three groups of ketotifen (4, 8, 16 mg/kg), three groups of caffeine (4, 8, 16 mg/kg) and one group of ketotifen (4 mg/kg) in combination with caffeine (4 mg/kg). Weight changes have been recorded and assessed every 3 days for 45 days.
Results: The results showed that in all dosages of the two drugs, significant weight loss occurred in comparison with the control group.
Conclusion: The effect of caffeine on weight loss according to our results, matches with human studies, while ketotifen contradictory to our assumption, resulted in weight loss which probably was related to the difference in metabolic pathways in mice and humans, or maybe the used doses of ketotifen in this study were insufficient to reduce TNF-α production or influence in serotonin release and be effective on appetite or weight gain.
Keywords: Ketotifen, Caffeine, Appetite, Weight changes, Mice
Introduction
According to World Health Organization (WHO) report in 2013, overweight and obesity are the fifth leading risks for global death, as there is a strong scientific agreement that obesity significantly increases the risk of serious chronic diseases like hypertension and cardiovascular disease, diabetes, obstructive sleep apnea and some forms of cancer and finally contributes to overall mortality.1,2 Weight gain occurrence, due to genetic predisposition or result from lifestyle and intake of calories more than needed or as a side effect of some medications; interventions should be done to combat this epidemic problem.
Ketotifen, is a safe anti-histamine with low dose and long-lasting effects, which inhibits release of mediators involved in asthma and allergies. Its primary pharmacological roles are histamine receptor antagonism, phosphodiesterase inhibition and prevention of calcium flux in smooth muscles. Distinctive anti-asthmatic properties of ketotifen which make it a suitable and effective treatment in asthma include: preventative effect on airway hyperreactivity associated with activation of platelets by PAF (Platelet Activating Factor) or caused by sympathomimetic drugs or the exposure to allergen; inhibition of eosinophils and platelets in the airways; suppression of the influx of eosinophils into inflammatory local and antagonism of bronchoconstriction due to leukotrienes.3 Ketotifen, like most antihistamines not only sedates and slows down body metabolism, but also can stimulate appetite and induce weight-gain.4,5 Specially ketotifen causes a significant weight gain in children with asthma,6 maybe as a chronic state of this disease and the long duration of drug use in asthma. Besides the prolonged use, the other effective factor in weight gain of these patients is the simultaneous use with corticosteroids which are prescribed in asthma and have weight gain effect due to their induced edema and mechanism of action. Thereby the weight gain incidence practically is higher in ketotifen-received asthmatic patients and it is tried to overcome this side effect by use of different agents as like as essential oils.7 Considering this effect of ketotifen few studies performed to make use of this side effect in a positive way in catechia. As a result of these studies, it is concluded that, ketotifen could be useful in the management of HIV-associated malnutrition by inhibition of release of TNF-alpha from stimulated peripheral blood mononuclear cells.8 Also due to this side effect, in some researches it has been used as an agent to induce weight gain.7,9
Caffeine is a methyl-xanthine with brain stimulant effect which unlike ketotifen increases alertness and concentration, and is considered as a stimulant of energy expenditure which can increase thermogenesis and fat oxidation,10 and can alter the energy balance by improving energy consumption. Clinical applications of caffeine have been reviewed in 1995.11 There are some evidence suggesting a positive effect of methyl-xanthine especially caffeine, in several diseases such as parkinsonism,12,13 asthma,14 apnea,15 cancer,16 diabetes17 and in migraine as an adjunctive analgesic in combination with ergotamine.18,19 Furthermore, it may be added to a variety of analgesics and some antiviral drugs.20 Different studies regarding the effects of caffeine-induced weight loss and energy expenditure are available.21-30 As it was pointed by Curatolo et al., caffeine appeared to be safe in regular used dosages, and can be considered as a useful agent to induce thermogenesis and lose weight.31,32 Thereby, epidemiological data suggest that increasing caffeine consumption may lead to a small reduction in long-term weight gain.29,33,34
Combinations of different drugs as a multi-ingredient formulation are prepared to improve drug effects or to prevent exacerbation of drug side effects. In this study with considering both of these roles, the impact of caffeine (an effective agent in asthma which is a bronchodilator and also reduces respiratory muscle fatigue)35,36 in reducing body weight, individually and in co-administration with ketotifen (an effective agent in asthma and allergies), has been investigated in mice model.
Materials and Methods
Animals
Male mice at the weight limit of 20-30 g divided in 8 groups (n=8 in each group) randomly and maintained with free access to standard mice food and tap water. All steps of experiment were performed according to the Guide for the Care and Use of Laboratory Animals (National Institutes of Health Publication No 85-23, revised 1985).
Drugs
Pure powders of ketotifen fumarate and caffeine in anhydrate form were purchased from Darupaksh Pharmaceutical Company, Tehran, Iran. Sodium chloride solution (0.9 %) was used as solvent of the drugs and determined doses were injected intraperitoneal (i.p.) to the mice.
Experimental protocols
Animals treated for 45 days in one control group and seven groups of treatment with different doses of drugs. Control group received normal saline 10 ml/kg, i.p. and in drug receiving groups, there were three groups of ketotifen in concentration of 4, 8, 16 mg/kg, i.p. and three groups of caffeine in concentration of 4, 8, 16 mg/kg, i.p. and one group of caffeine 4mg/kg, i.p. in combination with ketotifen 4 mg/kg, i.p. injection. Required drug dose for each mouse was calculated based on its body weight and injected intraperitoneally for 45 consecutive days. Weight changes were recorded as body weight (BW) and assessed every three days over 45 days of experiment and the dose of drugs were adjusted every three days based on the new recorded weight of each mouse.
Statistics analysis
Data was expressed as Means± SEM for each group in different times of BW measurement. To compare group means and determine significant differences between various groups, the analysis of variance (ANOVA) was used and assessed by Tukey test. Differences were considered as significant for P<0.05.
Results
Weight changes due to different doses of ketotifen (4, 8, 16 mg/kg)
According to Figure 1, comparison of weight changes in ketotifen 4 mg/kg and control group of receiving normal saline during 45 days of experiment, showed that there were significant differences on days of 24, 28, 36, 40 and 45 (P<0.05). For the dose of 8 mg/kg of ketotifen, there were significant differences on days of 40 and 45 of experiment (P<0.05). Also in dose of 16 mg/kg of ketotifen there were statistically significant differences on days of 32 (P<0.01) and 24, 28, 40 and 45 of experiment (P<0.001).
Figure 1 .
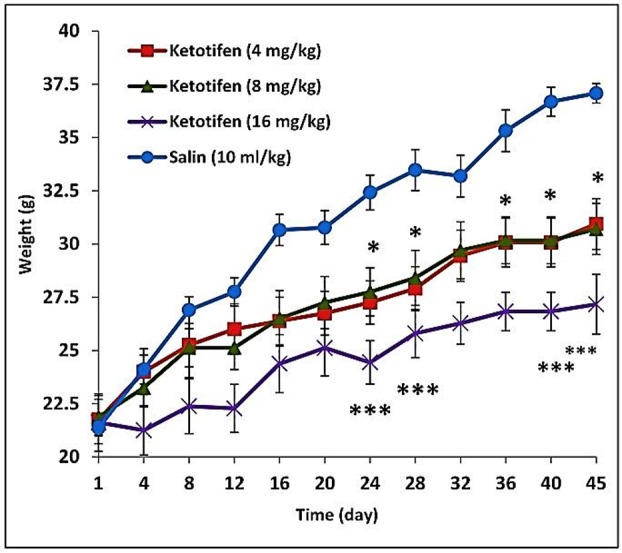
Weight changes due to different doses of ketotifen (4, 8, 16 mg/kg) in mice for 45 days. Values represent the Mean± SEM of 8 animals for each group. Significantly different from the control group; *p<0.05, **p<0.01, ***p<0.001.
Weight changes due to different doses of caffeine (4, 8, 16 mg/kg)
Comparison of weight change in groups receiving various doses of caffeine compared to control group, showed that there were significant differences, for 4 mg/kg of caffeine on 40 and 45th day of experiment (P<0.05) and in dose of 8 mg/kg of caffeine in 24 and 40th day (P<0.05) and 45th day (P<0.01) of the study. For higher dose of caffeine (16 mg/kg) there were statistically significant differences on days of 28, 32 (P<0.05) and 36, 40 and 45th of the study (P<0.01) (Figure 2).
Figure 2 .
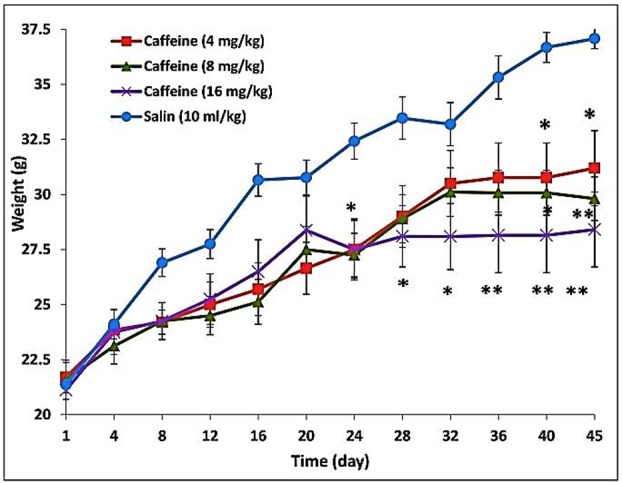
Weight changes due to different doses of caffeine (4, 8, 16 mg/kg) in mice for 45 days. Values represent the Mean± SEM of 8 animals for each group. Significantly different from the control group; *p<0.05, **p<0.01.
Weight changes due to co-administration of ketotifen (4 mg/kg) and caffeine (4 mg/kg)
Weight changes due to co-administration of ketotifen (4 mg/kg) and caffeine (4 mg/kg) in comparison with control group (normal saline 10 ml/kg) showed significant differences, on days of 28, 36, 40 (P<0.01) and 32 and 45 of experiment (P<0.05) (Figure 3). However the effect of co-administration is not significantly different with either single drug of ketotifen or caffeine in dose of 4 mg/kg.
Weight changes due to administration of same dose of the two drugs of ketotifen and caffeine
According to the diagrams in Figure 4 which compare weight changes in same dose of ketotifen and caffeine, there was no significant difference in any doses of 4, 8 and 16 mg/kg. However each dose of ketotifen and caffeine in comparison with control group had caused significant weight loss.
Discussion
The results of present study showed that, the injection of different doses of ketotifen and caffeine induced significant weight loss in comparison with control group. To interpret the result obtained from this study, we should concentrate on mechanism of action of these drugs.
Caffeine (1,3,7-trimethylxanthine), is the major pharmacologically active methylxanthine in coffee and tea.37 The predominate mechanism of its action is by blocking the action of adenosine as a competitive inhibitor of A1 and A2a adenosine receptor due to the similarity in its molecular structure to the nucleotide adenosine. Consistent with this effect on adenosine receptors, caffeine also releases norepinephrine, dopamine and serotonin in the brain and increases circulating catechol amines, following stimulation of central nervous system and energy metabolism in the peripheral tissues.38,39 A small amount of caffeine inhibits presynaptic adenosine receptors and increases release of catecholamine neurotransmitters. Also in larger quantities (>10 µmol/L), inhibition of phosphodiesterase and increase in cAMP concentration ultimately leads to increase in calcium influx into cells and in doses higher than 100 µmol/L, caffeine disrupt calcium retention through reticulum sarcoplasmic in cells.40
Figure 3 .
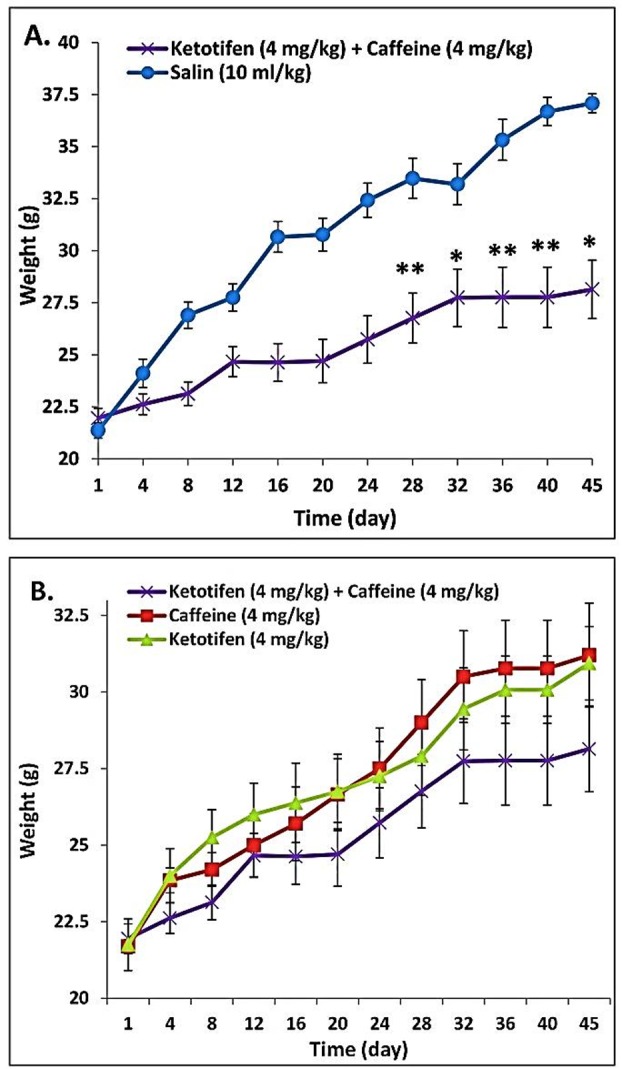
Weight changes due to co-administration of ketotifen (4 mg/kg) and caffeine (4 mg/kg) in mice for 45 days, in comparison with control group (A) and in comparison with separate dose of ketotifen (4 mg/kg) and caffeine (4 mg/kg) (B). Values represent the Mean± SEM of 8 animals for each group. Significantly different from the control group; *p<0.05, **p<0.01.
Figure 4 .
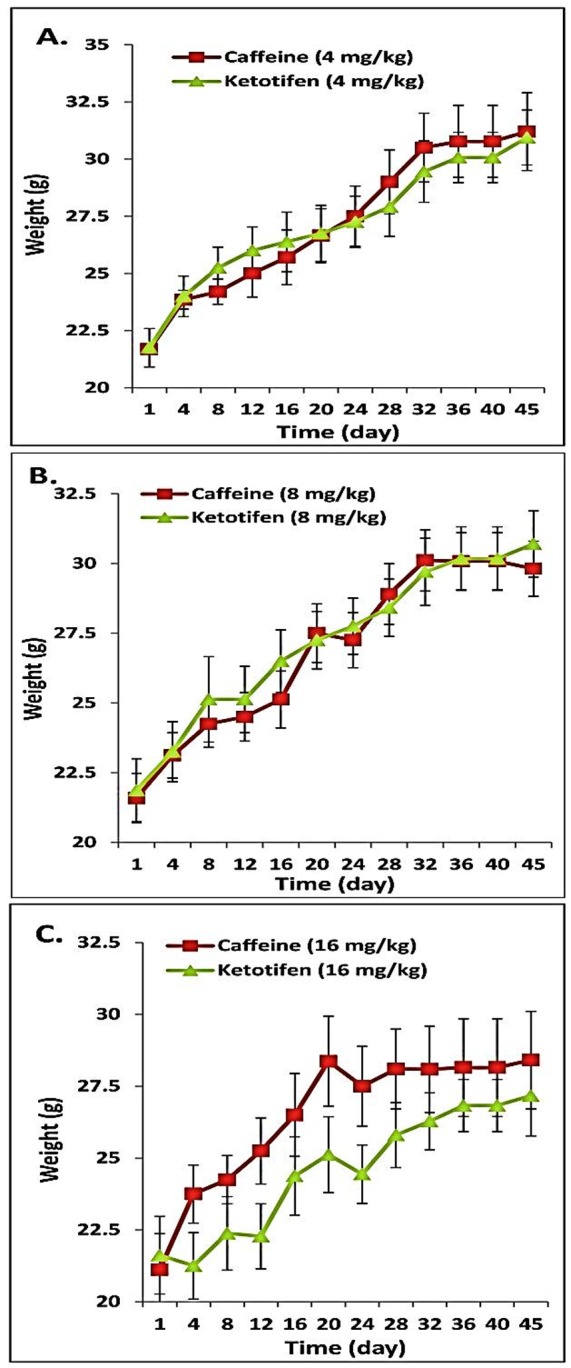
Weight changes due to administration of ketotifen (4 mg/kg) and caffeine (4 mg/kg) (A), ketotifen (8 mg/kg) and caffeine (8 mg/kg) (B), ketotifen (16 mg/kg) and caffeine (16 mg/kg) (C) in mice for 45 days. Values represent the Mean± SEM of 8 animals for each group.
Caffeine alone has several important metabolic effects. Caffeine stimulates fat utilization in muscle tissue during exercise.41 In addition, a dose-dependent increase in basal energy expenditure with caffeine is reported by Astrup et al., which exerted through an increase in lactate and triacylglycerol production and increased vascular smooth muscle tone.42 Increase in lipid turnover and lipid oxidation by interference in Cori-cycle and the FFA-triglycreride cycle and acting as a thermogenesis agent can be added to the mechanism of action of caffeine.43-45 Effect of caffeine on thermogenesis regulation was accomplished through an inhibitory effect on the enzyme phosphodiesterase. This resulted in increasing of cyclic adenosine mono phosphate (cAMP) content. Later, synaptic nerve system activity amplified and activated hormone-sensitive lipase, which promotes lipolysis.43,46
Another probable mechanism of weight loss caused by caffeine is through diuretic and natriuretic effect, which is induced by blockage of hepatic adenosine-mediated sensory nerves and hepatorenal reflex.47 There is evidence that moderate caffeine intake might be useful in preventing obesity by inhibiting proliferative activity in white adipose tissue.48 It is also suggested that the anti-obesity effect of caffeine is due to the additive and/or synergistic inhibitory activity of caffeine on intracellular lipid accumulation.49 The usual amount of caffeine increases circulating cortisol concentration, but does not have short term effects on appetite, energy intake, glucose metabolism, and inflammatory markers.50 All of the mentioned mechanisms suggest a beneficial effect of caffeine as a weight loosing agent and as a good factor to combine with some drugs with side effect of weight gain. In the same way, in this study, with use of different doses of caffeine in comparison with the control group, significant weight loss was observed, which may be due to the effect of caffeine in inducing diuresis, increasing lipolysis and basal metabolism, enhancement in mobility and reduction of feeling fatigue.
The other studied drug, ketotifen, is a second-generation noncompetitive H1-antihistamine and mast cell stabilizer which besides its anti-histaminic activity, also function as a leukotriene antagonist and a phosphodiesterase inhibitor. However, appetite stimulation and weight gain are its common side effects in human.51,52 A probable mechanism of ketotifen on weight gain and appetite is attributed to inhibitory effect on production of TNF-α which has been confirmed in human studies.8 It has been evidenced that TNF-α plays a key role in regulating energy metabolism53 and can act directly on adipocytes to regulate the release of leptin.54 Leptin acts on receptors in the hypothalamus of the brain, where it inhibits appetite.55 Ketotifen by inhibitory effect on production of TNF-α can reduce leptin level and thereby decreased the inhibition of leptin on appetite and finally result in weight gain. In addition to mentioned appetite enhancing mechanism of ketotifen, this drug by influence in 5-hydroxytryptamine regulation, could involve in central serotonin disinhibition,56 leading to decrease serotonin level and as the fact of suppressant effect of serotonin on appetite, ketotifen caused an increase in food intake tendency and appetite.
In the present study, different doses of ketotifen not only did not cause significant weight gain but also induced significant weight loss compared to the control group. The results may be due to the difference in metabolic pathways in mice and humans, or maybe the used doses of ketotifen in this study were not in the range of doses to reduce TNF-α production or influence serotonin release and be effective on appetite or weight gain, which require further studies and measuring the level of TNF-α. This contradictory effect of ketotifen is also reported in other studies. As an example, in an evaluation of combining ketotifen and oxymetholone on weight gain and performance status in human immunodeficiency virus (HIV) positive patients with chronic cachexia, addition of ketotifen did not result in weight gain57. In another study of evaluation of co-administration of ketotifen and cyproheptadine, the injection of different doses of ketotifen showed different results in mice, while the high doses of ketotifen caused a significant weight gain compared to the control group, but the low doses resulted in a significant weight loss9 which amplify the importance of doses used in research and indicate the probability of the different mechanism of different doses in variant patients.
Conclusion
According to this study and determining the separate and also combined prescription of ketotifen and caffeine on weight changes in mice, further study on exact mechanism of weight gain and effect of these drugs in these processes should be done to find the causes of weight loosing effect of ketotifen in low doses. And also measurement of the consumed food and water by animals is recommended to assess the impact of these drugs on appetite. Therefor to clarify the issue arising from different results of this study and previous works, and to attribute a new application of these drugs in the form of co-administration, it is suggested to study more in this field, maybe with higher doses or different protocol and time range. It means that maybe with higher doses of ketotifen and inducing weight gain, the combination of caffeine and ketotifen will be effective in reducing this side effect and also by the means of this combination in asthmatic patients the efficacy of ketotifen in controlling the disease symptoms can be enhanced.
Acknowledgements
The authors thank the Faculty of Pharmacy of Tabriz University of Medical Sciences, for providing technical support for this study.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- 1.Haslam DW, James WP. Obesity. Lancet . 2005;366(9492):1197–209. doi: 10.1016/S0140-6736(05)67483-1. [DOI] [PubMed] [Google Scholar]
- 2.Saito Y, Kita T, Mabuchi H, Matsuzaki M, Matsuzawa Y, Nakaya N. et al. Obesity as a risk factor for coronary events in Japanese patients with hypercholesterolemia on low-dose simvastatin therapy. J Atheroscler Thromb. 2010;17(3):270–7. doi: 10.5551/jat.2782. [DOI] [PubMed] [Google Scholar]
- 3.Thomson, Micromedex . Drug Information for the Health Care Professional. 24th ed. Greenwood Village: United States Pharmacopeial Convention, Inc; 2004. [Google Scholar]
- 4.Couluris M, Mayer JL, Freyer DR, Sandler E, Xu P, Krischer JP. The effect of cyproheptadine hydrochloride (periactin) and megestrol acetate (megace) on weight in children with cancer/treatment-related cachexia. J Pediatr Hematol Oncol. 2008;30(11):791–7. doi: 10.1097/MPH.0b013e3181864a5e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ali AH, Yanoff LB, Stern EA, Akomeah A, Courville A, Kozlosky M. et al. Acute effects of betahistine hydrochloride on food intake and appetite in obese women: a randomized, placebo-controlled trial. Am J Clin Nutr. 2010;92(6):1290–7. doi: 10.3945/ajcn.110.001586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Craps LP. Immunologic and therapeutic aspects of ketotifen. J Allergy Clin Immunol. 1985;76(2 Pt 2):389–93. doi: 10.1016/0091-6749(85)90659-1. [DOI] [PubMed] [Google Scholar]
- 7.Asnaashari S, Delazar A, Habibi B, Vasfi R, Nahar L, Hamedeyazdan S. et al. Essential oil from Citrus aurantifolia prevents ketotifen-induced weight-gain in mice. Phytother Res. 2010;24(12):1893–7. doi: 10.1002/ptr.3227. [DOI] [PubMed] [Google Scholar]
- 8.Ockenga J, Rohde F, Suttmann U, Herbarth L, Ballmaier M, Schedel I. Ketotifen in HIV-infected patients: effects on body weight and release of TNF-alpha. Eur J Clin Pharmacol. 1996;50(3):167–70. doi: 10.1007/s002280050087. [DOI] [PubMed] [Google Scholar]
- 9.Nemati M, Habibi B, Sharifi K. Effect of ketotifen and cyproheptadine on appetite and weight changes in mice. Iran J Pharm Sci. 2006;2(3):123–8. [Google Scholar]
- 10.Dulloo AG, Geissler CA, Horton T, Collins A, Miller DS. Normal caffeine consumption: influence on thermogenesis and daily energy expenditure in lean and postobese human volunteers. Am J Clin Nutr. 1989;49(1):44–50. doi: 10.1093/ajcn/49.1.44. [DOI] [PubMed] [Google Scholar]
- 11.Sawynok J. Pharmacological rationale for the clinical use of caffeine. Drugs. 1995;49(1):37–50. doi: 10.2165/00003495-199549010-00004. [DOI] [PubMed] [Google Scholar]
- 12.Carey RJ. Antiparkinsonian effects of caffeine depend upon pavlovian drug conditioning processes. Brain Res. 1990;518(1-2):186–92. doi: 10.1016/0006-8993(90)90971-d. [DOI] [PubMed] [Google Scholar]
- 13.Schwarzschild MA, Chen JF, Ascherio A. Caffeinated clues and the promise of adenosine A(2A) antagonists in PD. Neurology. 2002;58(8):1154–60. doi: 10.1212/wnl.58.8.1154. [DOI] [PubMed] [Google Scholar]
- 14.Tilley SL. Methylxanthines in asthma. Handb Exp Pharmacol. 2011;200:439–56. doi: 10.1007/978-3-642-13443-2_17. [DOI] [PubMed] [Google Scholar]
- 15.Henderson-Smart DJ, De Paoli AG. Prophylactic methylxanthine for prevention of apnoea in preterm infants. Cochrane Database Syst Rev. 2010;12:CD000432. doi: 10.1002/14651858.CD000432.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ohta A, Sitkovsky M. Methylxanthines, inflammation, and cancer: fundamental mechanisms. Handb Exp Pharmacol. 2011;200:469–81. doi: 10.1007/978-3-642-13443-2_19. [DOI] [PubMed] [Google Scholar]
- 17.Kempf K, Herder C, Erlund I, Kolb H, Martin S, Carstensen M. et al. Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial. Am J Clin Nutr. 2010;91(4):950–7. doi: 10.3945/ajcn.2009.28548. [DOI] [PubMed] [Google Scholar]
- 18.Yancey JR, Dattoli G. Caffeine as an analgesic adjuvant for acute pain in adults. Am Fam Physician. 2013;87(1):11. [PubMed] [Google Scholar]
- 19.Nieber K. [Does caffeine enhance the analgesic efficacy?] Dtsch Med Wochenschr. 2013;138(8):352. doi: 10.1055/s-0032-1329151. [DOI] [PubMed] [Google Scholar]
- 20.Jankiewicz K, Chroscinska-Krawczyk M, Blaszczyk B, Czuczwar SJ. [Caffeine and antiepileptic drugs: experimental and clinical data] Przegl Lek. 2007;64(11):965–7. [PubMed] [Google Scholar]
- 21.Striegel-Moore RH, Franko DL, Thompson D, Barton B, Schreiber GB, Daniels SR. Caffeine intake in eating disorders. Int J Eat Disord. 2006;39(2):162–5. doi: 10.1002/eat.20216. [DOI] [PubMed] [Google Scholar]
- 22.Dulloo AG. Herbal simulation of ephedrine and caffeine in treatment of obesity. Int J Obes Relat Metab Disord. 2002;26(5):590–2. doi: 10.1038/sj.ijo.0802036. [DOI] [PubMed] [Google Scholar]
- 23.Hackman RM, Havel PJ, Schwartz HJ, Rutledge JC, Watnik MR, Noceti EM. et al. Multinutrient supplement containing ephedra and caffeine causes weight loss and improves metabolic risk factors in obese women: a randomized controlled trial. Int J Obes (Lond) 2006;30(10):1545–56. doi: 10.1038/sj.ijo.0803283. [DOI] [PubMed] [Google Scholar]
- 24.Greenway FL, De Jonge L, Blanchard D, Frisard M, Smith SR. Effect of a dietary herbal supplement containing caffeine and ephedra on weight, metabolic rate, and body composition. Obes Res. 2004;12(7):1152–7. doi: 10.1038/oby.2004.144. [DOI] [PubMed] [Google Scholar]
- 25.Boozer CN, Nasser JA, Heymsfield SB, Wang V, Chen G, Solomon JL. An herbal supplement containing Ma Huang-Guarana for weight loss: a randomized, double-blind trial. Int J Obes Relat Metab Disord. 2001;25(3):316–24. doi: 10.1038/sj.ijo.0801539. [DOI] [PubMed] [Google Scholar]
- 26.Tremblay A, Masson E, Leduc S, Houde A, Després J-P. Caffeine reduces spontaneous energy intake in men but not in women. Nutr Res. 1988;8(5):553–8. [Google Scholar]
- 27.Pasman WJ, Westerterp-Plantenga MS, Saris WH. The effectiveness of long-term supplementation of carbohydrate, chromium, fibre and caffeine on weight maintenance. Int J Obes Relat Metab Disord. 1997;21(12):1143–51. doi: 10.1038/sj.ijo.0800528. [DOI] [PubMed] [Google Scholar]
- 28.Westerterp-Plantenga MS, Lejeune MP, Kovacs EM. Body weight loss and weight maintenance in relation to habitual caffeine intake and green tea supplementation. Obes Res. 2005;13(7):1195–204. doi: 10.1038/oby.2005.142. [DOI] [PubMed] [Google Scholar]
- 29.Lopez-Garcia E, Van Dam RM, Rajpathak S, Willett WC, Manson JE, Hu FB. Changes in caffeine intake and long-term weight change in men and women. Am J Clin Nutr. 2006;83(3):674–80. doi: 10.1093/ajcn.83.3.674. [DOI] [PubMed] [Google Scholar]
- 30.Hursel R, Viechtbauer W, Westerterp-Plantenga MS. The effects of green tea on weight loss and weight maintenance: a meta-analysis. Int J Obes (Lond) 2009;33(9):956–61. doi: 10.1038/ijo.2009.135. [DOI] [PubMed] [Google Scholar]
- 31.Curatolo PW, Robertson D. The health consequences of caffeine. Ann Intern Med. 1983;98(5 Pt 1):641–53. doi: 10.7326/0003-4819-98-5-641. [DOI] [PubMed] [Google Scholar]
- 32.Westerterp-Plantenga MS. Green tea catechins, caffeine and body-weight regulation. Physiol Behav. 2010;100(1):42–6. doi: 10.1016/j.physbeh.2010.02.005. [DOI] [PubMed] [Google Scholar]
- 33.Dalbo VJ, Roberts MD, Stout JR, Kerksick CM. Effect of gender on the metabolic impact of a commercially available thermogenic drink. J Strength Cond Res. 2010;24(6):1633–42. doi: 10.1519/JSC.0b013e3181db9bbd. [DOI] [PubMed] [Google Scholar]
- 34.Hursel R, Westerterp-Plantenga MS. Thermogenic ingredients and body weight regulation. Int J Obes (Lond) 2010;34(4):659–69. doi: 10.1038/ijo.2009.299. [DOI] [PubMed] [Google Scholar]
- 35.Welsh EJ, Bara A, Barley E, Cates CJ. Caffeine for asthma. Cochrane Database Syst Rev. 2010;1:CD001112. doi: 10.1002/14651858.CD001112.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bara AI, Barley EA. Caffeine for asthma. Cochrane Database Syst Rev. 2000;2:CD001112.. doi: 10.1002/14651858.CD001112. [DOI] [PubMed] [Google Scholar]
- 37.Nehlig A. Coffee, tea, chocolate, and the brain. Boca Raton, Florida: CRC Press; 2004. [Google Scholar]
- 38.Benowitz NL. Clinical pharmacology of caffeine. Annu Rev Med. 1990;41:277–88. doi: 10.1146/annurev.me.41.020190.001425. [DOI] [PubMed] [Google Scholar]
- 39.Nehlig A, Daval JL, Debry G. Caffeine and the central nervous system: mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res Brain Res Rev. 1992;17(2):139–70. doi: 10.1016/0165-0173(92)90012-b. [DOI] [PubMed] [Google Scholar]
- 40.Snyder SH. Adenosine receptors and the actions of methylxanthines. Trends Neurosci. 1981;4(0):242–4. [Google Scholar]
- 41.Spriet LL, Maclean DA, Dyck DJ, Hultman E, Cederblad G, Graham TE. Caffeine ingestion and muscle metabolism during prolonged exercise in humans. Am J Physiol. 1992;262(6 Pt 1):E891–8. doi: 10.1152/ajpendo.1992.262.6.E891. [DOI] [PubMed] [Google Scholar]
- 42.Astrup A, Toubro S, Cannon S, Hein P, Breum L, Madsen J. Caffeine: a double-blind, placebo-controlled study of its thermogenic, metabolic, and cardiovascular effects in healthy volunteers. Am J Clin Nutr. 1990;51(5):759–67. doi: 10.1093/ajcn/51.5.759. [DOI] [PubMed] [Google Scholar]
- 43.Acheson KJ, Gremaud G, Meirim I, Montigon F, Krebs Y, Fay LB. et al. Metabolic effects of caffeine in humans: lipid oxidation or futile cycling? Am J Clin Nutr. 2004;79(1):40–6. doi: 10.1093/ajcn/79.1.40. [DOI] [PubMed] [Google Scholar]
- 44.Westerterp-Plantenga M, Diepvens K, Joosen AM, Berube-Parent S, Tremblay A. Metabolic effects of spices, teas, and caffeine. Physiol Behav. 2006;89(1):85–91. doi: 10.1016/j.physbeh.2006.01.027. [DOI] [PubMed] [Google Scholar]
- 45.Diepvens K, Westerterp KR, Westerterp-Plantenga MS. Obesity and thermogenesis related to the consumption of caffeine, ephedrine, capsaicin, and green tea. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R77–85. doi: 10.1152/ajpregu.00832.2005. [DOI] [PubMed] [Google Scholar]
- 46.Cornelis MC, El-Sohemy A, Campos H. Genetic polymorphism of the adenosine A2A receptor is associated with habitual caffeine consumption. Am J Clin Nutr. 2007;86(1):240–4. doi: 10.1093/ajcn/86.1.240. [DOI] [PubMed] [Google Scholar]
- 47.Ming Z, Lautt WW. Caffeine-induced natriuresis and diuresis via blockade of hepatic adenosine-mediated sensory nerves and a hepatorenal reflex. Can J Physiol Pharmacol. 2010;88(11):1115–21. doi: 10.1139/y10-090. [DOI] [PubMed] [Google Scholar]
- 48.Bukowiecki LJ, Lupien J, Follea N, Jahjah L. Effects of sucrose, caffeine, and cola beverages on obesity, cold resistance, and adipose tissue cellularity. Am J Physiol. 1983;244(4):R500–7. doi: 10.1152/ajpregu.1983.244.4.R500. [DOI] [PubMed] [Google Scholar]
- 49.Nakabayashi H, Hashimoto T, Ashida H, Nishiumi S, Kanazawa K. Inhibitory effects of caffeine and its metabolites on intracellular lipid accumulation in murine 3T3-L1 adipocytes. Biofactors. 2008;34(4):293–302. doi: 10.3233/BIO-2009-1083. [DOI] [PubMed] [Google Scholar]
- 50.Gavrieli A, Yannakoulia M, Fragopoulou E, Margaritopoulos D, Chamberland JP, Kaisari P. et al. Caffeinated coffee does not acutely affect energy intake, appetite, or inflammation but prevents serum cortisol concentrations from falling in healthy men. J Nutr. 2011;141(4):703–7. doi: 10.3945/jn.110.137323. [DOI] [PubMed] [Google Scholar]
- 51.Phillips MJ, Meyrick Thomas RH, Moodley I, Davies RJ. A comparison of the in vivo effects of ketotifen, clemastine, chlorpheniramine and sodium cromoglycate on histamine and allergen induced weals in human skin. Br J Clin Pharmacol. 1983;15(3):277–86. doi: 10.1111/j.1365-2125.1983.tb01500.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Katzung BG. Basic & clinical pharmacology. 9th ed. Katzung BG, editor. New York: Lange Medical Books/McGraw Hill; 2004. [Google Scholar]
- 53.Sethi JK, Hotamisligil GS. The role of TNF alpha in adipocyte metabolism. Semin Cell Dev Biol. 1999;10(1):19–29. doi: 10.1006/scdb.1998.0273. [DOI] [PubMed] [Google Scholar]
- 54.Kirchgessner TG, Uysal KT, Wiesbrock SM, Marino MW, Hotamisligil GS. Tumor necrosis factor-alpha contributes to obesity-related hyperleptinemia by regulating leptin release from adipocytes. J Clin Invest. 1997;100(11):2777–82. doi: 10.1172/JCI119824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Henry BA, Goding JW, Alexander WS, Tilbrook AJ, Canny BJ, Dunshea F. et al. Central administration of leptin to ovariectomized ewes inhibits food intake without affecting the secretion of hormones from the pituitary gland: evidence for a dissociation of effects on appetite and neuroendocrine function. Endocrinology. 1999;140(3):1175–82. doi: 10.1210/endo.140.3.6604. [DOI] [PubMed] [Google Scholar]
- 56.Aguilera A, Selgas R, Codoceo R, Bajo A. Uremic anorexia: a consequence of persistently high brain serotonin levels? The tryptophan/serotonin disorder hypothesis. Perit Dial Int. 2000;20(6):810–6. [PubMed] [Google Scholar]
- 57.Hengge UR, Baumann M, Maleba R, Brockmeyer NH, Goos M. Oxymetholone promotes weight gain in patients with advanced human immunodeficiency virus (HIV-1) infection. Br J Nutr. 1996;75(1):129–38. doi: 10.1079/bjn19960116. [DOI] [PubMed] [Google Scholar]